Local Perceptions of an Integrated School Health and Nutrition Programme Involving
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
FW Emergency Plan of Action (Epoa) Population Movement Complex Emergency
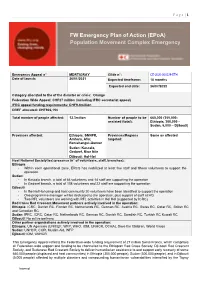
P a g e | 1 FW Emergency Plan of Action (EPoA) Population Movement Complex Emergency Emergency Appeal n° MDRTIGRAY Glide n°: CE-2020-000229-ETH Date of launch: 26/01/2021 Expected timeframe: 18 months Expected end date: 26/07/2022 Category allocated to the of the disaster or crisis: Orange Federation Wide Appeal: CHF27 million (including IFRC secretariat appeal) IFRC appeal funding requirements: CHF9.4million DREF allocated: CHF906,154 Total number of people affected: 12.3milion Number of people to be 660,000 (355,000- assisted (total): Ethiopia, 300,000 - Sudan, 5,000 – Djibouti) Provinces affected: Ethiopia: SNNPR, Provinces/Regions Same as affected Amhara, Afar, targeted: Benishangul-Gumuz Sudan: Kassala, Gedaref, Blue Nile Djibouti: Hol-Hol Host National Society(ies) presence (n° of volunteers, staff, branches): Ethiopia - Within each operational zone, ERCS has mobilized at least five staff and fifteen volunteers to support the operation. Sudan: - In Kassala branch, a total of 66 volunteers and 14 staff are supporting the operation - In Gedaref branch, a total of 108 volunteers and 22 staff are supporting the operation Djibouti - In the Hol Hol camp and host community 20 volunteers have been identified to support the operation - One programme manager will be dedicated to the operation, plus support of staff at HQ - Two RFL volunteers are working with RFL activities in Hol Hol (supported by ICRC) Red Cross Red Crescent Movement partners actively involved in the operation: Ethiopia: ICRC, Danish RC, Finnish RC, Netherlands RC, German -

January-December 2020.Pdf
Ethiopia Country Office Humanitarian Situation Report UNICEF Ethiopia/2020/ Mulugeta Ayene Situation in Numbers Reporting Period: January – December 2020 4,872,000 children in need of Highlights humanitarian assistance • Over the course of 2020, the number of children in need of humanitarian assistance increased from 4.87 million to 10.3 million (Humanitarian Response Plan Mid-Year Review). Flooding, cholera, 8,400,000 COVID-19, locust infestation, and conflict-induced displacement people in need drove humanitarian needs as evidenced by the increase in the (Humanitarian Response number of children in need of humanitarian assistance with significant Plan 2020) impact on children’s health, vulnerability to violence and educational attainment. The community transmission of COVID-19 has increased 1,846,551 the overall vulnerability of the population, stalling the delivery of internally displaced people essential life-saving services, impacting livelihoods and increasing the cost of service delivery, including critical humanitarian assistance. (IOM, Displacement Tracking Matrix 23) • With UNICEF support, over 1 million people (Internally Displaced Persons/IDPs and IDP returnees) have gained access to a sufficient 802,821 quantity of safe water for drinking, cooking and personal hygiene; registered refugees while 401,814 children (8,720 refugees) have been treated for Severe (UNHCR, 31 December 2020) Acute Malnutrition (SAM), and mobile health and nutrition teams have reached 463,766 IDPs in hard-to-reach areas in Afar and Somali regions. Another 130,994 people (all IDP/IDP returnees) have 1,102,484 benefitted from Gender-Based Violence (GBV) risk mitigation and people affected by floods response interventions, while over 400,000 individuals have received (FEWSNET, December 2020) cash transfer support to mitigate the effects of emergencies across several regions. -

Effects of Elevations on Woody Species Diversity and Carbon Stocks of Kella Natural Forests in Konso Zone, Southern Ethiopia
EFFECTS OF ELEVATIONS ON WOODY SPECIES DIVERSITY AND CARBON STOCKS OF KELLA NATURAL FORESTS IN KONSO ZONE, SOUTHERN ETHIOPIA M.Sc. THESIS BIRUK LULSEGED TILAHUN HAWASSA UNIVERSITY WONDO GENET COLLEGE OF FORESTRY AND NATURAL RESOURCES WONDO GENET, ETHIOPIA JUNE, 2019 i | P a g e EFFECTS OF ELEVATION ON WOODY SPECIES DIVERSITY AND CARBON STOCKS OF KELLA NATURAL FORESTS IN KONSO ZONE, SOUTHERN ETHIOPIA BIRUK LULSEGED TILAHUN A THESIS SUBMITTED TO DEPARTEMENT OF GENERAL FORESTRY, WONDO GENET COLLEGE OF FORESTRY AND NATURAL RESOUECES HAWASSA UNIVERSITY, WONDO GENET, ETHIOPIA IN PARTIAL FULFILLMENET OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE IN FOREST RESOURCES ASSESMENT AND MONITORING JUNE, 2019 ii | P a g e APPROVAL SHEET- I This is to certify that the thesis entitled “Effects of Elevation on Carbon Stocks and Woody Species Diversity of Kella Natural Forests in Konso Zone, Southern Ethiopia” submitted in partial fulfillment of the requirements for the degree of Master of science with specialization in Forest Resources Assessment and Monitoring of the graduate program of the department of General Forestry / Hawassa University, Wondo Genet College of Forestry and Natural Resources, and is a record of original research has been carried out by Biruk Lulseged ID No. M.Sc./FRAM/R004/09, under my supervision. Therefore, I recommend that the student has fulfilled the requirements and hence hereby can submit the thesis to the department. Dr Mesele Negash_ ________________ ___________ Name of Advisor Signature Date iii | P a g e APPROVAL SHEET- II We, the undersigned, members of the Board of Examiners of the final open defense by Biruk Lulseged have read and evaluated her thesis entitled “Effects of Elevation on Carbon Stocks and Woody Species Diversity of Kella Natural Forests in Konso Zone,Southern Ethiopia” and examined the candidate. -

HIGHLIGHTS in THIS ISSUE: Harvest Is Anticipated in the Highland and Midland Woredas • REGIONAL OVERVIEW of the Region
FOCUS ON ETHIOPIA PAGE 1 slaughtering of milking cows. Meanwhile, good meher HIGHLIGHTS IN THIS ISSUE: harvest is anticipated in the highland and midland woredas • REGIONAL OVERVIEW of the region. • NEWS: - POOR RAIN FORECASTS SUGGEST … - NEW NATIONAL NUTRITION STRATEGY Serious shortage of water and pasture is reported in Dillo, • UPCOMING & ONGOING MEETINGS Miyo, Dire, Dhas, Moyale, Teltele, Arero, and Yabello woredas in Borena zone; Liben woreda in Guji zone and 56 kebeles in various woredas of East Hararghe zone. The Focus on Ethiopia is produced by UN Office for the Coordination of Humanitarian Affairs (OCHA), in situation is severe in Dire woreda. Most of the ponds and collaboration with other UN agencies and partner NGOs. cisterns have dried and the yield of traditional wla/wells has Focus on Ethiopia provides a monthly overview of decreased. Most hand pumps, motorized units, and humanitarian trends and activities in Ethiopia, as well as boreholes require immediate rehabilitation. Pasture focusing on particular issues of interest. Send comments, reserves in Borena zone are over grazed, resulting in suggestions and contributions to [email protected] unusual livestock migration. Influx of herds from neighboring Somali Region aggravated the situation. Some schools are reportedly closed and dropout rates have increased, according to a joint assessment undertaken in REGIONAL OVERVIEW early January 2008. In addition, locust infestation in Bale, Borena and East Hararghe zones is damaging vegetation. OROMIYA The food security situation in the lowland woredas of As a result the physical condition of livestock deteriorated Borena, Guji, Bale, Arsi, East and West Hararghe zones is of and deaths of cattle is being reported. -

Traits and Farming System of Cowpea in the Southern Ethiopia
Production Constraints,Farmers Preferred- traits and Farming System of Cowpea in the Southern Ethiopia Yasin Goac ( [email protected] ) Southern Agricultural Research Institute, P. O. Box 79, Areka, Ethiopia Walelign Worku Hawassa University Hussein Mohammed Hawassa University Elias Urage Southern Agricultural Research Institute, P. O. Box 6, Hawassa, Ethiopia Research Keywords: Constraints,Cowpea, Farmers preference, Southern Ethiopia, Survey Posted Date: April 26th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-457943/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/23 Abstract The study was conducted at Gofa, Humbo, Kindo koyisha and Konso districts of South Nation Nationalities and Peoples Region (SNNPR) from May 2016 to February 2017 with the objective to assess the limitations on cowpea production conceived by farmers, farmers traits of interest and the farming system of cowpea. Participatory rural appraisal tools, which include seven focus group discussions and survey with 150 individual farmers, were used to generate data. Data recorded were analyzed on SPSS software and descriptive statistics were applied. The results showed that 85.3% of the farmers surveyed were men and the size of families ranged from 6 to 9 at the household level. Almost (40%) produced cowpea for household consumption, while 21.3% reported its food and income generation. The average cowpea elds were 0.24 ha with 503 kg/ ha as an average seed yield. The results revealed that 92.7% of farmers grow local landraces, whose seeds are recycled for many consecutive seasons, while approximately 7.3% grow both improved and local landrace. -

Outbreak Investigation, District Health Profile Description and Others Outputs Those Constituted in This Document
ADDIS ABABA UNIVERSITY, COLLEGE OF HEALTH SCIENCES, SCHOOL OF PUBLIC HEALTH Ethiopian Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field Epidemiology By: Ababu Fayisa Aboma (RN, BSc Nurse) Submitted to the School of Graduate Studies of the Addis Ababa University in Partial Fulfillment for the Degree of Master of Public Health in Field Epidemiology March 2021 Addis Ababa, Ethiopia ADDIS ABABA UNIVERSITY, COLLEGE OF HEALTH SCIENCES, SCHOOL OF PUBLIC HEALTH Ethiopian Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field Epidemiology By: - Ababu Fayisa Aboma (RN, BSc Nurse) Submitted to the School of Graduate Studies of Addis Ababa University in partial fulfillment for the degree of Master of Public Health in Field Epidemiology Mentors 1. Prof. Ahmed Ali 2. Mr. Sefonias Getachew March 2021 Addis Ababa, Ethiopia ADDIS ABABA UNIVERSITY, SCHOOL OF GRADUATE STUDIES Compiled Body of Works in Field Epidemiology By- Ababu Fayisa Aboma Ethiopian Field Epidemiology Training Program (EFETP) School of Public Health, College of Health Sciences Addis Ababa University Approval by Examining Board ___________________________ _______________ Chairman, School Graduate Committee ___________________________ ________________ Advisor ___________________________ ________________ Examiner ___________________________ ________________ Examiner Acknowledgements In this document, I would like to acknowledge individuals and institutions that have great contribution in all my field base residencies and projects. First, I would like to thank my Mentor, Prof. Ahmed Ali, who provided me with continuous guidance and excellent constructive comments on my outputs and encourages me to finalize this document on time. These provisions of guidance and comments help me to improve my work’s quality and might help me in my future career. -

Sero-Prevalence of Pesti Des Petitis Ruminants (PPR) in Selected Districts of Hawassa Zuriya, Konso Special and Zala Using Competitive ELISA (C-ELISA) Technique
Sero-Prevalence of Pesti Des Petitis Ruminants (PPR) in Selected Districts of Hawassa Zuriya, Konso Special and Zala using Competitive ELISA (C-ELISA) Technique Misganaw Mulugeta Chufamo, Shimelis Dejene Hayle, Desalegn Dosa Mengesha and Samson Abebe Boyza Sodo Regional Veterinary Laboratory, P.O. Box 82, Wolaita Sodo, Ethiopia Key words: PPR, sero-prevalence, shoats, samples, goats Abstract: A cross-sectional study to investigate the sero-prevalence of Peste des Petits Ruminants (PPR) was conducted between January and May, 2017 in selected districts of Hawassa Zuriya, Konso and Zala in the working areas of Sodo Regional Veterinary Laboratory. A total of 644 serum samples were collected from both the species of sheep and goats. Competitive Enzyme Linked Immunosorbent Assay (c-ELISA) was used to detect the presence of antibodies in the sera of shoats as indicator of exposure to the PPR virus. The results showed an overall individual animal sero-prevalence of 35.86% (231/644). The sero prevalence of the disease in the different districts of Konso, Hawassa Zuriya and Zala was 59.9% (182/304), 15.3% (34/314) and 12.7% (15/118), respectively where there is statistical significance difference in the different sites (p<0.05). The prevalence in sheep and goat was 35.6% (37/104) and 35.92% (194/540) where there is statistical significance difference in the different sites (p<0.05). At the same time the sero-prevalence in the young and adult goats was 32.3% (140/434) and 43.3% (91/210/1) respectively and there was statistically significant (p<0.05). -

Morphological Similarity and Contact: Plurals, Punctuals and Pluractionals in Konso and Gawwada (Cushitic, Southwest-Ethiopia)
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Institutional Research Information System University of Turin Rainer Vossen & Christa König (eds.): Patterns of Linguistic Convergence in Africa Frankfurter Afrikanistische Blätter 27/28 (2015/16) 171-193 Rüdiger Köppe Verlag, Köln Morphological Similarity and Contact: Plurals, Punctuals and Pluractionals in Konso and Gawwada (Cushitic, Southwest-Ethiopia) Ongaye ODA ORKAYDO & Mauro TOSCO Dilla University, Ethiopia & Università degli Studi di Torino, Italy 1 Introduction Konso and Gawwada are East Cushitic languages of the Afro-Asiatic phylum spoken in southwest Ethiopia. They belong to the Konsoid and Dullay subgroups, respective- ly (see figure 1). The Konsoid group consists of Konso, Diraytata (also referred to as Diraasha and, previously, Gidole), and Bussa (or Musiyye; Black 1974). The Dullay cluster consists of Gawwada, Ts’amakko and Harso-Dobase (Tosco 2007).1 From an administrative point of view, the Konso live in the Konso Zone; the Diraahe and Bussa (Musiyye) live in the Dirashe Special Wereda (“district”), and the Ale (Gaw- wada and Harso-Dobase) live in the Ale Special Wereda, while the Ts’amay (the speakers of Ts’amakko) are part of the South Omo Zone in the Southern Nations, Nationalities and Peoples’ Regional State (SNNPRS). Sasse (1986) discovered the existence of a small language area fully located within southwest Ethiopia: the Sagan Language Area (from the name of a river crossing the area), which consists of languages and dialects belonging to different subgroups of East Cushitic, a still unclassified language (Ongota, or, in Sasse’s terms, Birelle) and, “with some reservations,” the Omotic languages (of the Ometo subgroup) Koyra and Zayse. -

Assessing the Change and Continuity in the Social Organization and Practices Among the Kore of Southwestern Ethiopia
International Journal of Social Science And Human Research ISSN(print): 2644-0679, ISSN(online): 2644-0695 Volume 03 Issue 11 November 2020 DOI: 10.47191/ijsshr/v3-i11-08 Page No :299-305 Assessing the Change and Continuity in the Social Organization and Practices among the Kore of Southwestern Ethiopia Eshettu Tesfaye Retta Department of History and Heritage Management, Wolaita Sodo University, P.O. Box. 138, Wolaita Sodo, Ethiopia, Abstract: This study was aimed at assessing the change and continuity in the social organization in Ethiopia taking an example of Kore society, among the Amaro of southwestern Ethiopia. Qualitative research methodology was applied to describe the issue under consideration. The researcher tried to define social organization features and several of its associated components and their linkages. The study examines the way conquest and modernization deteriorated the social organization of the indigenous communities of Kore. It also tries to see the role of other factors like the missionary activities and the adherence of socialism by Ethiopian state as contributors. Key Words: Kore, Social Organization, Christianity, Modernization, Change and Continuity I. INTRODUCTION Human being has passed most of his history as hunter and gatherer by wondering from place to place. Settlement and social organizations are directly related with the beginning of river valley civilizations during the Neolithic era. This period was also characterized by permanent settlement, relatively advanced knowledge and complex socialization. -
March 2021 Children in Need Of
Ethiopia Country Office Humanitarian Situation Report Includes results from Tigray Response Situation in Numbers © UNICEF Ethiopia/2021/Demissew Bizuwerk 12.5 million Reporting Period: March 2021 children in need of humanitarian assistance 1 Highlights (HNO 2021) • In the past three months, UNICEF has reached a total of 1,583,723 people with safe water supply for personal use through the rehabilitation of non-functional water systems, water 23.5 million people in need treatment, and water trucking throughout the country. Of these, (HNO 2021) 641,976 people have been reached in Tigray Region. • Some 38,758 in people in Tigray were reached through the 22 active Mobile Health and Nutrition Teams (MHNTs), out of whom 2.3 million2 11,594 were children who received medical consultations, internally displaced people nutrition services, and immunization. (DTM, 2021) • Since the beginning of its response in Tigray, UNICEF has delivered 1,093.4 metric tons of multi-sectoral supplies to nine partners (including regional bureaus) with a total value of US$2.5 805,164 million. registered refugees • In February, 34,883 new cases of Severe Acute Malnutrition (UNHCR, 31 March 2021) (SAM) were admitted for treatment throughout the country. Out of these, 48 per cent were in Oromia, 26.7 percent in Somali, and 4.3 per cent in Tigray. The cure rate was 90.9 per cent, death rate was 0.2 per cent and defaulter rate was 1.85 per cent. The UNICEF HAC Appeal rest were medical transfers or non-respondent children. 2021 US$ 188 million UNICEF’s Response and Funding -

National Meteorological Agency Agrometeorological Bulletin
NATIONAL METEOROLOGICAL AGENCY AGROMETEOROLOGICAL BULLETIN SEASONAL AGROMETEOROLOGICAL BULLETIN BELG 2009 VOLUME 19 No. 15 DATE OF ISSUE: - JUNE 10, 2009 P.O.BOX 1090, ADDIS ABABA, ETHIOPIA E.Mail: [email protected] Fax: 251-11-6625292, Tel. 251-11-6615779 FORE WARD This Agro met Bulletin is prepared and disseminated by the National Meteorological Agency (NMA). The aim is to provide those sectors of the community involved in Agriculture and related disciplines with the current weather situation in relation to known agricultural practices. The information contained in the bulletin, if judiciously utilized, are believed to assist planners, decision makers and the farmers at large, through an appropriate media, in minimizing risks, increase efficiency, maximize yield. On the other hand, it is vital tool in monitoring crop/ weather conditions during the growing seasons, to be able to make more realistic assessment of the annual crop production before harvest. The Agency disseminates ten daily, monthly and seasonal weather reports in which all the necessary current information’s relevant to agriculture are compiled. We are of the opinion that careful and continuous use of this bulletin can benefit to raise ones agro climate consciousness for improving agriculture-oriented practices. Meanwhile, your comments and constructive suggestions are highly appreciated to make the objective of this bulletin a success. Director General NMA P.O.Box 1090 Tel: 011661-57-79 FAX 00251-11-6625292 E-mail [email protected] Addis Ababa Web site: - http://www.ethiomet.gov.et -

Rate of Peripheral Blood Smear Examination Service Provision and Its Barriers Among Public Hospitals in Southern Ethiopia: a Mixed-Methods Study
Rate of Peripheral Blood Smear Examination Service Provision and Its Barriers Among Public Hospitals in Southern Ethiopia: A Mixed-Methods Study Aklilu Alemayehu ( [email protected] ) Arba Minch University Tsegaye Yohanes Arba Minch University Tamiru Shibiru Arba Minch University Zeleke Hailemariam Arba Minch University Research Article Keywords: Peripheral Blood Smear Examination, Service Provision, Barriers, Southern Ethiopia Posted Date: June 1st, 2021 DOI: https://doi.org/10.21203/rs.3.rs-523176/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/25 Abstract Introduction: Peripheral blood smear examination is a vital hematological test for diagnosis and monitoring of disorders in blood. Despite the considerable benets of this test in the battle against the growing burden of communicable and non-communicable diseases, its rate of provision is low. This study aimed to assess the rate of peripheral blood smear examination service provision and its barriers among public hospitals in southern Ethiopia. Method: We have conducted a descriptive cross-sectional study from January 01 to March 31, 2019, among ve public hospitals in Southern Ethiopia. We collected socio-demographic data from patients and healthcare providers. We prepared peripheral blood smears from 423 patients with abnormal complete blood cell count. We examined a wright’s stained peripheral blood smear under the microscope to identify abnormality in the morphology of blood cells. We conducted key informant interviews with healthcare providers. We assessed health facilities using a standard checklist. We did descriptive statistical analysis for quantitative data using Statistical Package for Social Sciences (SPSS) version 20.0 software.