High Risk Pregnancy Associated Perinatal Morbidity and Mortality
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
SGS-Safeguards 04910- Minimum Wages Increased in Jiangsu -EN-10
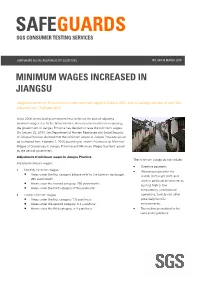
SAFEGUARDS SGS CONSUMER TESTING SERVICES CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 MINIMUM WAGES INCREASED IN JIANGSU Jiangsu becomes the first province to raise minimum wages in China in 2010, with an average increase of over 12% effective from 1 February 2010. Since 2008, many local governments have deferred the plan of adjusting minimum wages due to the financial crisis. As economic results are improving, the government of Jiangsu Province has decided to raise the minimum wages. On January 23, 2010, the Department of Human Resources and Social Security of Jiangsu Province declared that the minimum wages in Jiangsu Province would be increased from February 1, 2010 according to Interim Provisions on Minimum Wages of Enterprises in Jiangsu Province and Minimum Wages Standard issued by the central government. Adjustment of minimum wages in Jiangsu Province The minimum wages do not include: Adjusted minimum wages: • Overtime payment; • Monthly minimum wages: • Allowances given for the Areas under the first category (please refer to the table on next page): middle shift, night shift, and 960 yuan/month; work in particular environments Areas under the second category: 790 yuan/month; such as high or low Areas under the third category: 670 yuan/month temperature, underground • Hourly minimum wages: operations, toxicity and other Areas under the first category: 7.8 yuan/hour; potentially harmful Areas under the second category: 6.4 yuan/hour; environments; Areas under the third category: 5.4 yuan/hour. • The welfare prescribed in the laws and regulations. CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 P.2 Hourly minimum wages are calculated on the basis of the announced monthly minimum wages, taking into account: • The basic pension insurance premiums and the basic medical insurance premiums that shall be paid by the employers. -

Climate Research 57:123
Vol. 57: 123–132, 2013 CLIMATE RESEARCH Published August 20 doi: 10.3354/cr01174 Clim Res Extreme sea ice events in the Chinese marginal seas during the past 2000 years Jie Fei1,2,*, Zhong-Ping Lai2,3, David D. Zhang4, Hong-Ming He5 1Institute of Chinese Historical Geography, Fudan University, Shanghai 200433, PR China 2State Key Laboratory of Cryospheric Sciences (CAREERI), Chinese Academy of Sciences, Lanzhou 730000, PR China 3Qinghai Institute of Salt Lakes, Chinese Academy of Sciences, Xining 810008, PR China 4Department of Geography, The University of Hong Kong, Hong Kong SAR 5Institute of Soil and Water Conservation, Chinese Academy of Sciences & Ministry of Water Resources, Yangling District 712100, PR China ABSTRACT: We used Chinese historical literature to examine extreme records of sea ice events in the Chinese marginal seas during the past 2000 yr. We identified a total of 6 sea ice events that occurred in the sea areas to the south of 35° N. These extreme events occurred in the winters of AD 821/822, 903/904, 1453/1454, 1493/1494, 1654/1655 and 1670/1671. According to the histori- cal records, the southern limit of sea ice in the Chinese marginal seas should be in Hangzhou Bay (30−31° N), and most probably near Haiyan County in Zhejiang Province (30.5° N). The sea ice events of 1453/1454 and 1654/1655 were synchronous with the freezing events of Taihu Lake, and the sea ice event of 1670/1671 was synchronous with the freezing event of the lower reaches of the Yangtze River. However, none of the sea ice events was synchronous with the abnormally early freezing dates of Suwa Lake in Japan or the extreme freezing events of Venice Lagoon in Italy. -

GU 03032021 SHM 02 Nonfo
Produzent Adresse Land A.M. Design Ltd. Diakhali, Baron, Ashulia, Savar, Dhaka Bangladesh AB Apparels Ltd. 225, Singair Road, Tetuljhora, Hemayetpur, Savar, Dhaka Bangladesh ASR Sweater Ltd. Mulaid, Mawna, Sreepur, Gazipur, Dhaka Bangladesh Abanti Colour Tex Ltd. Plot-M-A-646, Shashongaon, Enayetnagar, Fatullah, Narayanganj, Dhaka Bangladesh Ador Composite Ltd. 1, C; B Bazar, Gilarchala, Sreepur, Gazipur, Bd Gazipur District, Gazipur, Dhaka Bangladesh Advanced Composite Textile Ltd. Kashor Masterbari, Bhaluka, Mymensingh, Sylhet Bangladesh Ahmed Fashions 34/1, Darus Salam Road, Dhaka Bangladesh Alim Knit (Bd) Ltd. Kashimpur, Nayapara, Gazipur, Gazipur, Dhaka Bangladesh Antim Knit Composite Ltd. Barpa, Rupshi, Rupgonj, Narayangonj, Dhaka Bangladesh Antim Knitting Dyeing & Finishing Ltd. Barpa, Rupshi, Rupgonj, Narayangonj, Dhaka Bangladesh Apparel Promoters Ltd. 1206/A, Nasirabad I/A, Bayzid Thana Road, Bayzid, Chittagong Bangladesh Aspire Garments Ltd. 491 Dhalla, Singair, Manikganj, Dhaka Bangladesh BHML Industries Ltd. Kamarjuri, Natun Bazar, National University, Gazipur, Dhaka Bangladesh BKC Sweater, Ltd. Plot No. 212-214, Dagerchala Main Road, Dagerchala, National University, Gazipur, Dhaka Bangladesh Basic Apparels Ltd. 135-138, Abdullahpur, Uttara, Dhaka Bangladesh Birds A & Z Ltd. Plot No. 113, Baipail, Savar, Dhaka Bangladesh Blue Planet Fashionwear Ltd. Kewa, Sreepur, Gazipur, Dhaka Bangladesh Bottoms Gallery (Pvt.) Ltd. Bulbul Tower, Dighirchala, Chandona, Joydebpur, Gazipur, Dhaka Bangladesh Chaity Composite Ltd. Chotto Silmondi, Tripurdi, Sonargaon, Narayangonj, Dhaka Bangladesh Crony Tex Sweater Ltd. Black B, Bscic Industrial Estate, Narajangonj, Dhaka Bangladesh Crown Exclusive Wears Ltd. Mawna, Sreepur, Gazipur, Dhaka Bangladesh Crown Fashion & Sweater Ind. Ltd. Plot. 781-782, Vogra, Joydebpur, P.O. Vogra, P.S. Joydebpur, Dist. Gazipur, Gazipur, Dhaka Bangladesh Crown Knitwear Ltd. 781/782, Vogra, Chourasta, Gazipur, Dhaka Bangladesh Deluxe Fashions Ltd. -

Results Announcement for the Year Ended December 31, 2020
(GDR under the symbol "HTSC") RESULTS ANNOUNCEMENT FOR THE YEAR ENDED DECEMBER 31, 2020 The Board of Huatai Securities Co., Ltd. (the "Company") hereby announces the audited results of the Company and its subsidiaries for the year ended December 31, 2020. This announcement contains the full text of the annual results announcement of the Company for 2020. PUBLICATION OF THE ANNUAL RESULTS ANNOUNCEMENT AND THE ANNUAL REPORT This results announcement of the Company will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism), and the website of the Company (www.htsc.com.cn), respectively. The annual report of the Company for 2020 will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of the National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism) and the website of the Company in due course on or before April 30, 2021. DEFINITIONS Unless the context otherwise requires, capitalized terms used in this announcement shall have the same meanings as those defined in the section headed “Definitions” in the annual report of the Company for 2020 as set out in this announcement. By order of the Board Zhang Hui Joint Company Secretary Jiangsu, the PRC, March 23, 2021 CONTENTS Important Notice ........................................................... 3 Definitions ............................................................... 6 CEO’s Letter .............................................................. 11 Company Profile ........................................................... 15 Summary of the Company’s Business ........................................... 27 Management Discussion and Analysis and Report of the Board ....................... 40 Major Events.............................................................. 112 Changes in Ordinary Shares and Shareholders .................................... 149 Directors, Supervisors, Senior Management and Staff.............................. -

Tier 1 Manufacturing Sites
TIER 1 MANUFACTURING SITES - Produced January 2021 SUPPLIER NAME MANUFACTURING SITE NAME ADDRESS PRODUCT TYPE No of EMPLOYEES Albania Calzaturificio Maritan Spa George & Alex 4 Street Of Shijak Durres Apparel 100 - 500 Calzificio Eire Srl Italstyle Shpk Kombinati Tekstileve 5000 Berat Apparel 100 - 500 Extreme Sa Extreme Korca Bul 6 Deshmoret L7Nr 1 Korce Apparel 100 - 500 Bangladesh Acs Textiles (Bangladesh) Ltd Acs Textiles & Towel (Bangladesh) Tetlabo Ward 3 Parabo Narayangonj Rupgonj 1460 Home 1000 - PLUS Akh Eco Apparels Ltd Akh Eco Apparels Ltd 495 Balitha Shah Belishwer Dhamrai Dhaka 1800 Apparel 1000 - PLUS Albion Apparel Group Ltd Thianis Apparels Ltd Unit Fs Fb3 Road No2 Cepz Chittagong Apparel 1000 - PLUS Asmara International Ltd Artistic Design Ltd 232 233 Narasinghpur Savar Dhaka Ashulia Apparel 1000 - PLUS Asmara International Ltd Hameem - Creative Wash (Laundry) Nishat Nagar Tongi Gazipur Apparel 1000 - PLUS Aykroyd & Sons Ltd Taqwa Fabrics Ltd Kewa Boherarchala Gila Beradeed Sreepur Gazipur Apparel 500 - 1000 Bespoke By Ges Unip Lda Panasia Clothing Ltd Aziz Chowdhury Complex 2 Vogra Joydebpur Gazipur Apparel 1000 - PLUS Bm Fashions (Uk) Ltd Amantex Limited Boiragirchala Sreepur Gazipur Apparel 1000 - PLUS Bm Fashions (Uk) Ltd Asrotex Ltd Betjuri Naun Bazar Sreepur Gazipur Apparel 500 - 1000 Bm Fashions (Uk) Ltd Metro Knitting & Dyeing Mills Ltd (Factory-02) Charabag Ashulia Savar Dhaka Apparel 1000 - PLUS Bm Fashions (Uk) Ltd Tanzila Textile Ltd Baroipara Ashulia Savar Dhaka Apparel 1000 - PLUS Bm Fashions (Uk) Ltd Taqwa -

Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020
Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020 Wei Zhang Xiamen University Jia Rui Xiamen University Xiaoqing Cheng Jiangsu Provincial Center for Disease Control and Prevention Bin Deng Xiamen University Hesong Zhang Xiamen University Lijing Huang Xiamen University Lexin Zhang Xiamen University Simiao Zuo Xiamen University Junru Li Xiamen University XingCheng Huang Xiamen University Yanhua Su Xiamen University Benhua Zhao Xiamen University Yan Niu Chinese Center for Disease Control and Prevention, Beijing City, People’s Republic of China Hongwei Li Xiamen University Jian-li Hu Jiangsu Provincial Center for Disease Control and Prevention Tianmu Chen ( [email protected] ) Page 1/30 Xiamen University Research Article Keywords: Hand foot mouth disease, Jiangsu Province, model, transmissibility, effective reproduction number Posted Date: July 30th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-752604/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 2/30 Abstract Background: Hand, foot, and mouth disease (HFMD) has been a serious disease burden in the Asia Pacic region represented by China, and the transmission characteristics of HFMD in regions haven’t been clear. This study calculated the transmissibility of HFMD at county levels in Jiangsu Province, China, analyzed the differences of transmissibility and explored the reasons. Methods: We built susceptible-exposed-infectious-asymptomatic-removed (SEIAR) model for seasonal characteristics of HFMD, estimated effective reproduction number (Reff) by tting the incidence of HFMD in 97 counties of Jiangsu Province from 2015 to 2020, compared incidence rate and transmissibility in different counties by non -parametric test, rapid cluster analysis and rank-sum ratio. -

Spatial and Temporal Evaluation of Ecological Footprint Intensity of Jiangsu Province at the County-Level Scale
International Journal of Environmental Research and Public Health Article Spatial and Temporal Evaluation of Ecological Footprint Intensity of Jiangsu Province at the County-Level Scale Decun Wu 1 and Jinping Liu 2,* 1 School of Public Administration and Sociology, Jiangsu Normal University, Xuzhou 221116, China; [email protected] 2 School of Economics and Management, China University of Mining and Technology, Xuzhou 221116, China * Correspondence: [email protected] Received: 10 September 2020; Accepted: 23 October 2020; Published: 26 October 2020 Abstract: Due to the high ecological pressure that exists in the process of rapid economic development in Jiangsu Province, it is necessary to evaluate its ecological footprint intensity (EFI). This article focuses on ecological footprint intensity analysis at the county scale. We used county-level data to evaluate the spatial distributions and temporal trends of the ecological footprint intensity in Jiangsu’s counties from 1995 to 2015. The temporal trends of counties are divided into five types: linear declining type, N-shape type, inverted-N type, U-shape type and inverted-U shape type. It was discovered that the proportions of the carbon footprint intensity were maintained or increased in most counties. Exploratory spatial data analysis shows that there was a certain regularity of the EFI spatial distributions, i.e., a gradient decrease from north to south, and there was a decline in the spatial heterogeneity of EFI in Jiangsu’s counties over time. The global Moran’s index (Moran’s I) and local spatial association index (LISA) are used to analyze both the global and local spatial correlation of EFIs among counties of Jiangsu Province. -

Public Factory List Combined Nov 2015
LIST OF MANUFACTURERS FOR THE VARNER GROUP Country Name of Manufacturer Address City / Area Region Bangladesh 4A Yarn Dying Ltd Kaichabari, Baipal, DEPZ Savar Dhaka Bangladesh Alema Textiles Ltd Vogra, Bashan Sarak Gazipur Dhaka Bangladesh Anan Socks Ltd Mulaid, Maowna, Sreepur Gazipur Dhaka Bangladesh Ananta Casual Wear Ltd Kunia,Targach,K.B. Bazar Gazipur Dhaka Bangladesh Ananta Denim Technology Ltd Noyabari, Kanchpur, Sonargoan Narayangonj Dhaka Bangladesh Ananta Huaxiang Ltd Plot H2-H4, 222, 223 Adamjee EPZ Narayangonj Dhaka Bangladesh Armana Fashions Ltd 232-234, Tejgaon Industrial Area Dhaka Dhaka Bangladesh Babylon Garments/Dresses Ltd 2-B/1 Darus Salam Road, Mirpur Dhaka Dhaka Bangladesh Bangladesh Spinners & Knitters Ltd Plot: 6-11; Sector: 4/A, CEPZ Chittagong Chittagong Bangladesh Bea-Con Knit Wear Limited (Factory-2) South Shalna, Shalna Bazar Gazipur Dhaka Bangladesh Body Fashion Ltd Naojur, Kodda, Joydebpur Gazipur Dhaka Bangladesh Coast To Coast PVT Ltd Vill - Itahata,Union - Bason, Mouja 35 (Chandona) Gazipur Dhaka Bangladesh Concept Knitting (Masco) Tilargati, Sataish Bazar, Tongi Gazipur Dhaka Bangladesh Creative Woolwear Ltd 3/B Darus Salam Road, Mirpur Dhaka Dhaka Bangladesh Dekko Designs Ltd East Noroshinghapur, Ashulia, Savar, Savar Dhaka Bangladesh Denimach Ltd Kewa Mouja, Ward No. 5, Gorgoria Masterbari, Sreepur Gazipur Dhaka Bangladesh DNV Clothing (Ananta) Plot No. 100/101, AEPZ, Adamjee Nagar, Siddhirgonj Narayangonj Dhaka Bangladesh Global Merchants Ltd Baimail, Konabari, Kashem Cotton Mills, Konabari, Joydevpur -

Subsidy Programs
SUBSIDIES REQUEST FROM THE UNITED STATES TO CHINA PURSUANT TO ARTICLE 25.10 OF THE AGREEMENT The following communication, dated 15 April 2016, is being circulated at the request of the Delegation of the United States. _______________ In the report that it prepared for China's most recent Trade Policy Review, held in July 2014, the Secretariat included information that it had uncovered on 30 support programs for China's fisheries sector.1 The Secretariat's Report noted that China had not notified any of these support programs to the Committee on Subsidies and Countervailing Measures (Committee) and that China could not verify any of the information provided to it by the Secretariat. During the ensuing Trade Policy Review meetings, China responded to Members' questions about these support programs by stating that it needed more time to identify and verify information regarding these support programs. In April of last year, the United States submitted questions to China with respect to these programs and other fishery support measures the United States had uncovered through its own efforts.2 Once again, despite its obligation under Article 25.9 of the Agreement to provide answers "as quickly as possible and in a comprehensive manner", China to date has not meaningfully responded to the United States' request and has refused repeated requests to meet bilaterally to discuss the issue, and the issue of subsidy notifications more generally. In November of last year, China submitted its latest subsidy notification covering the period 2009 through 2014.3 In this notification, China did not include: (1) any of the fishery subsidy programs identified in China's 2014 TPR report, (2) any of the additional measures identified by the United States in its Article 25.8 submission or (3) any of the fisheries subsidies measures identified in the 2014 Article 25.10 submission of the United States4. -

Produzent Adresse Land
Produzent Adresse Land A.M. Design Ltd. Diakhali, Baron, Ashulia, Savar, Dhaka Bangladesh AB Apparels Ltd. 225, Singair Road, Tetuljhora, Hemayetpur, Savar, Dhaka Bangladesh ASR Sweater Ltd. Mulaid, Mawna, Sreepur, Gazipur, Dhaka Bangladesh Abanti Colour Tex Ltd. Plot-M-A-646, Shashongaon, Enayetnagar, Fatullah, Narayanganj, Dhaka Bangladesh Ador Composite Ltd. 1, C; B Bazar, Gilarchala, Sreepur, Gazipur, Bd Gazipur District, Gazipur, Dhaka Bangladesh Advanced Composite Textile Ltd. Kashor Masterbari, Bhaluka, Mymensingh, Sylhet Bangladesh Ahmed Fashions 34/1, Darus Salam Road, Dhaka Bangladesh Alim Knit (Bd) Ltd. Kashimpur, Nayapara, Gazipur, Gazipur, Dhaka Bangladesh Antim Knit Composite Ltd. Barpa, Rupshi, Rupgonj, Narayangonj, Dhaka Bangladesh Antim Knitting Dyeing & Finishing Ltd. Barpa, Rupshi, Rupgonj, Narayangonj, Dhaka Bangladesh Apparel Promoters Ltd. 1206/A, Nasirabad I/A, Bayzid Thana Road, Bayzid, Chittagong Bangladesh Aspire Garments Ltd. 491 Dhalla, Singair, Manikganj, Dhaka Bangladesh BHML Industries Ltd. Kamarjuri, Natun Bazar, National University, Gazipur, Dhaka Bangladesh BKC Sweater, Ltd. Plot No. 212-214, Dagerchala Main Road, Dagerchala, National University, Gazipur, Dhaka Bangladesh Basic Apparels Ltd. 135-138, Abdullahpur, Uttara, Dhaka Bangladesh Birds A & Z Ltd. Plot No. 113, Baipail, Savar, Dhaka Bangladesh Blue Planet Fashionwear Ltd. Kewa, Sreepur, Gazipur, Dhaka Bangladesh Bottoms Gallery (Pvt.) Ltd. Bulbul Tower, Dighirchala, Chandona, Joydebpur, Gazipur, Dhaka Bangladesh Chaity Composite Ltd. Chotto Silmondi, Tripurdi, Sonargaon, Narayangonj, Dhaka Bangladesh Crony Tex Sweater Ltd. Black B, Bscic Industrial Estate, Narajangonj, Dhaka Bangladesh Crown Exclusive Wears Ltd. Mawna, Sreepur, Gazipur, Dhaka Bangladesh Crown Fashion & Sweater Ind. Ltd. Plot. 781-782, Vogra, Joydebpur, P.O. Vogra, P.S. Joydebpur, Dist. Gazipur, Gazipur, Dhaka Bangladesh Crown Knitwear Ltd. 781/782, Vogra, Chourasta, Gazipur, Dhaka Bangladesh Deluxe Fashions Ltd. -

Human Umbilical Cord Mesenchymal Stem Cells Ameliorate Hepatic
Hindawi BioMed Research International Volume 2021, Article ID 6685605, 13 pages https://doi.org/10.1155/2021/6685605 Research Article Human Umbilical Cord Mesenchymal Stem Cells Ameliorate Hepatic Stellate Cell Activation and Liver Fibrosis by Upregulating MicroRNA-455-3p through Suppression of p21-Activated Kinase-2 Qing Zhou ,1,2 Tengfei Gu ,3 Yong Zhang ,2 Hongda Li ,2 Xuemei Zhuansun ,4 Sanrong Xu ,2 and Yuting Kuang 1 1Department of General Surgery, The First Affiliated Hospital of Soochow University, Suzhou 215006, China 2Department of General Surgery, Affiliated Hospital of Jiangsu University, Zhenjiang 212001, China 3Department of Anesthesiology, People’s Hospital of Lianshui County, Jiangsu Province, Lianshui 223400, China 4Laboratory Animal Research Center, Medical College of Soochow University, Suzhou 215123, China Correspondence should be addressed to Sanrong Xu; [email protected] and Yuting Kuang; [email protected] Received 2 November 2020; Revised 2 February 2021; Accepted 6 February 2021; Published 25 February 2021 Academic Editor: Kai-Chiang Yang Copyright © 2021 Qing Zhou et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Mesenchymal stem cells (MSCs) were shown to have potential therapeutic effects for treatment of liver fibrosis, and dysregulated expression of microRNAs (miRNAs) played a pivotal role in the pathogenesis of liver fibrosis by regulating their downstream target genes. However, the mechanism by which MSCs affect the progression of liver fibrosis by regulating miRNA expression remains unclear. Here, we investigated whether human umbilical cord MSCs (HUC-MSCs) attenuated hepatic fibrosis by regulating miR-455-3p and its target gene. -

Explaining Peasants' Intention and Behavior of Farmland Trusteeship
sustainability Article Explaining Peasants’ Intention and Behavior of Farmland Trusteeship in China: Implications for Sustainable Agricultural Production Jianying Xiao 1, Yan Song 2 and Heyuan You 3,* 1 School of Public Policy & Management, China University of Mining and Technology, Xuzhou 221116, China; [email protected] 2 Department of City and Regional Planning, the University of North Carolina at Chapel Hill, Chapel Hill, NC 27599-3140, USA; [email protected] 3 School of Public Administration, Zhejiang University of Finance and Economics, Hangzhou 310018, China * Correspondence: [email protected] Received: 23 June 2020; Accepted: 15 July 2020; Published: 17 July 2020 Abstract: Developing countries generally face the problem of sustainable agricultural production during the process of agricultural modernization. Farmland trusteeship is an emerging mode of sustainable agricultural production and has played an important role in China. At present, the Chinese government has taken it as a pilot mode, but its effect also depends on the extensive participation of peasants. Based on the theory of planned behavior (TPB) and structural equation model (SEM) method, the paper analyzed peasants’ participation intention, behavior, drivers, and the influence of policy support on peasants’ participation behavior, using survey data of Jiangsu province and peasants’ participation variables. The results suggest that: (1) The behavioral attitude, subjective norms, and perceived behavioral control variables of peasants’ participation in farmland trusteeship have a significant direct impact on peasants’ willingness to participate, and these three factors indirectly influence peasants’ participation behavior by influencing peasants’ intention; (2) perceptual behavioral control variables such as the size of farmland trusteeship organization had no significant influence on peasants’ participation behaviors; (3) government policy support has a direct and significant impact on peasants’ participation behaviors.