Mouth-Level Nicotine Intake Estimates from Discarded Filter Butts to Examine Compensatory Smoking in Low Nicotine Cigarettes Tracy T
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Smoking Behavior and the Use of Cigarette Types Among University Student
E-ISSN 2240-0524 Journal of Educational and Social Research Vol 10 No 5 ISSN 2239-978X www.richtmann.org September 2020 . Research Article © 2020 Arisona et.al.. This is an open access article licensed under the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/) Smoking Behavior and the Use of Cigarette Types Among University Student Amalia Arisona Laili Rahayuwati Ayu Prawesti Habsyah Saparidah Agustina Faculty of Nursing, Universitas Padjadjaran, Indonesia DOI: https://doi.org/10.36941/jesr-2020-0100 Abstract The number of smokers is increasing every year in Indonesia. Cigarettes can cause several health problems and can even cause death. Aside from conventional cigarettes, e-cigarettes and shisha are starting to get the spotlight. The types of cigarettes include conventional cigarettes, electric cigarettes and shisha can cause health problems to both smokers and the people around them. The purpose of this study was to determine smoking behavior and the use of cigarette types in students. This research was quantitative descriptive. The population in this study were students who have smoked either the conventional, electric or shisha. The sampling technique used was accidental sampling with 384 students as the samples. The instrument in this study used a questionnaire that was independently developed by researchers with a total of 14 questions. The results of the data obtained were then analyzed using descriptive analysis presented in the form of a percentage. Based on the results of the study it was found that non-health students (90.6%) were more likely to smoke than health students (9.4%). -

Cigarette Smoking-Induced Endothelial Dysfunction: Molecular Mechanisms and Therapeutic Approaches
Cigarette Smoking-Induced Endothelial Dysfunction: Molecular Mechanisms and Therapeutic Approaches DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Tamer M. Abdelghany Graduate Program in Molecular, Cellular and Developmental Biology The Ohio State University 2013 Dissertation Committee: Dr. Jay L. Zweier, MD, Advisor Dr. Arthur Strauch III, PhD Dr. Amal Amer, MD PhD Copyright by Tamer M. Abdelghany 2013 Abstract Cigarette smoking (CS) remains the single largest preventable cause of death. Worldwide, smoking causes more than five million deaths annually and, according to the current trends, smoking may cause up to 10 million annual deaths by 2030. In the U.S. alone, approximately half a million adults die from smoking-related illnesses each year which represents ~ 19% of all deaths in the U.S., and among them 50,000 are killed due to exposure to secondhand smoke (SHS). Smoking is a major risk factor for cardiovascular disease (CVD). The crucial event of The CVD is the endothelial dysfunction (ED). Despite of the vast number of studies conducted to address this significant health problem, the exact mechanism by which CS induces ED is not fully understood. The ultimate goal of this thesis; therefore, is to study the mechanisms by which CS induces ED, aiming at the development of new therapeutic strategies that can be used in protection and/or reversal of CS-induced ED. In the first part of this study, we developed a well-characterized animal model for chronic secondhand smoke exposure (SHSE) to study the onset and severity of the disease. -
The Filter Fraud: Debunking the Myth of “Safer” As a Key New Strategy Of
THE FILTER FRAUD: DEBUNKING THE MYTH OF “SAFER” AS A KEY NEW STRATEGY OF TOBACCO CONTROL Alan Blum, MD, University of Alabama Center for the Study of Tobacco and Society, Tuscaloosa, AL, USA ([email protected]) Thomas E. Novotny, MD MPH, San Diego State University, Cigarette Butt Pollution Project, San Diego, CA, USA ([email protected]) Background Filters are a Health Hazard Although efforts have been made to eliminate the use of misleading • As with flavorings such as menthol, filters facilitate nicotine descriptors such as “low tar,” “lights,” and “mild” from cigarette addiction by making smoking less harsh and thus easier for marketing, the elimination of the cigarette filter, which is on 99.7% youth to start smoking. For existing smokers, the tobacco of cigarettes sold in United States, has been largely overlooked as a industry fostered consumer complacency and false security tobacco control strategy. The 2014 U.S. Surgeon General’s Report on about the implied protection that the filter could confer, the Health Consequences of Smoking and the 2001 U.S. National diminishing the urgency to quit smoking. Cancer Institute Monograph 13 report that the near-universal • Lung cancer risks among smokers have doubled for men and adoption by smokers of filtered cigarettes since their introduction in increased by almost 10 times for women from 1960-1980; the 1930s has not reduced these consumers’ risks for cancer and relative risks for and incidence of the more aggressive other diseases (1). Moreover, the non-biodegradable filter is the adenocarcinoma increased from 4.6 to19.0 among men and from main component of tobacco product waste in the environment. -

Cigarette Mainstream Smoke: the Evolution of Methods and Devices for Generation, Exposure and Collection * By
Beiträge zur Tabakforschung International Contributions to Tobacco Research Volume 27 @ No. 4 @ October 2016 DOI: 10.1515/cttr-2016-0015 Cigarette Mainstream Smoke: The Evolution of Methods and Devices for Generation, Exposure and Collection * by Hubert Klus 1, Barbara Boenke-Nimphius 2, and Lutz Müller 3 1 Oriongasse 9,3100 St. Pölten, Austria 2 Beiträge zur Tabakforschung International, Chausseestraße 51A, 10115 Berlin, Germany 3 Stralsunder Straße 1, 01109 Dresden, Germany SUMMARY (filters and traps) developed over time - some for very specific purposes - and refers to the perpetual problem of The objective of this review is to support tobacco scientists artifact formation by aging. [Beitr. Tabakforsch. Int. 27 when evaluating information published on smoking ma- (2016) 137–274] chines, and on cigarette mainstream smoke (in vivo and in vitro) exposure systems and collection devices. The intriguing development of smoking machines (mainly ZUSAMMENFASSUNG for cigarettes) is followed for more than 170 years - from the first simple set-ups in the 1840s to the sophisticated and Es ist die Intention dieser Übersicht, auf dem Gebiet des fully automated analytical smoking machines available Tabaks arbeitende Wissenschaftler zu unterstützen bei der today. Systems for the large-scale production of smoke Bewertung publizierter Informationen über Rauchmaschi- (condensate) for preparative work are equally considered. nen sowie über Systeme zur experimentellen Exposition (in The standardization of machine smoking methods and test vivo und in vitro) mit Zigarettenhauptstromrauch und pieces has solved several technical problems and produced Apparate zu dessen Sammlung. sensible rules but, at the same time, given rise to new Die sehr interessante Entwicklung von Rauchmaschinen controversies like the compatibility of artificial and human (vornehmlich für Zigaretten) wird über einen Zeitraum von smoking, and the implementation of more intense machine mehr als 170 Jahren nachgezeichnet - von den ersten ein- smoking regimes. -

Release of Carbon Granules from Cigarettes with Charcoal Filters
1997;6:33-4Q 33 Tob Control: first published as 10.1136/tc.6.1.33 on 1 March 1997. Downloaded from Release of carbon granules from cigarettes with charcoal filters John L Pauly, Sharon J Stegmeier, Andrew G Mayer, Joel D Lesses, Richard J Streck Abstract Keywords: cigarette filter; charcoal; fibres; gas Objective~~-To inspect cigarettes with a Most (more than 95%) of cigarettes marketed triple granular filter for charcoal granules 1 5 on the cut filter surface and, if present, to today in the United States have filters. " We determine whether the charcoal granules believe that the smoker perceives the filter of a on the filter are released during smoking. cigarette to be both safe and efficient. Design—400 Lark cigarettes in 20 packs However, recent observations in our laboratory were examined individually by each of challenged this view. For example, we have observed the release of cellulose acetate fibres three investigators for the presence of 1 charcoal granules on the cut surface of the from cigarette filters.' These filter fibres were: cellulose acetate filter. Without removing (a) observed trapped between the cellophane the cigarettes from the pack, the filters wrapper and the unopened pack of cigarettes; were examined with a stereo zoom micro- (b) present in the residue at the bottom of scope for charcoal granules. The percent- packs; (c) discharged from the filter when ciga- age of cigarettes that had charcoal rettes were tapped from a height of 3.5 cm or granules was defined, and charcoal dropped from 15 cm; (d) liberated when the granules on each filter were counted. -
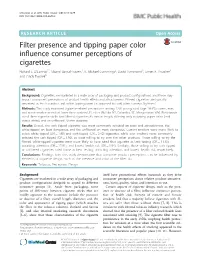
Filter Presence and Tipping Paper Color Influence Consumer Perceptions of Cigarettes Richard J
O’Connor et al. BMC Public Health (2015) 15:1279 DOI 10.1186/s12889-015-2643-z RESEARCH ARTICLE Open Access Filter presence and tipping paper color influence consumer perceptions of cigarettes Richard J. O’Connor1*, Maansi Bansal-Travers1, K. Michael Cummings2, David Hammond3, James F. Thrasher4 and Cindy Tworek5 Abstract Background: Cigarettes are marketed in a wide array of packaging and product configurations, and these may impact consumers’ perceptions of product health effects and attractiveness. Filtered cigarettes are typically perceived as less hazardous and white tipping paper (as opposed to cork) often conveys ‘lightness’. Methods: This study examined cigarette-related perceptions among 1220 young adult (age 18-35) current, ever, and never smokers recruited from three eastern U.S. cities (Buffalo NY, Columbia SC, Morgantown WV). Participants rated three cigarette sticks: two filtered cigarettes 85 mm in length, differing only in tipping paper color (cork versus white), and an unfiltered 70 mm cigarette. Results: Overall, the cork-tipped cigarette was most commonly selected on taste and attractiveness, the white-tipped on least dangerous, and the unfiltered on most dangerous. Current smokers were more likely to select white-tipped (OR = 1.98) and cork-tipped (OR = 3.42) cigarettes, while ever smokers more commonly selected the cork-tipped (OR = 1.96), as most willing to try over the other products. Those willing to try the filtered white-tipped cigarette were more likely to have rated that cigarette as best tasting (OR = 11.10), attracting attention (OR = 17.91), and lowest health risk (OR = 1.94). Similarly, those willing to try cork tipped or unfiltered cigarettes rated those as best testing, attracting attention, and lowest health risk, respectively. -

Nicotine & Tobacco Research
This article was downloaded by:[Canadian Research Knowledge Network] On: 7 February 2008 Access Details: [subscription number 770885181] Publisher: Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Nicotine & Tobacco Research Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713439766 Digital image analysis of cigarette filter staining to estimate smoke exposure Richard J. O'Connor a; Lynn T. Kozlowski b; David Hammond c; Tammy T. Vance a; Joseph P. Stitt d; K. Michael Cummings a a Department of Health Behavior, Roswell Park Cancer Institute, Buffalo, NY b Department of Biobehavioral Health, Pennsylvania State University, University Park, PA c Department of Health Studies, University of Waterloo, Waterloo, Canada d Applied Research Laboratory, Pennsylvania State University, University Park, PA Online Publication Date: 01 August 2007 To cite this Article: O'Connor, Richard J., Kozlowski, Lynn T., Hammond, David, Vance, Tammy T., Stitt, Joseph P. and Cummings, K. Michael (2007) 'Digital image analysis of cigarette filter staining to estimate smoke exposure', Nicotine & Tobacco Research, 9:8, 865 - 871 To link to this article: DOI: 10.1080/14622200701485026 URL: http://dx.doi.org/10.1080/14622200701485026 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. -

The 'Filter Fraud' Persists: the Tobacco Industry Is Still Using Filters To
Industry watch Tob Control: first published as 10.1136/tobaccocontrol-2020-056245 on 26 April 2021. Downloaded from The ‘filter fraud’ persists: the tobacco industry is still using filters to suggest lower health risks while destroying the environment Karen Evans- Reeves , Kathrin Lauber , Rosemary Hiscock Department for Health, FILTERS AND HARM Now tobacco companies are exploring the University of Bath, Bath, UK Despite being labelled the “deadliest fraud in the possibility of biodegradable filters. However, this history of human civilisation”,1 filter tips now should be regarded with caution. First, biodegrad- Correspondence to feature on almost every mass- produced cigarette able filters would still leach harmful chemicals Kathrin Lauber, Department for 2 16 Health, University of Bath, Bath smoked across the globe. After filters first appeared into the environment if discarded improperly BA2 7AY, UK; kl580@ bath. ac. uk in the 1860s as an attempt to protect against tobacco and second, it is likely that the tobacco industry flakes entering the mouth,3 the tobacco industry will use biodegradable filters as both a Corporate Received 17 September 2020 introduced modern cellulose acetate cigarette filters Social Responsibility and a marketing opportunity. Revised 1 February 2021 The potential unintended consequences would be Accepted 5 February 2021 in the 1950s to alleviate public concerns about smoking- related lung cancer.4 Filters and innova- reputation rehabilitation and consumers and non- tions to filters have been consistently marketed -

Anthropology of Tobacco
Anthropology of Tobacco Tobacco has become one of the most widely used and traded commodities on the planet. Reflecting contemporary anthropological interest in material culture studies, Anthropology of Tobacco makes the plant the centre of its own contentious, global story in which, instead of a passive commodity, tobacco becomes a powerful player in a global adventure involving people, corporations and public health. Bringing together a range of perspectives from the social and natural sciences as well as the arts and humanities, Anthropology of Tobacco weaves stories together from a range of historical, cross-cultural and literary sources and empirical research. These combine with contemporary anthropological theories of agency and cross-species relationships to offer fresh perspectives on how an apparently humble plant has progressed to world domination, and the consequences of it having done so. It also considers what needs to happen if, as some public health advocates would have it, we are seriously to imagine ‘a world without tobacco’. This book presents students, scholars and practitioners in anthropology, public health and social policy with unique and multiple perspectives on tobacco-human relations. Andrew Russell is Associate Professor in Anthropology at Durham University, UK, where he is a member of the Anthropology of Health Research Group. His research and teaching spans the sciences, arts and humanities, and mixes both theoretical and applied aspects. He has conducted research in Nepal, the UK and worldwide. Earlier books include The Social Basis of Medicine, which won the British Medical Association’s student textbook of the year award in 2010, and a number of edited volumes, the latest of which (co-edited with Elizabeth Rahman) is The Master Plant: Tobacco in Lowland South America. -

Seatca Packaging Design (25Feb2020)Web
No logos, colours, Pictorial health brand images or warnings used in promotional conjunction with information standardised packaging SMOKING CAUSES LUNG CANCER Pack surfaces in a standard colour Brand and product names in a standard colour and font 2020 Southeast Asia Tobacco Control Alliance Packaging Design Analysis to Support Standardised Packaging in the ASEAN Authors: Tan Yen Lian and Yong Check Yoon Editorial Team: Southeast Asia Tobacco Control Alliance Suggested citation: Tan YL. and Yong CY. (2020). Packaging Design Analysis to Support Standardised Packaging in the ASEAN, January 2020. Southeast Asia Tobacco Control Alliance (SEATCA), Bangkok. Thailand. Published by: Southeast Asia Tobacco Control Alliance (SEATCA) Thakolsuk Place, Room 2B, 115 Thoddamri Road, Dusit, Bangkok 10300 Thailand Telefax: +66 2 241 0082 Acknowledgment We would like to express our sincere gratitude to our country partners for their help in purchasing the cigarette packs from each country for the purpose of the study, which contributed to the development of this report. Disclaimer The information, ndings, interpretations, and conclusions expressed herein are those of the author(s) and do not necessarily reect the views of the funding organization, its sta, or its Board of Directors. While reasonable eorts have been made to ensure the accuracy of the information presented at the time of publication, SEATCA does not guarantee the completeness and accuracy of the information in this document and shall not be liable for any damages incurred as a result of its use. Any factual errors or omissions are unintentional. For any corrections, please contact SEATCA at [email protected]. © Southeast Asia Tobacco Control Alliance 2020 This document is the intellectual property of SEATCA and its authors. -

Degradation of Cellulose Acetate-Based Materials: a Review
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Springer - Publisher Connector J Polym Environ (2011) 19:152–165 DOI 10.1007/s10924-010-0258-0 ORIGINAL PAPER Degradation of Cellulose Acetate-Based Materials: A Review Juergen Puls • Steven A. Wilson • Dirk Ho¨lter Published online: 20 November 2010 Ó The Author(s) 2010. This article is published with open access at Springerlink.com Abstract Cellulose acetate polymer is used to make a enhanced by the addition of titanium dioxide, which is used variety of consumer products including textiles, plastic as a whitening agent in many consumer products. Photo films, and cigarette filters. A review of degradation degradation with TiO2 causes surface pitting, thus mechanisms, and the possible approaches to diminish the increasing a material’s surface area which enhances bio- environmental persistence of these materials, will clarify degradation. The combination of both photo and biodeg- the current and potential degradation rates of these prod- radation allows a synergy that enhances the overall ucts after disposal. Various studies have been conducted on degradation rate. The physical design of a consumer the biodegradability of cellulose acetate, but no review has product can also facilitate enhanced degradation rate, since been compiled which includes biological, chemical, and rates are highly influenced by the exposure to environ- photo chemical degradation mechanisms. Cellulose acetate mental conditions. The patent literature contains an abun- is prepared by acetylating cellulose, the most abundant dance of ideas for designing consumer products that are natural polymer. Cellulose is readily biodegraded by less persistent in the outdoors environment, and this review organisms that utilize cellulase enzymes, but due to the will include insights into enhanced degradability designs. -
TITANIUM DIOXIDE EU Tobacco Directive 2014/40/EU, Article 6, Priority Additive
REPORT TITANIUM DIOXIDE EU Tobacco Directive 2014/40/EU, Article 6, Priority Additive Priority Additives Tobacco Consortium KT&G Corporation 71, Beotkkot-gil, Daedeok-gu, Daejeon, Republic of Korea [email protected] Priority Additive Tobacco Consortium 1 Report for Priority Additive: Titanium Dioxide Table of Contents Table of Appendices ............................................................................................................................... 2 Executive Summary ................................................................................................................................ 3 1. Rationale for the Report ................................................................................................................. 5 2. Study Organization ......................................................................................................................... 6 A. Priority Additives Tobacco Consortium ............................................................................ 6 B. Test and Reference Cigarette Production ........................................................................ 7 C. Laboratories .......................................................................................................................... 7 D. Literature Review ................................................................................................................. 7 3. Comprehensive Literature Overview ............................................................................................. 8 A.