Sleep Abnormalities Associated with Alcohol, Cannabis, Cocaine, and Opiate Use: a Comprehensive Review Gustavo A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
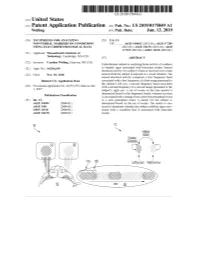
ANNNNNNNNNNNNNNNNNNNN 100A 006 Left Eye Input Right Eye Input
US 20190175049A1 ( 19) United States (12 ) Patent Application Publication (10 ) Pub. No. : US 2019 /0175049 A1 Welling ( 43 ) Pub . Date : Jun . 13 , 2019 ( 54 ) TECHNIQUES FOR ANALYZING (52 ) U . S . CI. NON -VERBAL MARKERS OF CONDITIONS CPC . .. A61B 5 /04842 (2013 . 01 ) ; A61B 5 / 7289 USING ELECTROPHYSIOLOGICAL DATA (2013 . 01) ; A61B 5 /0478 ( 2013 .01 ) ; A61B 5 /7225 ( 2013. 01 ) ; G06N 20 / 10 (2019 .01 ) (71 ) Applicant: Massachusetts Institute of Technology , Cambridge , MA (US ) ( 57 ) ABSTRACT (72 ) Inventor : Caroline Welling, Hanover, NH (US ) Embodiments related to analyzing brain activity of a subject to identify signs associated with binocular rivalry . Sensed ( 21 ) Appl. No. : 16 / 206, 639 electrical activity of a subject' s brain is received over a time period while the subject is exposed to a visual stimulus. The ( 22 ) Filed : Nov. 30 , 2018 sensed electrical activity comprises a first frequency band Related U . S . Application Data associated with a first frequency of a first image presented to the subject ' s left eye , a second frequency band associated (60 ) Provisional application No .62 / 593 , 535, filed on Dec . with a second frequency of a second image presented to the 1 , 2017 subject ' s right eye . A set of events in the time period is determined based on the frequency bands, wherein an event Publication Classification is associated with a change from a previous perceptual event (51 ) Int. Ci. to a new perceptual event. A metric for the subject is A61B 5 /0484 ( 2006 .01 ) determined based on the set of events . The metric is ana A61B 5 /00 ( 2006 .01 ) lyzed to determine whether the subject exhibits signs asso GO6N 20 / 10 (2006 .01 ) ciated with a condition that is associated with binocular A61B 5 /0478 ( 2006 .01 ) rivalry . -

Drugs Inducing Insomnia As an Adverse Effect
2 Drugs Inducing Insomnia as an Adverse Effect Ntambwe Malangu University of Limpopo, Medunsa Campus, School of Public Health, South Africa 1. Introduction Insomnia is a symptom, not a stand-alone disease. By definition, insomnia is "difficulty initiating or maintaining sleep, or both" or the perception of poor quality sleep (APA, 1994). As an adverse effect of medicines, it has been documented for several drugs. This chapter describes some drugs whose safety profile includes insomnia. In doing so, it discusses the mechanisms through which drug-induced insomnia occurs, the risk factors associated with its occurrence, and ends with some guidance on strategies to prevent and manage drug- induced insomnia. 2. How drugs induce insomnia There are several mechanisms involved in the induction of insomnia by drugs. Some drugs affects sleep negatively when being used, while others affect sleep and lead to insomnia when they are withdrawn. Drugs belonging to the first category include anticonvulsants, some antidepressants, steroids and central nervous stimulant drugs such amphetamine and caffeine. With regard to caffeine, the mechanism by which caffeine is able to promote wakefulness and insomnia has not been fully elucidated (Lieberman, 1992). However, it seems that, at the levels reached during normal consumption, caffeine exerts its action through antagonism of central adenosine receptors; thereby, it reduces physiologic sleepiness and enhances vigilance (Benington et al., 1993; Walsh et al., 1990; Rosenthal et al., 1991; Bonnet and Arand, 1994; Lorist et al., 1994). In contrast to caffeine, methamphetamine and methylphenidate produce wakefulness by increasing dopaminergic and noradrenergic neurotransmission (Gillman and Goodman, 1985). With regard to withdrawal, it may occur in 40% to 100% of patients treated chronically with benzodiazepines, and can persist for days or weeks following discontinuation. -

Effect of Repeated Gaboxadol Administration on Night Sleep and Next-Day Performance in Healthy Elderly Subjects
Neuropsychopharmacology (2005) 30, 833–841 & 2005 Nature Publishing Group All rights reserved 0893-133X/05 $30.00 www.neuropsychopharmacology.org Effect of Repeated Gaboxadol Administration on Night Sleep and Next-Day Performance in Healthy Elderly Subjects 1 2 ,3 1 Stefan Mathias , Josef Zihl , Axel Steiger* and Marike Lancel 1Section of Sleep Pharmacology, Max-Planck-Institute of Psychiatry, Munich, Germany; 2Section of Neuropsychology, Max-Planck-Institute of Psychiatry, Munich, Germany; 3Department of Psychiatry, Max-Planck-Institute of Psychiatry, Munich, Germany Aging is associated with dramatic reductions in sleep continuity and sleep intensity. Since gaboxadol, a selective GABAA receptor agonist, has been demonstrated to improve sleep consolidation and promote deep sleep, it may be an effective hypnotic, particularly for elderly patients with insomnia. In the present study, we investigated the effects of subchronic gaboxadol administration on nocturnal sleep and its residual effects during the next days in elderly subjects. This was a randomized, double-blind, placebo-controlled, balanced crossover study in 10 healthy elderly subjects without sleep complaints. The subjects were administered either placebo or 15 mg gaboxadol hydrochloride at bedtime on three consecutive nights. Sleep was recorded during each night from 2300 to 0700 h and tests assessing attention (target detection, stroop test) and memory function (visual form recognition, immediate word recall, digit span) were applied at 0900, 1400, and 1700 h during the following days. Compared with placebo, gaboxadol significantly shortened subjective sleep onset latency and increased self-rated sleep intensity and quality. Polysomnographic recordings showed that it significantly decreased the number of awakenings, the amount of intermittent wakefulness, and stage 1, and increased slow wave sleep and stage 2. -

GABA Receptors
D Reviews • BIOTREND Reviews • BIOTREND Reviews • BIOTREND Reviews • BIOTREND Reviews Review No.7 / 1-2011 GABA receptors Wolfgang Froestl , CNS & Chemistry Expert, AC Immune SA, PSE Building B - EPFL, CH-1015 Lausanne, Phone: +41 21 693 91 43, FAX: +41 21 693 91 20, E-mail: [email protected] GABA Activation of the GABA A receptor leads to an influx of chloride GABA ( -aminobutyric acid; Figure 1) is the most important and ions and to a hyperpolarization of the membrane. 16 subunits with γ most abundant inhibitory neurotransmitter in the mammalian molecular weights between 50 and 65 kD have been identified brain 1,2 , where it was first discovered in 1950 3-5 . It is a small achiral so far, 6 subunits, 3 subunits, 3 subunits, and the , , α β γ δ ε θ molecule with molecular weight of 103 g/mol and high water solu - and subunits 8,9 . π bility. At 25°C one gram of water can dissolve 1.3 grams of GABA. 2 Such a hydrophilic molecule (log P = -2.13, PSA = 63.3 Å ) cannot In the meantime all GABA A receptor binding sites have been eluci - cross the blood brain barrier. It is produced in the brain by decarb- dated in great detail. The GABA site is located at the interface oxylation of L-glutamic acid by the enzyme glutamic acid decarb- between and subunits. Benzodiazepines interact with subunit α β oxylase (GAD, EC 4.1.1.15). It is a neutral amino acid with pK = combinations ( ) ( ) , which is the most abundant combi - 1 α1 2 β2 2 γ2 4.23 and pK = 10.43. -

Gaboxadol Normalizes Behavioral Abnormalities in a Mouse Model of Fragile X Syndrome
ORIGINAL RESEARCH published: 25 June 2019 doi: 10.3389/fnbeh.2019.00141 Gaboxadol Normalizes Behavioral Abnormalities in a Mouse Model of Fragile X Syndrome Patricia Cogram 1,2,3,4, Robert M. J. Deacon 1,2,3,4, Jennifer L. Warner-Schmidt 5, Melanie J. von Schimmelmann 6, Brett S. Abrahams 6,7 and Matthew J. During 6,8* 1FRAXA-DVI, FRAXA Research Foundation, Boston, MA, United States, 2Centre for Systems Biotechnology, Biomedicine Division, Fraunhofer-Gesellschaft, Santiago, Chile, 3GEN.DDI Limited, London, United Kingdom, 4Institute of Ecology and Biodiversity (IEB), University of Chile, Santiago, Chile, 5NeuroJenic Consulting, LLC, Garden City, NY, United States, 6Ovid Therapeutics, New York, NY, United States, 7Department of Genetics and Neuroscience, Albert Einstein College of Medicine, Bronx, NY, United States, 8Department of Neurological Surgery and Molecular Virology, Immunology and Medical Genetics, Ohio State University College of Medicine, Columbus, OH, United States Fragile X syndrome (FXS) is the most common inherited form of intellectual disability and autism. FXS is also accompanied by attention problems, hyperactivity, anxiety, aggression, poor sleep, repetitive behaviors, and self-injury. Recent work supports the role of g-aminobutyric-acid (GABA), the primary inhibitory neurotransmitter in the brain, in mediating symptoms of FXS. Deficits in GABA machinery have been observed in a mouse model of FXS, including a loss of tonic inhibition in the amygdala, which is Edited by: Martine Ammassari-Teule, mediated by extrasynaptic GABAA receptors. Humans with FXS also show reduced Italian National Research Council GABAA receptor availability. Here, we sought to evaluate the potential of gaboxadol (CNR), Italy (also called OV101 and THIP), a selective and potent agonist for delta-subunit-containing Reviewed by: extrasynaptic GABA receptors (dSEGA), as a therapeutic agent for FXS by assessing Giulia Poggi, A University of Zurich, Switzerland its ability to normalize aberrant behaviors in a relatively uncharacterized mouse model Valerie J. -

Sleep Inducing Toothpaste Made with Natural Herbs and a Natural Hormone
Sleep inducing toothpaste made with natural herbs and a natural hormone Abstract A toothpaste composition for inducing sleep while simultaneously promoting intraoral cleanliness, which includes toothpaste base ingredients and at least one sleep- inducing natural herb or hormone. The sleep-inducing natural herbs and hormone are selected from the group consisting of Chamomile, Lemon Balm, Passion Flower, and Valerian, and the hormone Melatonin. The sleep-inducing natural herbs are in a range of 0.25% to 18% by weight of the composition. Description of the Invention FIELD OF THE INVENTION The following natural herbs and natural hormone in combination with toothpaste is used at night to improve sleep. The expected dose of toothpaste is calculated at 2 grams. The ingredients have been assessed for range of daily dose for best effects, toxicity in normal range, recommended proportion of each, and water solubility of key constituents. BACKGROUND OF THE INVENTION It is an object of the present invention to provide a sleep-inducing toothpaste or mouth spray which includes sleep-inducing natural herbs and a natural hormone. It is a further object of the present invention to provide a sleep-inducing toothpaste which includes toothpaste base ingredients and natural herbs being Chamomile, Lemon Balm, Passion Flower, Valerian and the natural hormone Melatonin. SUMMARY OF THE INVENTION A toothpaste composition is provided for inducing sleep while simultaneously promoting intraoral cleanliness, which includes toothpaste base ingredients and at least one sleep-inducing natural herb or hormone. The sleep-inducing natural herbs and hormone are selected from the group consisting of the natural herbs Chamomile, Lemon Balm, Passion Flower, and Valerian, and the natural hormone Melatonin. -

THE USE of MIRTAZAPINE AS a HYPNOTIC O Uso Da Mirtazapina Como Hipnótico Francisca Magalhães Scoralicka, Einstein Francisco Camargosa, Otávio Toledo Nóbregaa
ARTIGO ESPECIAL THE USE OF MIRTAZAPINE AS A HYPNOTIC O uso da mirtazapina como hipnótico Francisca Magalhães Scoralicka, Einstein Francisco Camargosa, Otávio Toledo Nóbregaa Prescription of approved hypnotics for insomnia decreased by more than 50%, whereas of antidepressive agents outstripped that of hypnotics. However, there is little data on their efficacy to treat insomnia, and many of these medications may be associated with known side effects. Antidepressants are associated with various effects on sleep patterns, depending on the intrinsic pharmacological properties of the active agent, such as degree of inhibition of serotonin or noradrenaline reuptake, effects on 5-HT1A and 5-HT2 receptors, action(s) at alpha-adrenoceptors, and/or histamine H1 sites. Mirtazapine is a noradrenergic and specific serotonergic antidepressive agent that acts by antagonizing alpha-2 adrenergic receptors and blocking 5-HT2 and 5-HT3 receptors. It has high affinity for histamine H1 receptors, low affinity for dopaminergic receptors, and lacks anticholinergic activity. In spite of these potential beneficial effects of mirtazapine on sleep, no placebo-controlled randomized clinical trials of ABSTRACT mirtazapine in primary insomniacs have been conducted. Mirtazapine was associated with improvements in sleep on normal sleepers and depressed patients. The most common side effects of mirtazapine, i.e. dry mouth, drowsiness, increased appetite and increased body weight, were mostly mild and transient. Considering its use in elderly people, this paper provides a revision about studies regarding mirtazapine for sleep disorders. KEYWORDS: sleep; antidepressive agents; sleep disorders; treatment� A prescrição de hipnóticos aprovados para insônia diminuiu em mais de 50%, enquanto de antidepressivos ultrapassou a dos primeiros. -

Ligand-Gated Ion Channels' British Journal of Pharmacology, Vol
Edinburgh Research Explorer The Concise Guide to PHARMACOLOGY 2015/16 Citation for published version: Alexander, SP, Peters, JA, Kelly, E, Marrion, N, Benson, HE, Faccenda, E, Pawson, AJ, Sharman, JL, Southan, C, Davies, JA & CGTP Collaborators 2015, 'The Concise Guide to PHARMACOLOGY 2015/16: Ligand-gated ion channels' British Journal of Pharmacology, vol. 172, no. 24, pp. 5870-5903. DOI: 10.1111/bph.13350 Digital Object Identifier (DOI): 10.1111/bph.13350 Link: Link to publication record in Edinburgh Research Explorer Document Version: Publisher's PDF, also known as Version of record Published In: British Journal of Pharmacology General rights Copyright for the publications made accessible via the Edinburgh Research Explorer is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights. Take down policy The University of Edinburgh has made every reasonable effort to ensure that Edinburgh Research Explorer content complies with UK legislation. If you believe that the public display of this file breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Download date: 05. Apr. 2019 S.P.H. Alexander et al. The Concise Guide to PHARMACOLOGY 2015/16: Ligand-gated ion channels. British Journal of Pharmacology (2015) 172, 5870–5903 THE CONCISE GUIDE TO PHARMACOLOGY 2015/16: Ligand-gated ion channels Stephen PH Alexander1, -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -

Melatonin Protects Against the Effects of Chronic Stress on Sexual Behaviour in Male Rats
MOTIVATION, EMOTION, FEEDING, DRINKING NEUROREPORT Melatonin protects against the effects of chronic stress on sexual behaviour in male rats Lori A. Brotto, Boris B. GorzalkaCA and Amanda K. LaMarre Department of Psychology, 2136 West Mall, Vancouver, BC, Canada V6T 1Z4 CACorresponding Author Received 9 July 2001; accepted 24 August 2001 The effects of chronic mild stress (CMS) on both sexual but not the effects on either spontaneous WDS or WDS in behaviour and wet dog shakes (WDS), a serotonergic type 2A response to the 5-HT2A agonist 1-(2,5-dimethoxy-4-iodophe- (5-HT2A) receptor-mediated behaviour, were explored in the nyl)-2-aminopropane, suggesting a mechanism of action other male rat. In addition, the possible attenuation of these effects than exclusive 5-HT2A antagonism. These results are the ®rst by chronic treatment with melatonin, a putative 5-HT2A to demonstrate that melatonin signi®cantly protects against the antagonist, was examined. The CMS procedure resulted in a detrimental effects of a chronic stressor on sexual behaviour. signi®cant increase in WDS and an overall decrease in all NeuroReport 12:3465±3469 & 2001 Lippincott Williams & aspects of sexual behaviour. Concurrent melatonin administra- Wilkins. tion attenuated the CMS-induced effects on sexual behaviour, Key words: Chronic mild stress; 5-HT2A receptors; Melatonin; Serotonin; Sexual behaviour INTRODUCTION vioural effect of melatonin is mediated via a reduction in The chronic mild stress (CMS) procedure, in which rats are 5-HT2A receptor activity rather than altered central 5-HT2A repeatedly exposed to a variety of mild stressors, is receptor density [8]. The demonstration that melatonin associated with behavioural and biochemical sequelae that reduces the concentration-dependent 5-HT2A receptor- are commonly associated with anhedonia [1]. -

ICADTS \(28-30 Août 2007, Seattle, USA\)
Annales de Toxicologie Analytique, vol. XIX, n° 4, 2007 ORAL PRESENTATIONS RESULTS: There were 7,673 external cause deaths in Victoria between July 2000 and June 2005. Of these, COMMUNICATIONS ORALES there were 2,086 (27%) external cause deaths contained a toxicology report where alcohol was identified as positive (greater than 0). A toxicology report was not Postmortem toxicology attached in 1,420 (18.5%) cases and the remaining Toxicologie postmortem 4,152 external cause cases contained a negative result for alcohol. Of cases with a toxicology report 455 Understanding forensic toxicology in (5.4%) had a blood alcohol concentration (BAC) of less than 0.06 g/100 mL. There were 564 (7.4%) detected relation to external-cause deaths with alcohol (0.06 g/100mL to <0.16 g/100mL) and 659 J. KILLIAN(1), O. DRUMMER(2), J. OZANNE- (8.6%) had a toxic level of alcohol (>0.16 g/100 mL). SMITH(1) Of all causes with alcohol detected, 2726 (37%) were (1) Monash University Accident Research Centre, due to intentional self-harm, followed by 2005 (27%) being transport related, 932 (12%) due to poisoning and Victoria, Australia 553 (7%) being fall related. The trends and themes of (2) Monash University Department of Forensic other drugs will also be reported especially in relation Medicine and Victorian Institute of Forensic Medicine, to traffic injuries. Victoria, Australia CONCLUSIONS: The study results provide, for the AIMS: Injuries are not only recognised as an important first time in Australia, a systematic examination of the public health problem, but are also one of the major epidemiology of licit and illicit drugs in injury deaths causes of death. -

Insomnia Disorder a VA Clinician’S Guide to Managing Insomnia Disorder (2019) Contents Insomnia Disorder
Insomnia Disorder A VA Clinician’s Guide to Managing Insomnia Disorder (2019) Contents Insomnia Disorder .................................................................................................... 3 Risks in elderly patients and patients with dementia .................................15 Background ................................................................................................................ 3 Provider perceptions vs reality ............................................................................16 Figure 1. Stepped Care for Management of Insomnia Disorder .............. 3 Figure 5. Weighing the potential risks versus benefits of Table 1. Brief summary of the ISI ......................................................................... 4 medication use .........................................................................................................16 Figure 2. Acute Insomnia to Insomnia Disorder ............................................ 5 Doxepin ........................................................................................................................17 Clinical Pearl ............................................................................................................... 5 Figure 6. Doxepin Use .............................................................................................18 Figure 3. Common causes of sleep disturbance ........................................... 6 Ramelteon ...................................................................................................................18