PG Series Ophthalmology Buster
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
RETINAL DISORDERS Eye63 (1)
RETINAL DISORDERS Eye63 (1) Retinal Disorders Last updated: May 9, 2019 CENTRAL RETINAL ARTERY OCCLUSION (CRAO) ............................................................................... 1 Pathophysiology & Ophthalmoscopy ............................................................................................... 1 Etiology ............................................................................................................................................ 2 Clinical Features ............................................................................................................................... 2 Diagnosis .......................................................................................................................................... 2 Treatment ......................................................................................................................................... 2 BRANCH RETINAL ARTERY OCCLUSION ................................................................................................ 3 CENTRAL RETINAL VEIN OCCLUSION (CRVO) ..................................................................................... 3 Pathophysiology & Etiology ............................................................................................................ 3 Clinical Features ............................................................................................................................... 3 Diagnosis ......................................................................................................................................... -

Genes in Eyecare Geneseyedoc 3 W.M
Genes in Eyecare geneseyedoc 3 W.M. Lyle and T.D. Williams 15 Mar 04 This information has been gathered from several sources; however, the principal source is V. A. McKusick’s Mendelian Inheritance in Man on CD-ROM. Baltimore, Johns Hopkins University Press, 1998. Other sources include McKusick’s, Mendelian Inheritance in Man. Catalogs of Human Genes and Genetic Disorders. Baltimore. Johns Hopkins University Press 1998 (12th edition). http://www.ncbi.nlm.nih.gov/Omim See also S.P.Daiger, L.S. Sullivan, and B.J.F. Rossiter Ret Net http://www.sph.uth.tmc.edu/Retnet disease.htm/. Also E.I. Traboulsi’s, Genetic Diseases of the Eye, New York, Oxford University Press, 1998. And Genetics in Primary Eyecare and Clinical Medicine by M.R. Seashore and R.S.Wappner, Appleton and Lange 1996. M. Ridley’s book Genome published in 2000 by Perennial provides additional information. Ridley estimates that we have 60,000 to 80,000 genes. See also R.M. Henig’s book The Monk in the Garden: The Lost and Found Genius of Gregor Mendel, published by Houghton Mifflin in 2001 which tells about the Father of Genetics. The 3rd edition of F. H. Roy’s book Ocular Syndromes and Systemic Diseases published by Lippincott Williams & Wilkins in 2002 facilitates differential diagnosis. Additional information is provided in D. Pavan-Langston’s Manual of Ocular Diagnosis and Therapy (5th edition) published by Lippincott Williams & Wilkins in 2002. M.A. Foote wrote Basic Human Genetics for Medical Writers in the AMWA Journal 2002;17:7-17. A compilation such as this might suggest that one gene = one disease. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -

Erounds on Wednesday Mornings, the West LA VA Optometry Residents & Student Participate in Erounds
West Los Angeles VA Health Care Center, Los Angeles, CA eRounds On Wednesday mornings, the West LA VA Optometry residents & student participate in eRounds. An eRounds typically includes presentation of one or more illustrative cases of the condition under consideration. During the case presentations, trainees are asked to identify normal and abnormal findings, list ocular differential diagnoses, list systemic differential diagnoses when applicable, and state options for ocular (and systemic) management. This is usually followed by a presentation of information on the topic, which may include epidemiology, presenting signs and symptoms of the condition, clinical diagnostic testing, ancillary testing, ocular and systemic management, etc. Topics include: Acne rosacea Conjunctival actinic keratosis Conjunctivochalasis Entropion and ectropion Floppy eyelid syndrome Fat prolapse Herpetic eye disease Hyphema Neovascular glaucoma Corneal degenerations Squamous cell carcinoma of the eyelid Basal cell carcinoma of the eyelid Sebaceous carcinoma Pemphigoid Phthisis bulbi Ocular manifestations of Valsalva maneuver Xanthelasma Branch retinal artery occlusion Central retinal artery occlusion Giant cell arteritis Fibrinoplatelet retinal embolus Ophthalmic artery occlusion Multiple Hollenhorst plaques Solitary Hollenhorst plaque Best dystrophy Retinitis pigmentosa Cone-rod dystrophies Optic disc drusen Tilted disc syndrome Stargardt’s disease Diabetic retinopathy Diabetes mellitus and ocular media disorders Diabetes mellitus and neuro-ophthalmic disease -

Prevalence of Amblyopia in Congenital Blepharoptosis: a Systematic Review and Meta-Analysis
Int J Ophthalmol, Vol. 12, No. 7, Jul.18, 2019 www.ijo.cn Tel: 8629-82245172 8629-82210956 Email: [email protected] ·Meta-Analysis· Prevalence of amblyopia in congenital blepharoptosis: a systematic review and Meta-analysis Jia-Ying Zhang1,2, Xiao-Wei Zhu1,2, Xia Ding1,2, Ming Lin1,2, Jin Li1,2 1Department of Ophthalmology, Shanghai Ninth People’s and management of amblyopia should be integral to the Hospital, Shanghai Jiao Tong University School of Medicine, treatment of congenital ptosis. Shanghai 200011, China ● KEYWORDS: amblyopia; congenital ptosis; blepharophimosis; 2Shanghai Key Laboratory of Orbital Diseases and Ocular systematic review Oncology, Shanghai 200011, China DOI:10.18240/ijo.2019.07.21 Correspondence to: Jin Li. Department of Ophthalmology, Shanghai Ninth Peolple’s Hospital, Shanghai Jiao Tong Citation: Zhang JY, Zhu XW, Ding X, Lin M, Li J. Prevalence of University School of Medicine, No.639, Zhizaoju Road, amblyopia in congenital blepharoptosis: a systematic review and Shanghai 200011, China. [email protected] Meta-analysis. Int J Ophthalmol 2019;12(7):1187-1193 Received: 2018-09-25 Accepted: 2019-03-05 INTRODUCTION Abstract ongenital blepharoptosis is an eyelid disorder that ● AIM: To conduct a systematic review and Meta-analysis of C is characterized by an involuntary drooping of the the published literature to evaluate the pooled prevalence upper eyelid since birth. Etiologically, myogenic factors are rate of amblyopia in patients with congenital ptosis. most common, referring to dysgenesis or weakness of the ● METHODS: We searched the PubMed, Embase, the levator muscle and sometimes the superior rectus muscle. Cochrane Central Register of Controlled Trials, China The etiological subtypes of congenital ptosis include simple National Knowledge Infrastructure, Wanfang Data, and congenital ptosis, blepharophimosis-ptosis-epicanthus inversus Chongqing VIP databases for studies reporting the syndrome (BPES), Marcus Gunn jaw-winking syndrome prevalence of amblyopia in patients with congenital ptosis. -

20-OPHTHALMOLOGY Cataract-Ds Brushfield-Down Synd Christmas
20-OPHTHALMOLOGY cataract-ds BrushfielD-Down synd christmas tree-myotonic dystrophy coronaRY-pubeRtY cuneiform-cortical(polyopia) cupuliform-post subcapsular(max vision loss) Elschnig pearl, ring of Soemmering-after(post capsule) experimenTal-Tyr def glassworker-infrared radiation grey(soft), yellow, amber, red(cataracta rubra), brown(cataracta brunescence), black(cat nigrans)(GYARBB)-nuclear(hard) heat-ionising radiation Membranous-HallerMan Streiff synd morgagnian-hypermature senile oildrop(revers)-galactossemia(G1PUT def) post cortical/bread crumb/polychromatic lustre/rainbow-complicated post polar-PHPV(persistent hyperplastic prim vitreous) radiational-post subcapsular riders-zonular/lamellar(vitD def, hypoparathy) roseTTe(ant cortex)-Trauma, concussion shield-atopic dermatitis snowstorm/flake-juvenile DM(aldose reductase def, T1>T2, sorbitol accumulat) star-electrocution sunflower/flower of petal-Wilson ds, chalcosis, penetrating trauma syndermatotic-atopic ds total-cong rubella zonular-galactossemia(galactokinase def) stage of cataract lamellar separation incipient/intumescence(freq change of glass) immature mature hypermature Aim4aiims.inmorgagnian sclerotic lens layer ant capsule ant epithelium lens fibre[66%H2O, 34%prot-aLp(Largest), Bet(most aBundant), γ(crystalline, soluble)] nucleus embryonic(0-3mthIUL) fetal(3-8mthIUL)-Y shape(suture) infantile(8mthIUL-puberty) adult(>puberty) cortex post capsule thinnest-post pole>ant pole thickest, most active cell-equator vitA absent in lens vitC tpt in lens by myoinositol H2O tpt in lens -

Amaurosis Fugax (Transient Monocular Or Binocular Vision Loss)
Amaurosis fugax (transient monocular or binocular vision loss) Syndee Givre, MD, PhD Gregory P Van Stavern, MD The next version of UpToDate (15.3) will be released in October 2007. INTRODUCTION AND DEFINITIONS — Amaurosis fugax (from the Greek "amaurosis," meaning dark, and the Latin "fugax," meaning fleeting) refers to a transient loss of vision in one or both eyes. Varied use of common terminology may cause some confusion when reading the literature. Some suggest that "amaurosis fugax" implies a vascular cause for the visual loss, but the term continues to be used when describing visual loss from any origin and involving one or both eyes. The term "transient monocular blindness" is also often used but is not ideal, since most patients do not experience complete loss of vision with the episode. "Transient monocular visual loss" (TMVL) and "transient binocular visual loss" (TBVL) are preferred to describe abrupt and temporary loss of vision in one or both eyes, since they carry no connotation regarding etiology. Transient visual loss, either monocular or binocular, reflects a heterogeneous group of disorders, some relatively benign and others with grave neurologic or ophthalmologic implications. The task of the clinician is to use the history and examination to localize the problem to a region in the visual pathways, identify potential etiologies, and, when indicated, perform a focused battery of laboratory tests to confirm or exclude certain causes. Therapeutic interventions and prognostic implications are specific to the underlying cause. This topic discusses transient visual loss. Other ocular and cerebral ischemic syndromes are discussed separately. APPROACH TO TRANSIENT VISUAL LOSS — By definition, patients with transient visual loss almost always present after the episode has resolved; hence, the neurologic and ophthalmologic examination is usually normal. -

Ocular Motility
10 Ocular Motility C. Denise Pensyl, William J. Benjamin linicians are faced with the challenge of differenti approximately 2 rnm, below which the effects of Cating the etiologies of asthenopia, blur, diplopia, reduced retinal illuminance and diffraction outweigh and headaches associated with the use of the eyes by the beneficial aspects ofan increase in depth offield and their patients. Oculomotor deficiencies can be one of reduction of ocular spherical aberration. The entrance several possible causes of such symptoms and are the pupil also controls blur circle size at the retina for object result of defects in the central nervous system, afferent rays not originating from the far point plane of the eye. or efferent nerve pathways, or local conditions of a The entrance pupil averages 3.5 mm in diameter in nature so as to impede appropriate oculomotor func adults under normal illumination but can range from tion. Oculomotor function will be extensively analyzed 1.3 mm to 10 mm. It is usually centered on the optic during phorometry (see Chapter 21) in terms of binoc axis of the eye but is displaced temporally away from ularity and muscle balance after the subjective refraction the visual axis or line of sight an average of 5 degrees. has been completed. This chapter focuses on clinical The entrance pupil is decentered approximately procedures that are typically used to analyze oculomo 0.15 mm nasally and 0.1 mm inferior to the geometric tor function before the subjective refraction is per center ofthe cornea. J This amount ofdecentration is not formed, though in some cases the practitioner may distinguished in casual observation or by the clinician's decide to use a few of these tests after the refraction is normal examination ofthe pupils. -
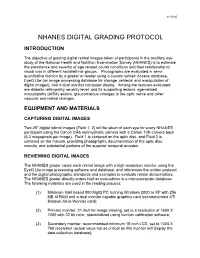
Nhanes Digital Grading Protocol
01/15/05 NHANES DIGITAL GRADING PROTOCOL INTRODUCTION The objective of grading digital retinal images taken of participants in the ancillary eye study of the National Health and Nutrition Examination Survey (NHANES) is to estimate the prevalence and severity of age-related ocular conditions and their relationship to visual loss in different racial/ethnic groups. Photographs are evaluated in semi- quantitative fashion by a grader or reader using a custom written Access database, EyeQ Lite (an image processing database for storage, retrieval and manipulation of digital images), and a dual monitor computer display. Among the features evaluated are diabetic retinopathy severity level, and its supporting lesions, age-related maculopathy (ARM) lesions, glaucomatous changes to the optic nerve and other vascular and retinal changes. EQUIPMENT AND MATERIALS CAPTURING DIGITAL IMAGES Two 45o digital retinal images (Field 1, 2) will be taken of each eye for every NHANES participant using the Canon CR6 nonmydriatic camera with a Canon 10D camera back (6.3 megapixels per image). Field 1 is centered on the optic disc, and Field 2 is centered on the macula, providing photographic documentation of the optic disc, macula, and substantial portions of the superior temporal arcades REVIEWING DIGITAL IMAGES The NHANES grader views each retinal image with a high resolution monitor using the EyeQ Lite image processing software and database, and references the written protocol and the digital photographic standards and examples to evaluate retinal abnormalities. -

Frontalis Sling: a Modified Simple Technique
Br J Ophthalmol: first published as 10.1136/bjo.69.6.443 on 1 June 1985. Downloaded from British Journal of Ophthalmology, 1985, 69, 443-445 Frontalis sling: a modified simple technique S M BETHARIA From Dr Rajendra Prasad Centrefor Ophthalmic Sciences, Ansari Nagar, New Delhi 110029, India SUMMARY A modified simple technique of brow suspension by using 4-0 Supramid (non- absorbable thread) suture and only one skin incision is described in 25 eyes of 15 cases of ptosis, including cases of congenital and mechanical ptosis and ptosis with Marcus Gunn phenomenon. This technique avoids the use of any special instruments such as the Reese ptosis knife and Wright needle. A sling operation is by far the easiest of all ptosis with the Marcus Gunn phenomenon after disinser- operations to perform. Though it may have im- tion of levator muscle from the tarsal plate (Table 1). portant disadvantages, such as the risk of lagophthal- mos and lid lag in down gaze, it is the operation of SURGICAL PROCEDURE choice for certain cases of gross bilateral ptosis with The operation is carried out under general anaes- poor levator function as seen in the blepharophimosis thesia. The first step is to lift the lid with the help of syndrome, cases of mechanical ptosis, and in severe the index finger just medial to the centre of the upper unilateral ptosis covering the pupillary area to pre- lid and observe the contour of the lid margin in vent amblyopia before a definitive levator operation relation to the limbus. This gives an approximate idea can be carried out. -

2015 NW Resconf Coursebook.Pdf
2015 NORTHWEST RESIDENTS CONFERENCE Pacific University College of Optometry – Jefferson 224 Friday, June 12 & Saturday, June 13, 2015 PROGRAM AGENDA Faculty: Carole Timpone, OD, FAAO, FNAP, Associate Dean of Clinical Programs and Director of Residencies, will oversee the event. Each resident will deliver a 30 minute presentation that includes responding to questions and comments from attendees. FRIDAY, JUNE 12, 2015 PAGES Rachael Lloyd, OD 1-11 Idiopathic Intracranial Hypertension – You Down VA Puget Sound Health Care System with PTC? Alisa Nola, OD Post Trauma Vision Syndrome Diagnosis and 12-21 Bright Eyes Vision Clinic Management using Visual Evoked Potentials (VEP) Mackenzie Macintyre, OD Ocriplasmin for Vitreomacular Adhesion: Boom 22-32 VA Portland Health Care System and Bust? Emily Liu, OD Plaque to the Future: Utilizing SD-OCT in the 33-41 VA Puget Sound Health Care System Management of CRAO and Retinal Emboli BREAK Haley McCoy, OD Ocular Sequelae of Common Systemic Medications 42-50 VA Portland Health Care System Magi Labib, OD Retinal Artery Occlusions Secondary to Illicit Drug 51-60 Lebanon VA Medical Center Use Victoria Roan, OD Oral Acetazolamide versus Topical Dorzolamide in 61-69 Jonathan Wainwright Memorial VAMC the Treatment of Retinitis Pigmentosa Kolten Kuntz, OD A Look into Current Trends and Future Advances in 70-76 Spokane VA Medical Center Cataract Surgery Frank Zheng, OD The Effects of Decentering Multifocal Soft Contact 77-87 Pacific University and Associated Clinics Lens Optics and its Relation to Distance Vision -
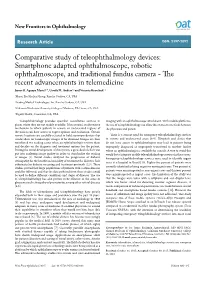
Comparative Study of Teleophthalmology Devices
New Frontiers in Ophthalmology Research Article ISSN: 2397-2092 Comparative study of teleophthalmology devices: Smartphone adapted ophthalmoscope, robotic ophthalmoscope, and traditional fundus camera - The recent advancements in telemedicine James B. Aguayo Martel1-4, Ursula M. Anders1,2 and Victoria Kravchuk1,2 1Martel Eye Medical Group, Rancho Cordova, CA, USA 2Leading Medical Technologies, Inc. Rancho Cordova, CA, USA 3California Northstate University College of Medicine, Elk Grove, CA, USA 4Dignity Health, Carmichael, CA, USA Teleophthalmology provides specialist consultation services in imaging with an ophthalmoscope attachment. With mobile platforms, places where they are not readily available. It has created an alternative the use of teleophthalmology can allow direct one on one feeds between mechanism to which patients in remote or underserved regions of the physician and patient. the nation can have access to expert opinion and evaluation. Certain remote locations are carefully selected to hold stationary devices that There is a current need for emergency teleophthalmology services would allow for funduscopic images to be obtained. Images are then in remote and underserved areas [8-9]. Hospitals and clinics that transferred to a reading center where an ophthalmologist reviews them do not have access to ophthalmologists may lead to patients being and decides on the diagnosis and treatment options for the patient. improperly diagnosed or improperly transferred to another facility During the initial development of this system, a great deal of effort was where an ophthalmologist is available for consult. A way to avoid this put into analyzing image quality in order to standardize the reading would be to integrate mobile teleophthalmology services in these areas.