3D Osteology of the Nasal Cavity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

An Endoscopic Study on the Prevalence of the Accessory Maxillary Ostium in Chronic Sinusitis Patients
International Journal of Otorhinolaryngology and Head and Neck Surgery Varadharajan R et al. Int J Otorhinolaryngol Head Neck Surg. 2020 Jan;6(1):40-44 http://www.ijorl.com pISSN 2454-5929 | eISSN 2454-5937 DOI: http://dx.doi.org/10.18203/issn.2454-5929.ijohns20195211 Original Research Article An endoscopic study on the prevalence of the accessory maxillary ostium in chronic sinusitis patients Ramesh Varadharajan*, Swara Sahithya, Ranjitha Venkatesan, Agaman Gunasekaran, Sneha Suresh Department of Otorhinolaryngology and Head and Neck Surgery , Aarupadai Veedu Medical College and Hospital, Kirumampakkam, Puducherry, India Received: 21 October 2019 Revised: 07 November 2019 Accepted: 08 November 2019 *Correspondence: Dr. Ramesh Varadharajan, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: Chronic maxillary sinusitis is one of the common ENT problems. Accessory maxillary ostium (AMO) has been postulated in many publications to play a role in the development of chronic maxillary sinusitis. AMO is found in the medial wall of maxillary sinus and located in the lateral wall of the nose. It’s been frequently identified in the routine nasal endoscopy. The variations in the location of AMO have been evaluated by nasal endoscopy in live subjects or through cadaver dissections by many authors. This live study is conducted to identify the prevalence of AMO during nasal endoscopic evaluation of chronic sinusitis patients. -

Foley Catheter Action in the Nasopharynx a Cadaveric Study
ORIGINAL ARTICLE Foley Catheter Action in the Nasopharynx A Cadaveric Study Wai Chung Lee, FRCS(ORL); Peter Ka Ming Ku, FRCSEd; Charles Andrew van Hasselt, FRCS Objectives: To determine the action of the Foley cath- eral side at appropriate inflation volumes in 17 (85%) of eter in the posterior nasal cavity in relation to balloon 20 nasal fossae. Complete sealing between volumes of 12 volume, and to deduce its implications in the treatment and 15 mL was achieved in 13 fossae (65%), between 11 of posterior epistaxis. and 15 mL in 10 nasal fossae (50%), and between 5 and 15 mL in 3 nasal fossae (15%). Failure to seal at any vol- Design: Human cadaveric study. ume occurred in 3 nasal fossae (15%). Bimodal seal (ie, complete seal at high [15 mL] and low volumes [4-7 mL], Materials: Twenty nasal fossae of 10 adult cadavers. but leakage in intermediate volumes) occurred in 3 na- sal fossae (15%). The balloon remained in the nasopha- Interventions: A Foley catheter (size 14) was inserted rynx under traction and did not slip past the choanal rim into the nasopharynx via each nostril. The catheter bal- to encroach on the middle and inferior turbinates until loon was inflated to its recommended maximum vol- the balloon volume was reduced to between 4 and 7 mL. ume with 15 mL of water. Firm traction was applied to The balloon slid out of the nose at a volume of 5 mL or the catheter. Colored liquid was instilled into the ipsi- less. The inflation volumes ranging from 8 to 12 mL were lateral aspect of the nasal cavity, and liquid leakage into statistically more effective in sealing the choana than lower the contralateral side was monitored using a nasoendo- volumes (4-7 mL) (P,.002, x2 test). -

Congenital Nasal Pyriform Aperture Stenosis
Published online: 2021-08-02 HEAD AND NECK Congenital nasal pyriform aperture stenosis: A rare cause of nasal airway obstruction in a neonate Elsa M Thomas, Sridhar Gibikote, Jyoti S Panwar, John Mathew1 Departments of Radiology and 1ENT and Head and Neck Surgery, Christian Medical College, Vellore, Tamil Nadu, India Correspondence: Dr. Elsa Mary Thomas, Department of Radiology, Christian Medical College, Vellore, Tamil Nadu - 632 004, India. E-mail: [email protected] Abstract Congenital nasal pyriform aperture stenosis (CNPAS) is a rare cause of nasal airway obstruction that clinically mimics choanal atresia, but needs to be differentiated from the latter because of the widely divergent modes of management. We present a case of CNPAS, to highlight the importance of recognizing the classic signs of CNPAS on cross-sectional imaging. Key words: Choanal atresia; CNPAS; holoprosencephaly; megaincisor; pyriform aperture stenosis Introduction the upper airways. This was negative for choanal atresia, but revealed multiple typical findings, which led to the Congenital nasal pyriform aperture stenosis (CNPAS), first diagnosis of CNPAS. The nasal cavity showed medial clinically described in 1989,[1] is a rare cause of neonatal approximation of the nasal processes of the maxilla, nasal airway obstruction. It typically presents with clinical causing marked narrowing of the pyriform apertures, features that may mimic posterior choanal atresia,[2] and it which measured 3 mm in width on an axial image, at the is important to differentiate it from the latter as there are level of the inferior meatus [Figure 1]. There was associated differences in patient management.[3] thinning of the anterior nasal septum. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Anatomic Variations of Paranasal Sinus on Multidetector Computed Tomography Examinations for Functional Endoscopic Sinus Surgery
MÜSBED 2013;3(2):102-106 DOI: 10.5455/musbed.20130410100848 Derleme / Review Anatomic Variations of Paranasal Sinus on Multidetector Computed Tomography Examinations for Functional Endoscopic Sinus Surgery Filiz Namdar Pekiner Department of Oral Diagnosis and Radiology, Faculty of Dentistry, Marmara University, Istanbul - Turkey Ya zış ma Ad re si / Add ress rep rint re qu ests to: Filiz Namdar Pekiner, Marmara University, Faculty of Dentistry, Department of Oral Diagnosis and Radiology, Nisantasi, Istanbul - Turkey Elekt ro nik pos ta ad re si / E-ma il add ress: [email protected] Ka bul ta ri hi / Da te of ac cep tan ce: 10 Nisan 2013 / April 10, 2013 ÖZET ABS TRACT Fonksiyonel endoskopik sinüs cerrahisinde mul- Anatomic variations of paranasal sinus tidetektör bilgisayarlı tomografide paranasal on multidetector computed tomography sinüslerin anatomik varyasyonları examinations for functional endoscopic sinus surgery Bilgisayarlı tomografi paranasal sinüslerin hastalıklarının ve fonksiyo- nel endoskopik sinüs cerrahisi ile tedavilerinin değerlendirilmesinde Computed tomography is excellent means of providing anatomical anatomik olarak sağladığı bilgi oldukça önemlidir. Paranasal sinüs- information of paranasal sinuses, assessing disease and guiding lerde izlenen anatomik varyasyonlar nadir değildir. Bu makalenin treatment with functional endoscopic sinus surgery (FESS). Common amacı paranasal sinüslerde izlenebilen bazı anatomik varyasyonları anatomical variations are not rare in the paranasal sinuses. The aim of sunmaktır. this article was presented radiological characteristics of some anatomic Anahtar sözcükler: Paranasal sinüsler, anatomik varyasyonlar, bilgi- variation in paranasal sinuses. sayarlı tomografi, fonksiyonel endoskopik sinüs cerrahisi Key words: Paranasal sinus, anatomical variation, computed tomography, functional endoscopic sinus surgery INTRODUCTION anatomy as shown on CT are of potential significance, it may predispose to certain pathologic conditions and Functional endoscopic sinus surgery (FESS) has been diseases (5). -

Dissertation on an OBSERVATIONAL STUDY COMPARING the EFFECT of SPHENOPALATINE ARTERY BLOCK on BLEEDING in ENDOSCOPIC SINUS SURGE
Dissertation On AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY Dissertation submitted to TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI For M.S.BRANCH IV (OTORHINOLARYNGOLOGY) Under the guidance of DR. F ANTHONY IRUDHAYARAJAN, M.S., D.L.O Professor & HOD, Department of ENT & Head and Neck Surgery, Govt. Stanley Medical College, Chennai. GOVERNMENT STANLEY MEDICAL COLLEGE THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY, CHENNAI-32, TAMILNADU APRIL 2017 CERTIFICATE This is to certify that this dissertation titled AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY is the original and bonafide work done by Dr. NIGIL SREEDHARAN under the guidance of Prof Dr F ANTHONY IRUDHAYARAJAN, M.S., DLO Professor & HOD, Department of ENT & Head and Neck Surgery at the Government Stanley Medical College & Hospital, Chennai – 600 001, during the tenure of his course in M.S. ENT from July-2014 to April- 2017 held under the regulation of the Tamilnadu Dr. M.G.R Medical University, Guindy, Chennai – 600 032. Prof Dr F Anthony Irudhayarajan, M.S., DLO Place : Chennai Professor & HOD, Date : .10.2016 Department of ENT & Head and Neck Surgery Government Stanley Medical College & Hospital, Chennai – 600 001. Dr. Isaac Christian Moses M.D, FICP, FACP Place: Chennai Dean, Date : .10.2016 Govt.Stanley Medical College, Chennai – 600 001. CERTIFICATE BY THE GUIDE This is to certify that this dissertation titled “AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY” is the original and bonafide work done by Dr NIGIL SREEDHARAN under my guidance and supervision at the Government Stanley Medical College & Hospital, Chennai – 600001, during the tenure of his course in M.S. -
The Axial Skeleton Visual Worksheet
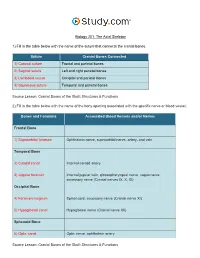
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -

A STUDY on POSITION of INFRAORBITAL FORAMEN Shaik Hussain Saheb 1, Shruthi B.N *2, Pavan P Havaldar 3
International Journal of Anatomy and Research, Int J Anat Res 2017, Vol 5(3.2):4257-60. ISSN 2321-4287 Original Research Article DOI: https://dx.doi.org/10.16965/ijar.2017.300 A STUDY ON POSITION OF INFRAORBITAL FORAMEN Shaik Hussain Saheb 1, Shruthi B.N *2, Pavan P Havaldar 3. 1 Department of Anatomy, JJM Medical College, Davangere, Karnataka, India. *2 Department of Anatomy, Rajarajeswari Medical College and hospital, Bangalore, Karnataka, India. 3 Department of Anatomy, Gadag institute of medical sciences, Gadag, Karnataka, India. ABSTRACT Background: The infraorbital foramen is located on the maxillary bone about 1 cm inferior to the infraorbital margin. The infraorbital nerve and vessels are transmitted through this foramen. The infraorbital nerve, the continuation of the maxillary or second division of the trigeminal nerve, is solely a sensory nerve. It traverses the inferior orbital fissure into the inferior orbital canal and emerges onto the face at the infraorbital foramen. It divides into several branches that innervate the skin and the mucous membrane of the midface, such as the lower eyelid, cheek, lateral aspect of the nose, upper lip, and the labial gum. Materials and Methods: Total 300 skulls were used for this study, the following mesearements were recorded, mean distance between the infra orbital foramen and the infra orbital margin on right and left side and average of it. The mean distance between the infra orbital foramen and the piriform aperature on right and left side measured and average of it also recorded. The mean distance between infra orbital foramen and the anterior nasal spine on right and left side measured. -
![NASAL CAVITY and PARANASAL SINUSES, PTERYGOPALATINE FOSSA, and ORAL CAVITY (Grant's Dissector [16Th Ed.] Pp](https://docslib.b-cdn.net/cover/6054/nasal-cavity-and-paranasal-sinuses-pterygopalatine-fossa-and-oral-cavity-grants-dissector-16th-ed-pp-1806054.webp)
NASAL CAVITY and PARANASAL SINUSES, PTERYGOPALATINE FOSSA, and ORAL CAVITY (Grant's Dissector [16Th Ed.] Pp
NASAL CAVITY AND PARANASAL SINUSES, PTERYGOPALATINE FOSSA, AND ORAL CAVITY (Grant's Dissector [16th Ed.] pp. 290-294, 300-303) TODAY’S GOALS (Nasal Cavity and Paranasal Sinuses): 1. Identify the boundaries of the nasal cavity 2. Identify the 3 principal structural components of the nasal septum 3. Identify the conchae, meatuses, and openings of the paranasal sinuses and nasolacrimal duct 4. Identify the openings of the auditory tube and sphenopalatine foramen and the nerve and blood supply to the nasal cavity, palatine tonsil, and soft palate 5. Identify the pterygopalatine fossa, the location of the pterygopalatine ganglion, and understand the distribution of terminal branches of the maxillary artery and nerve to their target areas DISSECTION NOTES: General comments: The nasal cavity is divided into right and left cavities by the nasal septum. The nostril or naris is the entrance to each nasal cavity and each nasal cavity communicates posteriorly with the nasopharynx through a choana or posterior nasal aperture. The roof of the nasal cavity is narrow and is represented by the nasal bone, cribriform plate of the ethmoid, and a portion of the sphenoid. The floor is the hard palate (consisting of the palatine processes of the maxilla and the horizontal portion of the palatine bone). The medial wall is represented by the nasal septum (Dissector p. 292, Fig. 7.69) and the lateral wall consists of the maxilla, lacrimal bone, portions of the ethmoid bone, the inferior nasal concha, and the perpendicular plate of the palatine bone (Dissector p. 291, Fig. 7.67). The conchae, or turbinates, are recognized as “scroll-like” extensions from the lateral wall and increase the surface area over which air travels through the nasal cavity (Dissector p. -

Investigations on the Growth Pattern of the Maxillary Sinus in Japanese Human Fetuses
Okajimas Folia Anat. Jpn., 71(5): 311-318, December, 1994 Investigations on the Growth Pattern of the Maxillary Sinus in Japanese Human Fetuses By Thomas KOPPE, Toshio YAMAMOTO, Osamu TANAKA and Hiroshi NAGAI Department of Anatomy, Okayama University, School of Dentistry Department of Anatomy, First Division, Shimane Medical University -Received for Publication, August 31, 1994- Key Words: Pneumatization, Maxillary sinus, Growth, Human fetuses Summary: The growth pattern of the maxillary sinus was analyzed using 18 human fetuses of both sexes between 9 and 21 weeks of age postconception. The paraffin embedded specimens were cut in series in the frontal and the transversal plane, respectively. The inner surface of the maxillary sinuses was redrawn and surrounded with a digitizer and then the volumes were calculated. A correlation analysis as well as a simple linear regression analysis between the values of the maxillary sinus, different linear values of the nasal cavity and the crown-rump length (CRL) served to prove possible growth relations. The maxillary sinus' Anlage was already identifiable in the 29.8 mm (CRL) fetus. From this first appearance, the maxillary sinus expands not only in posterior direction but also in anterior direction from 11 weeks onwards. The maxillary sinus volume increased from 0.0008 mm3 at the age of 9 weeks to more than 9 mm3 at the age of 21 weeks. The results of the statistical analysis indicated, that the relationship between the maxillary sinus' Anlage and the nasal cavity were strongly influenced by the body size (CRL). This study suggests, that the growth of the maxillary sinus follows special regularities in the early fetal development. -

Evolution of the Nasal Structure in the Lower Tetrapods
AM. ZOOLOCIST, 7:397-413 (1967). Evolution of the Nasal Structure in the Lower Tetrapods THOMAS S. PARSONS Department of Zoology, University of Toronto, Toronto, Ontario, Canada SYNOPSIS. The gross structure of the nasal cavities and the distribution of the various types of epithelium lining them are described briefly; each living order of amphibians and reptiles possesses a characteristic and distinctive pattern. In most groups there are two sensory areas, one lined by olfactory epithelium with nerve libers leading to the main olfactory bulb and the other by vomeronasal epithelium Downloaded from https://academic.oup.com/icb/article/7/3/397/244929 by guest on 04 October 2021 with fibers to the accessory bulb. All amniotes except turtles have the vomeronasal epithelium in a ventromedial outpocketing of the nose, the Jacobson's organ, and have one or more conchae projecting into the nasal cavity from the lateral wall. Although urodeles and turtles possess the simplest nasal structure, it is not possible to show that they are primitive or to define a basic pattern for either amphibians or reptiles; all the living orders are specialized and the nasal anatomy of extinct orders is unknown. Thus it is impossible, at present, to give a convincing picture of the course of nasal evolution in the lower tetrapods. Despite the rather optimistic title of this (1948, squamates), Stebbins (1948, squa- paper, I shall, unfortunately, be able to do mates), Bellairs and Boyd (1950, squa- iittle more than make a few guesses about mates), and Parsons (1959a, reptiles). Most the evolution of the nose. I can and will of the following descriptions are based on mention briefly the major features of the these works, although others, specifically nasal anatomy of the living orders of cited in various places, were also used.