National Trauma Data Bank Report 2006 Version 6.0 American College of Surgeons National Trauma Data Bank® 2006, Version 6.0
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Savings Plus OA Managed Choice® POS Network Overview
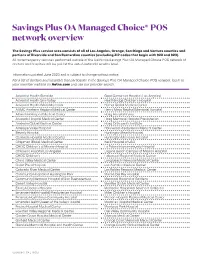
Savings Plus OA Managed Choice® POS network overview The Savings Plus service area consists of all of Los Angeles, Orange, San Diego and Ventura counties and portions of Riverside and San Bernardino counties (excluding ZIP codes that begin with 922 and 923). All nonemergency services performed outside of the California Savings Plus OA Managed Choice POS network of doctors and hospitals will be paid at the out-of-network benefits level. Information updated June 2020 and is subject to change without notice. For a list of doctors and hospitals that participate in the Savings Plus OA Managed Choice POS network, log in to your member website on Aetna.com and use our provider search. Adventist Health Glendale Good Samaritan Hospital (Los Angeles) Adventist Health Simi Valley Healthbridge Children’s Hospital Adventist Health White Memorial Hemet Global Medical Center AHMC Anaheim Regional Medical Center Henry Mayo Newhall Memorial Hospital Alhambra Hospital Medical Center Hoag Hospital Irvine Alvarado Hospital Medical Center Hoag Memorial Hospital Presbyterian Anaheim Global Medical Center Hoag Orthopedic Institute Antelope Valley Hospital Hollywood Presbyterian Medical Center Beverly Hospital Huntington Beach Hospital Centinela Hospital Medical Center Huntington Memorial Hospital Chapman Global Medical Center Keck Hospital of USC CHOC Children’s at Mission Hospital La Palma Intercommunity Hospital Children’s Hospital Los Angeles Laguna Beach Campus of Mission Hospital CHOC Children’s Lakewood Regional Medical Center Chino Valley Medical Center -

Californiachoice® Small Group Advantage PPO Three-Tier Hospital Network
CaliforniaChoice® Small Group Advantage PPO three-tier hospital network With the CaliforniaChoice Advantage PPO plans, you have a choice of tiers (or levels) of hospitals to visit. Tier one hospitals offer the greatest savings to you. Tier two hospitals have the second best level of savings. Tier three hospitals — or out-of-network hospitals — offer the least out-of-pocket savings, but you’ll still be covered. Keep in mind that the tier levels aren’t based on the quality of care given at each hospital. They’re based on which hospitals have shown they’re better able to give quality care that’s also cost effective. Our three-tier levels* are: }}Tier 1 — PPO network hospitals with lower-negotiated hospital reimbursement rates. }}Tier 2 — the remaining PPO network hospitals. }}Tier 3 — non-network hospitals. * The tier levels are not based on the quality of care given at each hospital. Instead, each level stands for the hospitals that show 19685CABENABC 08/15 the best use of health care dollars. CaliforniaChoice® Small Group Advantage PPO three-tier hospital network Here is a list of the Tier-1 and Tier-2 hospitals included in the network. Any hospital not listed is considered out of network. Hospital County Tier St Rose Hospital Alameda 1 Alameda Hospital Alameda 1 Children’s Hospital Oakland Alameda 2 Valleycare Medical Center Alameda 2 Washington Hospital Alameda 2 Sutter Amador Health Center Pioneer 1 Sutter Amador Health Center Plymouth 1 Sutter Amador Hospital Amador 1 Oroville Hospital & Medical Center Butte 1 Feather River Hospital -

Access+ HMO 2021Network
Access+ HMO 2021Network Our Access+ HMO plan provides both comprehensive coverage and access to a high-quality network of more than 10,000 primary care physicians (PCPs), 270 hospitals, and 34,000 specialists. You have zero or low copayments for most covered services, plus no deductible for hospitalization or preventive care and virtually no claims forms. Participating Physician Groups Hospitals Butte County Butte County BSC Admin Enloe Medical Center Cohasset Glenn County BSC Admin Enloe Medical Center Esplanade Enloe Rehabilitation Center Orchard Hospital Oroville Hospital Colusa County Butte County BSC Admin Colusa Medical Center El Dorado County Hill Physicians Sacramento CalPERS Mercy General Hospital Mercy Medical Group CalPERS Methodist Hospital of Sacramento Mercy Hospital of Folsom Mercy San Juan Medical Center Fresno County Central Valley Medical Medical Providers Inc. Adventist Medical Center Reedley Sante Community Physicians Inc. Sante Health Systems Clovis Community Hospital Fresno Community Hospital Fresno Heart and Surgical Hospital A Community RMCC Fresno Surgical Hospital San Joaquin Valley Rehabilitation Hospital Selma Community Hospital St. Agnes Medical Center Glenn County Butte County BSC Admin Glenn Medical Center Glenn County BSC Admin Humboldt County Humboldt Del Norte IPA Mad River Community Hospital Redwood Memorial Hospital St. Joseph Hospital - Eureka Imperial County Imperial County Physicians Medical Group El Centro Regional Medical Center Pioneers Memorial Hospital Kern County Bakersfield Family Medical -

Medi-Cal Managed Health Care Options in San Diego County
Medi-Cal Managed Health Care Your Medi-Cal Managed Care Health Plan Choices Options in San Diego County This material is being provided to help you better understand your choices. It is not an endorsement of any specific Medi-Cal Health Plan. Standard Medi-Cal Covered Services Welcome to Medi-Cal Managed Care Benefits Alvarado Hospital & Medical Center Scripps Mercy Hospital Chula Your Medi-Cal benefits can now be provided by a Medi-Cal Managed Care Health Plan. A Palomar Medical Center Vista Managed Care Health Plan gives you access to a network of doctors, clinics, specialists, Plan Network Paradise Valley Hospital Sharp Chula Vista Medical Center pharmacies and hospitals. Hospitals* Pomerado Hospital Sharp Coronado Hospital How Does Managed Care Work? Rady Children’s Hospital San Diego Sharp Grossmont Hospital Each Medi-Cal Managed Care Health Plan has a list of primary care providers you can choose *Call your Scripps Green Hospital Sharp Mary Birch Hospital for from. If you have a doctor now, you will need to find out if that doctor belongs to a Medi-Cal provider about Scripps Memorial Hospital Women & Newborns Managed Care Health Plan. Your primary care provider will be responsible for managing your using other Encinitas Sharp Memorial Hospital overall health care and referring you to other doctors if needed. locations in an Scripps Memorial Hospital La Jolla Sharp Mesa Vista Hospital Who Can Join a Medi-Cal Managed Care Health Plan? emergency. Scripps Mercy Hospital San Diego Tri-City Medical Center Anyone who is on Medi-Cal, lives in San Diego County, and has a qualifying aid code may UCSD Medical Center – Hillcrest choose a Medi-Cal Managed Care Health Plan. -
Sharp Value Provider Network Overview
Sharp Value Provider Network Overview Physicians • Hospitals • Urgent Care Centers • Pharmacies • Other Facilities Effective January 1, 2018 Sharp Value Provider Network Medical Groups At Sharp Health Plan, we understand the importance of selecting a network that fits your lifestyle and budget. As a member, you’ll join a family of award-winning medical groups, physicians and hospitals dedicated to meeting your health care needs. The Sharp Value Provider Network offers access to a core group of physicians and hospitals to provide you with greater value. With Sharp Value, you’ll have access to more than 1,900 physicians, including Primary Care Physicians and specialists. Sharp Rees-Stealy (SRS) This medical group offers a network of more than 470 physicians, including Primary Care Physicians and specialists. Admitting hospitals include Sharp HealthCare facilities and Rady Children’s Hospital. SRS physicians are located throughout San Diego County, including: • Carmel Valley • Frost Street • Mt. Helix • San Carlos • Chula Vista • Genesee • Murphy Canyon • San Diego • Del Mar • La Mesa • Otay Ranch • Scripps Ranch • Downtown San Diego • La Mesa West • Point Loma • Sorrento Mesa • El Cajon • Mira Mesa • Rancho Bernardo Sharp Community Medical Group (SCMG) This medical group offers a network of more than1,090 physicians, including Primary Care Physicians and specialists. Admitting hospitals include Sharp HealthCare facilities, Rady Children’s Hospital and Palomar Health facilities.1 SCMG, SCMG Inland North, SCMG Graybill and SCMG Arch Health -

Network Comparison List San Diego County LARGE GROUP 101+ Effective Janary 1, 2021
Network Comparison List San Diego County LARGE GROUP 101+ Effective Janary 1, 2021 Salud HMO Participating Physcian Group Full ExcelCare SmartCare y Más Arch Health Partners Cassidy Medical Group Greater Tri-Cities IPA Mercy Physicians Medical Group Mid-County Physicians Medical Group Noble AMA IPA Primary Care Associated Medical Group Rady Children's Health Network Scripps Clinic - Anderson Scripps Clinic - Carmel Valley Scripps Clinic - Del Mar Scripps Clinic - Encinitas Scripps Clinic - La Jolla Scripps Clinic - Liberty Station Scripps Clinic - Mission Valley Scripps Clinic - Rancho Bernardo Scripps Clinic - Rancho San Diego Scripps Clinic - Santee Scripps Clinic - Torrey Pines Scripps Coastal Medical Center - Carlsbad Scripps Coastal Medical Center - Eastlake Scripps Coastal Medical Center - Encinitas Scripps Coastal Medical Center - Escondido Scripps Coastal Medical Center - Hillcrest Scripps Coastal Medical Center - Oceanside Scripps Coastal Medical Center - Solana Beach Scripps Coastal Medical Center - Vista Scripps Physicians Medical Group Sharp Community Medical Group - Arch Sharp Community Medical Group - Graybill Sharp Community Medical Group - Inland North Sharp Community Medical Group at San Diego Sharp Rees-Stealy Medical Group Sharp Rees-Stealy Medical Group - Chula Vista Sharp Rees-Stealy Medical Group - La Mesa Sharp Rees-Stealy Medical Group - Mira Mesa Sharp Rees-Stealy Medical Group - Rancho Bernardo Sharp Rees-Stealy Medical Group - San Diego UC San Diego Health - Downtown - Internal Med UC San Diego Health - Eastlake -

Medi-Cal 2020 Attachment D Participating PRIME Entities
Attachment D Designated Public Hospital Systems and District/Municipal Public Hospitals that are Participating PRIME Entities The following governmental health systems participate in the Public Hospital Redesign and Incentives in Medi-Cal (PRIME) Pool. I. Designated Public Hospital (DPH) systems DPH systems include the following designated public hospitals and their affiliated governmental providers and contracted governmental and non- governmental providers, including any successor or differently named hospital as applicable. The DPHs are operated by a county, a city and county, University of California, or special hospital authority described in Section 101850 or 101852, et seq., of the California Health & Safety Code. State Government-operated University of California (UC) Hospitals 1. UC Davis Medical Center 2. UC Irvine Medical Center 3. UC San Diego Medical Center 4. UC San Francisco Medical Center 5. UC Los Angeles Medical Center 6. Santa Monica UCLA Medical Center (aka – Santa Monica UCLA Medical Center & Orthopedic Hospital) Non-State Government-operated 7. Los Angeles County (LA Co.) health system a. LA Co. Harbor/UCLA Medical Center b. LA Co. Olive View Medical Center c. LA Co. Rancho Los Amigos National Rehabilitation Center d. LA Co. University of Southern California Medical Center 8. Alameda Health System a. Highland Hospital (including the Fairmont and John George Psychiatric facilities) b. Alameda Hospital c. San Leandro Hospital 9. Arrowhead Regional Medical Center 10. Contra Costa Regional Medical Center 11. Kern Medical Center 12. Natividad Medical Center 13. Riverside University Health System -- Medical Center 14. San Francisco General Hospital 15. San Joaquin General Hospital 16. San Mateo Medical Center 17. Santa Clara Valley Medical Center 18. -

PPO Select Narrow Hospital Network
PPO Select Narrow Hospital Network Hospital County Tier ALAMEDA HOSPITAL ALAMEDA 1 ST ROSE HOSPITAL ALAMEDA 1 CHILDREN'S HOSPITAL OAKLAND ALAMEDA 2 VALLEYCARE MEDICAL CENTER ALAMEDA 2 WASHINGTON HOSPITAL ALAMEDA 2 SUTTER AMADOR HOSPITAL AMADOR 1 BIGGS MEMORIAL HOSPITAL BUTTE 1 FEATHER RIVER HOSPITAL BUTTE 1 OROVILLE HOSPITAL & MEDICAL CENTER BUTTE 1 ENLOE MEDICAL CENTER INC BUTTE 2 MARK TWAIN ST JOSEPH'S HOSPITAL CALAVERAS 1 COLUSA REGIONAL MEDICAL CENTER COLUSA 1 DOCTORS MEDICAL CENTER – SAN PABLO/PINOLE CONTRA COSTA 1 SAN RAMON REGIONAL MEDICAL CENTER CONTRA COSTA 1 JOHN MUIR MEDICAL CENTER – CONCORD CAMPUS CONTRA COSTA 2 JOHN MUIR MEDICAL CENTER – WALNUT CREEK CONTRA COSTA 2 SUTTER COAST HOSPITAL DEL NORTE 1 MARSHALL MEDICAL CENTER EL DORADO 1 BARTON MEMORIAL HOSPITAL EL DORADO 2 CLOVIS COMMUNITY HOSPITAL FRESNO 1 COALINGA REGIONAL MEDICAL CENTER FRESNO 1 COMMUNITY MEDICAL CENTER – FRESNO FRESNO 1 FRESNO HEART HOSPITAL FRESNO 1 FRESNO SURGICAL HOSPITAL FRESNO 1 SAN JOAQUIN VALLEY REHABILITATION HOSPITAL FRESNO 1 SIERRA KINGS DISTRICT HOSPITAL FRESNO 1 ST AGNES MEDICAL CENTER FRESNO 1 KINGSBURG DISTRICT HOSPITAL FRESNO 2 GLENN MEDICAL CENTER GLENN 1 MAD RIVER COMMUNITY HOSPITAL HUMBOLDT 1 JEROLD PHELPS COMMUNITY HOSPITAL HUMBOLDT 2 REDWOOD MEMORIAL HOSPITAL HUMBOLDT 2 ST JOSEPH HOSPITAL – EUREKA HUMBOLDT 2 EL CENTRO REGIONAL MEDICAL CENTER IMPERIAL 1 PIONEERS MEMORIAL HEALTHCARE DISTRICT IMPERIAL 1 NORTHERN INYO HOSPITAL INYO 1 SOUTHERN INYO HOSPITAL INYO 1 GOOD SAMARITAN HOSPITAL KERN 1 HEALTHSOUTH BAKERSFIELD REHABILITATION HOSPITAL -

2021 Plan Year Information
2021 PLAN YEAR INFORMATION MOVING AHEAD IN UNCERTAINTY 2021 AND BEYOND September 2020 IMPORTANT NOTES Version 12/16/2020 • This document was created on September 1, 2020 for reference only, and should not be used as the fixed premium rates to give to consumers. This document has been updated to fix the footer on the bronze and silver rate tables to reflect the correct APTC amounts. • Premium rates shown are for a 25-year-old and a 40-year-old single individual. • The lowest-priced plan for each metal tier is shown in bold green font. • The second-lowest silver plan is shown with a red square. • Plans that are not offered in all ZIP codes in the county are shown with an asterisk (*). • Use the Covered California Shop and Compare Tool to see the premium rates for specific ages, household size, incomes, and ZIP codes. 1 2021 PLAN BENEFIT YEAR OVERVIEW 2020 Covered California Enrollment Profile Qualified health plan enrollment Enrollment by metal plans 2019 Enrollment data as of 6/30/2019 . 3 Policies and Outreach Make a Difference in 2020 Plan Year Average dollar amount of financial help received by middle income households between 400-600% of Federal Poverty Level* 25% 23% 20% ~625,000 17% (42%) 15% 1.5 15% 13% QUALIFIED 11% MILLION FOR STATE 10% 8% SUBSIDES 7% 7% PLAN SELECTED FOR 2020 PLAN YEAR 5% 0% $1 - $50 $51 - $101 - $201 - $401 - $600 - $801 - $1,001 + $100 $200 $400 $600 $800 $1,000 Nearly 32,000 middle-income consumers qualified for the new financial help, which averaged $504 per month for eligible households, and lowered their monthly premium by half. -

OSHPD FACILITY CODES -- Sorted by Hospital CPQCC Centers Indicated in Bold Italics
OSHPD FACILITY CODES -- Sorted by Hospital CPQCC Centers Indicated in Bold Italics OSHPD CENTER NAME CITY COUNTY 700564 30TH MEDICAL GROUP (700564) 700597 60TH MEDICAL GROUP (700597) 700431 722ND MEDICAL GROUP (700431) 700103 95TH MEDICAL GROUP (700103) 190323 ADVENTIST HEALTH - GLENDALE (190323) GLENDALE LOS ANGELES 190878 ADVENTIST HEALTH - WHITE MEMORIAL (190878) LOS ANGELES LOS ANGELES 150788 ADVENTIST HEALTH BAKERSFIELD (150788) BAKERSFIELD KERN 171049 ADVENTIST HEALTH CLEARLAKE (171049) CLEARLAKE LAKE 040875 ADVENTIST HEALTH FEATHER RIVER (040875) PARADISE BUTTE 164029 ADVENTIST HEALTH HANFORD (164029) HANFORD KINGS 390923 ADVENTIST HEALTH LODI MEMORIAL (390923) LODI SAN JOAQUIN 150808 ADVENTIST HEALTH MEDICAL CENTER TEHACHAPI VALLEY (150808) TEHACHAPI KERN 560525 ADVENTIST HEALTH SIMI VALLEY (560525) SIMI VALLEY VENTURA 554011 ADVENTIST HEALTH SONORA - GREENLEY (554011) SONORA TUOLUMNE 281078 ADVENTIST HEALTH ST. HELENA (281078) ST. HELENA NAPA 231396 ADVENTIST HEALTH UKIAH VALLEY (231396) UKIAH MENDOCINO 160787 ADVENTIST MEDICAL CENTER - CENTRAL VALLEY (160787) 100797 ADVENTIST MEDICAL CENTER - REEDLEY (100797) REEDLEY FRESNO 100793 ADVENTIST MEDICAL CENTER-SELMA (100793) SELMA FRESNO 301098 AHMC ANAHEIM REGIONAL MEDICAL CENTER (301098) ANAHEIM ORANGE 010735 ALAMEDA HOSPITAL (010735) ALAMEDA ALAMEDA 010989 ALAMEDA HOSPITAL AT WATERS EDGE (010989) ALAMEDA ALAMEDA 190017 ALHAMBRA HOSPITAL MEDICAL CENTER (190017) ALHAMBRA LOS ANGELES 010844 ALTA BATES SUMMIT MED CTR-HERRICK CAMPUS (010844) BERKELEY ALAMEDA 010937 ALTA BATES SUMMIT -

Medicare Readmission Chart with September 2012 Update
Medicare Readmission Penalties by Hospital (September Update) Medicare will apply the readmissions penalty to reimbursements beginning on Oct. 1. This chart shows both the original penalties released by Medicare in August and the corrected numbers Medicare released on Sept. 28. Maryland hospitals were not penalized because the state has a unique reimbursement arrangement with Medicare. In addition, hospitals with fewer than 25 cases in each of three categories-- heart failure, heart attack and pneumonia--are exempt from the penalties. These hospitals are noted in the "Penalty Eligibility Status." Source: Kaiser Health News analysis of data from the Centers for Medicare & Medicaid Services Initial Corrected Readmission Readmission Penalty Penalty Change in Penalty Eligibility Hospital Name City State Hospital Referral Region (August) (September) Penalty Status Alabama ANDALUSIA REGIONAL HOSPITAL ANDALUSIA AL Pensacola, FL 0.62% 0.67% 0.05% Enough Cases ATHENS-LIMESTONE HOSPITAL ATHENS AL Huntsville, AL 0.05% 0.06% 0.01% Enough Cases ATMORE COMMUNITY HOSPITAL ATMORE AL Pensacola, FL 0.94% 1.00% 0.06% Enough Cases BAPTIST MEDICAL CENTER EAST MONTGOMERY AL Montgomery, AL 0.37% 0.40% 0.03% Enough Cases BAPTIST MEDICAL CENTER SOUTH MONTGOMERY AL Montgomery, AL 0.71% 0.74% 0.03% Enough Cases BAPTIST MEDICAL CENTER-PRINCETON BIRMINGHAM AL Birmingham, AL 0.00% 0.00% 0.00% Enough Cases BIBB MEDICAL CENTER CENTREVILLE AL Tuscaloosa, AL 0.00% 0.00% 0.00% Enough Cases BROOKWOOD MEDICAL CENTER BIRMINGHAM AL Birmingham, AL 0.00% 0.00% 0.00% Enough Cases -

DRG TAR-Free Phase I
DEPARTMENT OF HEALTH CARE SERVICES CLINICAL ASSURANCE AND ADMINISTRATIVE SUPPORT DIVISION LIST OF NON-DESIGNATED PUBLIC HOSPITALS (NDPH) AND PRIVATE HOSPITALS TRANSITIONING TO STANDARDIZED MEDICAL REVIEW CRITERIA PHASE I • DRG-TAR FREE (9 hospitals) Hospital Hospital Type City Mountain View El Camino Hospital NDPH Los Gatos John F. Kennedy Memorial Hospital Private Indio Lakewood Regional Medical Center Private Lakewood Lodi Memorial Hospital Private Lodi Marshall Medical Center Private Placerville Palomar Medical Center NDPH Escondido Pomerado Hospital NDPH Poway Sharp Chula Vista Medical Center Private Chula Vista Sharp Memorial Hospital Private San Diego Phase I Implementation: Admission dates on or after February 1, 2016 DEPARTMENT OF HEALTH CARE SERVICES CLINICAL ASSURANCE AND ADMINISTRATIVE SUPPORT DIVISION LIST OF NON-DESIGNATED PUBLIC HOSPITALS (NDPH) AND PRIVATE HOSPITALS TRANSITIONING TO STANDARDIZED MEDICAL REVIEW CRITERIA PHASE II • DRG-TAR FREE (9 hospitals) Hospital Hospital Type City Desert Regional Medical Center Private Palm Springs Doctors Hospital of Manteca Private Manteca Feather River Hospital Private Paradise Fountain Valley Regional Hospital Private Fountain Valley Mercy Hospital Folsom Private Folsom Olympia Medical Center Private Los Angeles St. Helena Hospital Private Saint Helena St. Rose Hospital Private Hayward Woodland Memorial Hospital Private Woodland Phase II Implementation: Admission dates on or after October 1, 2016 DEPARTMENT OF HEALTH CARE SERVICES CLINICAL ASSURANCE AND ADMINISTRATIVE SUPPORT DIVISION LIST OF NON-DESIGNATED PUBLIC HOSPITALS (NDPH) AND PRIVATE HOSPITALS TRANSITIONING TO STANDARDIZED MEDICAL REVIEW CRITERIA PHASE III • DRG-TAR FREE (12 hospitals) Hospital Hospital Type City Adventist Medical Center - Hanford Private Hanford Adventist Medical Center -- Reedley Private Reedley Adventist Medical Center - Selma Private Selma Frank R.