CONCEPTS in ENDOCRINOLOGY Emma Jakoi, Ph
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Endocrinology Resident Profile Jill Trinacty
Endocrinology Resident Profile Jill Trinacty July 2017 About me My name is Jill Trinacty, and I was raised in Berwick, Nova Scotia. I went completed my BSc. (Honours) at Saint Francis Xavier University in Antigonish, Nova Scotia. I spent a year as the Active Living Coordinator with the Town of Kentville then completed my MD at Dalhousie University. I moved to Ottawa, Ontario in 2013 for my residency in Internal Medicine at the University of Ottawa and am currently a PGY-5 in Endocrinology and Metabolism. Why I chose General Endocrinology In medical school I became interested in almost every area of medicine, but ultimately applied to internal medicine for a number of reasons. I have always been interested in Endocrinology, specifically diabetes. Diabetes affects so many people in our communities and can have significant morbidity and mortality. I liked the detail of internal medicine and the complexity of patients. Having some previous experience in public health, I knew that I wanted a career that would allow me to discuss lifestyle changes as an aspect of therapy – specifically nutrition and physical activity. I also wanted a career that would allow for work/life balance. Seeing the day-to-day lifestyle of each internal medicine subspecialty confirmed that Endocrinology was the right fit for me. Clinical Life What does a typical day of clinical duties involve? This is an example of my typical daily and weekly schedule: Endocrinology – A typical day 7:30 – 8:00 Clerical work / Chief resident duties. Review emails, follow up on patient results, approve vacation requests, make call schedule. -

Actions of Vasoactive Intestinal Peptide on the Rat Adrenal Zona Glomerulosa
51 Actions of vasoactive intestinal peptide on the rat adrenal zona glomerulosa J P Hinson, J R Puddefoot and S Kapas1 Molecular and Cellular Biology Section, Division of Biomedical Sciences, St Bartholomew’s and The Royal London School of Medicine and Dentistry, Queen Mary and Westfield College, Mile End Road, London E1 4NS, UK 1Oral Diseases Research Centre, St Bartholomew’s and The Royal London School of Medicine and Dentistry, 2 Newark Street, London E1 2AT, UK (Requests for offprints should be addressed to J P Hinson) Abstract Previous studies, by this group and others, have shown that The response to VIP in adrenals obtained from rats fed vasoactive intestinal peptide (VIP) stimulates aldosterone a low sodium diet was also investigated. Previous studies secretion, and that the actions of VIP on aldosterone have found that adrenals from animals on a low sodium secretion by the rat adrenal cortex are blocked by â diet exhibit increased responsiveness to VIP. Specific VIP adrenergic antagonists, suggesting that VIP may act by binding sites were identified, although the concentration the local release of catecholamines. The present studies or affinity of binding sites in the low sodium group was not were designed to test this hypothesis further, by measur- significantly different from the controls. In the low sodium ing catecholamine release by adrenal capsular tissue in group VIP was found to increase catecholamine release to response to VIP stimulation. the same extent as in the control group, however, in Using intact capsular tissue it was found that VIP caused contrast to the control group, the adrenal response to VIP a dose-dependent increase in aldosterone secretion, with a was not altered by adrenergic antagonists in the low concomitant increase in both adrenaline and noradrenaline sodium group. -

Affect Breast Cancer Risk
HOW HORMONES AFFECT BREAST CANCER RISK Hormones are chemicals made by the body that control how cells and organs work. Estrogen is a female hormone made mainly in the ovaries. It’s important for sexual development and other body functions. From your first monthly period until menopause, estrogen stimulates normal breast cells. A higher lifetime exposure to estrogen may increase breast cancer risk. For example, your risk increases if you start your period at a young age or go through menopause at a later age. Other hormone-related risks are described below. Menopausal hormone therapy Pills Menopausal hormone therapy (MHT) is The U.S. Food and Drug Administration also known as postmenopausal hormone (FDA) recommends women use the lowest therapy and hormone replacement dose that eases symptoms for the shortest therapy. Many women use MHT pills to time needed. relieve hot flashes and other menopausal Any woman currently taking or thinking symptoms. MHT should be used at the Birth control about taking MHT pills should talk with her lowest dose and for the shortest time pills (oral doctor about the risks and benefits. contraceptives) needed to ease menopausal symptoms. Long-term use can increase breast cancer Vaginal creams, suppositories Current or recent use risk and other serious health conditions. and rings of birth control pills There are 2 main types of MHT pills: slightly increases breast Vaginal forms of MHT do not appear to cancer risk. However, estrogen plus progestin and estrogen increase the risk of breast cancer. However, this risk is quite small alone. if you’ve been diagnosed with breast cancer, vaginal estrogen rings and suppositories are because the risk of Estrogen plus progestin MHT breast cancer for most better than vaginal estrogen creams. -

HORMONES and SPORT Insulin, Growth Hormone and Sport
13 HORMONES AND SPORT Insulin, growth hormone and sport P H Sonksen Guy’s, King’s and St Thomas’ School of Medicine, St Thomas’ Hospital, London SE1 7EH, UK; Email: [email protected] Abstract This review examines some interesting ‘new’ histories of blood rather than urine samples. The first method has a insulin and reviews our current understanding of its window of opportunity lasting about 24 h after an injec- physiological actions and synergy with GH in the regu- tion and is most suitable for ‘out of competition’ testing. lation of metabolism and body composition. It reviews the The second method has reasonable sensitivity for as long as history of GH abuse that antedates by many years the 2 weeks after the last injection of GH and is uninfluenced awareness of endocrinologists to its potent anabolic actions. by extreme exercise and suitable for post-competition Promising methods for detection of GH abuse have been samples. This method has a greater sensitivity in men than developed but have yet to be sufficiently well validated to in women. The specificity of both methods seems accept- be ready for introduction into competitive sport. So far, ably high but lawyers need to decide what level of there are two promising avenues for detecting GH abuse. scientific probability is needed to obtain a conviction. Both The first uses immunoassays that can distinguish the methods need further validation before implementation. isomers of pituitary-derived GH from the monomer of Research work carried out as part of the fight against recombinant human GH. The second works through doping in sport has opened up a new and exciting area of demonstrating circulating concentrations of one or more endocrinology. -

Phenotype Microarrays Panels PM-M1 to PM-M14
Phenotype MicroArrays™ Panels PM-M1 to PM-M14 for Phenotypic Characterization of Mammalian Cells Assays: Energy Metabolism Pathways Ion and Hormone Effects on Cells Sensitivity to Anti-Cancer Agents and for Optimizing Culture Conditions for Mammalian Cells PRODUCT DESCRIPTIONS AND INSTRUCTIONS FOR USE PM-M1 Cat. #13101 PM-M2 Cat. #13102 PM-M3 Cat. #13103 PM-M4 Cat. #13104 PM-M5 Cat. #13105 PM-M6 Cat. #13106 PM-M7 Cat. #13107 PM-M8 Cat. #13108 PM-M11 Cat. #13111 PM-M12 Cat. #13112 PM-M13 Cat. #13113 PM-M14 Cat. #13114 © 2016 Biolog, Inc. All rights reserved Printed in the United States of America 00P 134 Rev F February 2020 - 1 - CONTENTS I. Introduction ...................................................................................................... 2 a. Overview ................................................................................................... 2 b. Background ............................................................................................... 2 c. Uses ........................................................................................................... 2 d. Advantages ................................................................................................ 3 II. Product Description, PM-M1 to M4 ................................................................ 3 III. Protocols, PM-M1 to M4 ................................................................................. 7 a. Materials Required .................................................................................... 7 b. Determination -

Thyroid Hormones in Fetal Growth and Prepartum Maturation
A J FORHEAD and A L FOWDEN Thyroid hormones and fetal 221:3 R87–R103 Review development Thyroid hormones in fetal growth and prepartum maturation A J Forhead1,2 and A L Fowden1 Correspondence should be addressed 1Department of Physiology, Development and Neuroscience, University of Cambridge, Physiology Building, to A L Fowden Downing Street, Cambridge CB2 3EG, UK Email 2Department of Biological and Medical Sciences, Oxford Brookes University, Oxford OX3 0BP, UK [email protected] Abstract The thyroid hormones, thyroxine (T4) and triiodothyronine (T3), are essential for normal Key Words growth and development of the fetus. Their bioavailability in utero depends on " thyroid hormones development of the fetal hypothalamic–pituitary–thyroid gland axis and the abundance " intrauterine growth of thyroid hormone transporters and deiodinases that influence tissue levels of bioactive " maturation hormone. Fetal T4 and T3 concentrations are also affected by gestational age, nutritional and " neonatal adaptation endocrine conditions in utero, and placental permeability to maternal thyroid hormones, which varies among species with placental morphology. Thyroid hormones are required for the general accretion of fetal mass and to trigger discrete developmental events in the fetal brain and somatic tissues from early in gestation. They also promote terminal differentiation of fetal tissues closer to term and are important in mediating the prepartum maturational effects of the glucocorticoids that ensure neonatal viability. Thyroid hormones act directly through anabolic effects on fetal metabolism and the stimulation of fetal oxygen Journal of Endocrinology consumption. They also act indirectly by controlling the bioavailability and effectiveness of other hormones and growth factors that influence fetal development such as the catecholamines and insulin-like growth factors (IGFs). -

Chronic Fatigue: Is It Endocrinology?
I ORIGINAL PAPERS Chronic fatigue: is it endocrinology? Kate M Evans, Daniel E Flanagan and Terence J Wilkin Kate M Evans ABSTRACT – Fatigue and stress-related illnesses imal physical signs where initial investigations are MRCP, Consultant often become diagnoses of exclusion after exten- normal. It is possible to reassure the individual that Physician sive investigation. ‘Tired all the time’ is a frequent there is no significant disease at that point but there Daniel E reason for referral to the endocrine clinic, the are no clear data to address the question of whether Flanagan implicit question being – is there a subtle overt pathology will develop in the future. This paper FRCP, Consultant endocrine pathology contributing to the patient’s reports audit findings for a cohort of patients seen Physician symptoms? Often initial assessment suggests not in an endocrinology clinic with fatigue, including but there are no clear data to address the ques- Terence J Wilkin outcome data at five or more years later. FRCP, Professor of tion of whether overt pathology will develop in the Medicine future. This study observed outcomes after five Subjects and methods years in 101 consecutive and unselected referrals Department of to secondary care for ‘fatigue?cause’, where initial Consecutive and unselected referrals from primary Endocrinology and assessment did not suggest treatable endocrine care to the endocrinology service over a four-year Metabolism, Peninsula Medical pathology. The findings suggest that the clinical period (1995–99) were identified from the clinic School, Plymouth diagnosis of fatigue, based on history and tests to database. Referrals were included in the dataset if the and Derriford exclude anaemia, hypothyroidism and diabetes, is primary reason for referral or primary symptom was Hospital, Plymouth secure: these patients do not subsequently fatigue. -

Chapter 45-Hormones and the Endocrine System Pathway Example – Simple Hormone Pathways Stimulus Low Ph in Duodenum
Chapter 45-Hormones and the Endocrine System Pathway Example – Simple Hormone Pathways Stimulus Low pH in duodenum •Hormones are released from an endocrine cell, S cells of duodenum travel through the bloodstream, and interact with secrete secretin ( ) Endocrine the receptor or a target cell to cause a physiological cell response Blood vessel A negative feedback loop Target Pancreas cells Response Bicarbonate release Insulin and Glucagon: Control of Blood Glucose Body cells •Insulin and glucagon are take up more Insulin antagonistic hormones that help glucose. maintain glucose homeostasis Beta cells of pancreas release insulin into the blood. The pancreas has clusters of endocrine cells called Liver takes islets of Langerhans up glucose and stores it as glycogen. STIMULUS: Blood glucose Blood glucose level level declines. rises. Target Tissues for Insulin and Glucagon Homeostasis: Blood glucose level Insulin reduces blood glucose levels by: (about 90 mg/100 mL) Promoting the cellular uptake of glucose Blood glucose STIMULUS: Slowing glycogen breakdown in the liver level rises. Blood glucose level falls. Promoting fat storage Alpha cells of pancreas release glucagon. Liver breaks down glycogen and releases glucose. Glucagon Glucagon increases blood glucose levels by: Stimulating conversion of glycogen to glucose in the liver Stimulating breakdown of fat and protein into glucose Diabetes Mellitus Type I diabetes mellitus (insulin-dependent) is an autoimmune disorder in which the immune system destroys pancreatic beta cells Type II diabetes -

Endocrinology Test List Endocrinology Test List
For Endocrinologists Endocrinology Test List Endocrinology Test List Extensive Capabilities Managing patients with endocrine disorders is complex. Having access to the right test for the right patient is key. With a legacy of expertise in endocrine laboratory diagnostics, Quest Diagnostics offers an extensive menu of laboratory tests across the spectrum of endocrine disorders. This test list highlights the extensive menu of laboratory diagnostic tests we offer, including highly specialized tests and those performed using highly specific and sensitive mass spectrometry detection. It is conveniently organized by glandular function or common endocrine disorder, making it easy for you to identify the tests you need to care for the patients you treat. Comprehensive Care Quest Diagnostics Nichols Institute has been pioneering state-of-the-art endocrine testing for over four decades. Our commitment to innovative diagnostics and our dedication to quality and service means we deliver solutions that enable you to make informed clinical decisions for comprehensive patient management. We strive to remain at the forefront of innovation in endocrine testing so you can deliver the highest level of patient care. Abbreviations and Footnotes NDM, neonatal diabetes mellitus; MODY, maturity-onset diabetes of the young; CH, congenital hyperinsulinism; MSUD, maple syrup urine disease; IHH, idiopathic hypogonadotropic hypogonadism; BBS, Bardet-Biedl syndrome; OI, osteogenesis imperfecta; PKD, polycystic kidney disease; OPPG, osteoporosis-pseudoglioma syndrome; CPHD, combined pituitary hormone deficiency; GHD, growth hormone deficiency. The tests highlighted in green are performed using highly specific and sensitive mass spectrometry detection. Panels that include a test(s) performed using mass spectrometry are highlighted in yellow. For tests highlighted in blue, refer to the Athena Diagnostics website (athenadiagnostics.com/content/test-catalog) for test information. -
Endocrinology Review – Adrenal and Thyroid Disorders
FOCUS: ENDOCRINOLOGY Endocrinology Review – Adrenal and Thyroid Disorders LINDA S. GORMAN, JANELLE M. CHIASERA LEARNING OBJECTIVES This article represents the first of three articles focusing 1. Define endocrinology and list the major endocrine on the endocrine system. The first article will provide glands of the body. you with fundamental theory regarding the endocrine system that will serve as a basis for understanding the 2. Explain how feedback (positive and negative) Downloaded from promotes maintenance of normal levels of next two articles focusing on two specific endocrine hormones. glands, the thyroid and adrenal glands. 3. Differentiate between steroid and peptide hormones with regard to their mechanism of Endocrinology is the branch of medical science that action. deals with the endocrine system, a system that consists 4. Provide examples of peptide and steroid hormones. of several glands located in different parts of the body http://hwmaint.clsjournal.ascls.org/ 5. Explain how endocrine disorders are categorized. that secrete hormones directly into the bloodstream. Although every organ system in the body may respond ABBREVIATIONS: ACTH - adrenocorticotropic hor- to hormones, endocrinology focuses specifically on mone; ADH - antidiuretic hormone; CRH – cortico- endocrine glands whose primary function is hormone tropin releasing hormone; DHEA – dehydroepian- secretion. Major endocrine glands include the pituitary drosterone; FSH - follicle stimulating hormone; GHRH (anterior and posterior), hypothalamus, thyroid, - growth hormone -
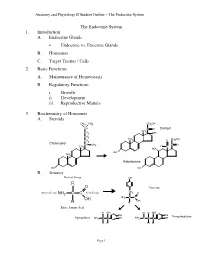
Lecture Outline
Anatomy and Physiology II Student Outline – The Endocrine System The Endocrine System 1. Introduction A. Endocrine Glands • Endocrine vs. Exocrine Glands B. Hormones C. Target Tissues / Cells 2. Basic Functions A. Maintenance of Homeostasis B. Regulatory Functions i. Growth ii. Development iii. Reproductive Matters 3. Biochemistry of Hormones A. Steroids CH3 CH3 CH2OH CH C O Cortisol CH CH2 3 OH CH2 CH CH OH CH 3 O 2 2 Cholesterol CH CH C O 3 H CH3 C HO HO CH 3 Aldosterone HO HO B. Amines Radical Group OH R O Tyrosine CH Amino Group NH2 C C Acid Group 2 O NH2 C C OH OH H H Basic Amino Acid H OH H H OH OH OH Norepinephrine Epinephrine NH2 C C OH NH2 C C C OH H H H H Page 1 Anatomy and Physiology II Student Outline – The Endocrine System C. Peptides • Antidiuretic Hormone • Oxytocin Oxytocin Antidiuretic Hormone Tyr Tyr Cys Cys Ileu Phe Glu Glu Cys Pro Leu Gly Cys Pro Arg Gly Asp Asp D. Proteins E. Glycoproteins 4. Feedback Control System A. Negative Feedback System (See Endocrine Pathways Handout: “Control Paradigm (Negative Feedback System)) i. Example: (See Endocrine Pathways Handout: “Negative Feedback Example”) B. Positive Feedback System (See Endocrine Pathways Handout: “Positive Feedback Example”) i. Child Birth and Oxytocin Page 2 Anatomy and Physiology II Student Outline – The Endocrine System 5. Mechanisms of Hormone Control A. Fixed-Membrane-Receptor Mechanism ii. Mechanism Inactive ATP Enzyme 1 Inactive cAMP Active Enzyme 2 Enzyme 1 (Secondary Active Messenger) Enzyme 2 Inactive Inactive Enzyme 4 ActiveEnzyme 3 Enzyme 3 Altered Active Cell Function Enzyme 4 ii. -

Different Mechanisms of Calcitonin, Calcitonin Gene-Related Peptide
Henry Ford Hospital Medical Journal Volume 35 Number 2 Second International Workshop on Article 20 MEN-2 6-1987 Different Mechanisms of Calcitonin, Calcitonin Gene-Related Peptide, and Somatostatin Regulation by Glucocorticoids in a Cell Culture of Human Medullary Thyroid Carcinoma Gilbert J. Cote Robert F. Gagel Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons Recommended Citation Cote, Gilbert J. and Gagel, Robert F. (1987) "Different Mechanisms of Calcitonin, Calcitonin Gene-Related Peptide, and Somatostatin Regulation by Glucocorticoids in a Cell Culture of Human Medullary Thyroid Carcinoma," Henry Ford Hospital Medical Journal : Vol. 35 : No. 2 , 149-152. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol35/iss2/20 This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons. Different Mechanisms of Calcitonin, Calcitonin Gene-Related Peptide, and Somatostatin Regulation by Glucocorticoids in a Cell Culture of Human Medullary Thyroid Carcinoma Gilbert J. Cote, and Robert F. Gagel* We have employed the TT cell line, a model for the human medullary thyroid carcinoma cell, lo study the regulation of peptide hormone production by glucocorticoids. Complementary DNA probes were used to measure the calcitonin (CT), CT gene-related peptide (CGRP), and somatostatin (SRIF) mRNA levels. Dose-response experiments in serum-free medium showed that dexamethasone (six-day treatment) lowered somatostatin (to 1% of basal) and CGRP mRNA (to 50% of basal) and stimulated CT mRNA (threefold to thirteenfold) with a half-maximal effective concentration of 10 " M.