0.99) Or Low Genotyping Performance; None Were Excluded
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PARSANA-DISSERTATION-2020.Pdf
DECIPHERING TRANSCRIPTIONAL PATTERNS OF GENE REGULATION: A COMPUTATIONAL APPROACH by Princy Parsana A dissertation submitted to The Johns Hopkins University in conformity with the requirements for the degree of Doctor of Philosophy Baltimore, Maryland July, 2020 © 2020 Princy Parsana All rights reserved Abstract With rapid advancements in sequencing technology, we now have the ability to sequence the entire human genome, and to quantify expression of tens of thousands of genes from hundreds of individuals. This provides an extraordinary opportunity to learn phenotype relevant genomic patterns that can improve our understanding of molecular and cellular processes underlying a trait. The high dimensional nature of genomic data presents a range of computational and statistical challenges. This dissertation presents a compilation of projects that were driven by the motivation to efficiently capture gene regulatory patterns in the human transcriptome, while addressing statistical and computational challenges that accompany this data. We attempt to address two major difficulties in this domain: a) artifacts and noise in transcriptomic data, andb) limited statistical power. First, we present our work on investigating the effect of artifactual variation in gene expression data and its impact on trans-eQTL discovery. Here we performed an in-depth analysis of diverse pre-recorded covariates and latent confounders to understand their contribution to heterogeneity in gene expression measurements. Next, we discovered 673 trans-eQTLs across 16 human tissues using v6 data from the Genotype Tissue Expression (GTEx) project. Finally, we characterized two trait-associated trans-eQTLs; one in Skeletal Muscle and another in Thyroid. Second, we present a principal component based residualization method to correct gene expression measurements prior to reconstruction of co-expression networks. -

Number 2 February 2017 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Volume 1 - Number 1 May - September 1997 Volume 21 - Number 2 February 2017 Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Scope The Atlas of Genetics and Cytogenetics in Oncology and Haematology is a peer reviewed on-line journal in open access, devoted to genes, cytogenetics, and clinical entities in cancer, and cancer-prone diseases. It is made for and by: clinicians and researchers in cytogenetics, molecular biology, oncology, haematology, and pathology. One main scope of the Atlas is to conjugate the scientific information provided by cytogenetics/molecular genetics to the clinical setting (diagnostics, prognostics and therapeutic design), another is to provide an encyclopedic knowledge in cancer genetics. The Atlas deals with cancer research and genomics. It is at the crossroads of research, virtual medical university (university and post-university e-learning), and telemedicine. It contributes to "meta-medicine", this mediation, using information technology, between the increasing amount of knowledge and the individual, having to use the information. Towards a personalized medicine of cancer. It presents structured review articles ("cards") on: 1- Genes, 2- Leukemias, 3- Solid tumors, 4- Cancer-prone diseases, and also 5- "Deep insights": more traditional review articles on the above subjects and on surrounding topics. It also present 6- Case reports in hematology and 7- Educational items in the various related topics for students in Medicine and in Sciences. The Atlas of Genetics and Cytogenetics in Oncology and Haematology does not publish research articles. See also: http://documents.irevues.inist.fr/bitstream/handle/2042/56067/Scope.pdf Editorial correspondance Jean-Loup Huret, MD, PhD, Genetics, Department of Medical Information, University Hospital F-86021 Poitiers, France phone +33 5 49 44 45 46 [email protected] or [email protected] . -

Datasheet: VMA00937 Product Details
Datasheet: VMA00937 Description: MOUSE ANTI CIAPIN1 Specificity: CIAPIN1 Format: Purified Product Type: PrecisionAb Monoclonal Clone: AB04/1G9 Isotype: IgG1 Quantity: 100 µl Product Details Applications This product has been reported to work in the following applications. This information is derived from testing within our laboratories, peer-reviewed publications or personal communications from the originators. Please refer to references indicated for further information. For general protocol recommendations, please visit www.bio- rad-antibodies.com/protocols. Yes No Not Determined Suggested Dilution Western Blotting 1/1000 The PrecisionAb label is reserved for antibodies that meet the defined performance criteria within Bio-Rad's ongoing antibody validation programme. Click here to learn how we validate our PrecisionAb range. Where this product has not been tested for use in a particular technique this does not necessarily exclude its use in such procedures. Further optimization may be required dependent on sample type. Target Species Human Product Form Purified IgG - Liquid Preparation Mouse monoclonal antibody affinity purified on Protein G from tissue culture supernatant Buffer Solution Phosphate buffered saline Preservative 0.09% Sodium Azide Stabilisers Approx. Protein IgG concentration 1.0 mg/ml Concentrations Immunogen E. coli-derived recombinant protein of amino acids 1-312 of human CIAPIN1 Page 1 of 3 External Database Links UniProt: Q6FI81 Related reagents Entrez Gene: 57019 CIAPIN1 Related reagents Fusion Partners Spleen cells from immunised BALB/c mice were fused with cells of the mouse SP2/0 myeloma cell line Specificity Mouse anti CIAPIN1 antibody recognizes anamorsin, also known as cytokine-induced apoptosis inhibitor 1. CIAPIN1 is an electron transfer protein required for assembly of cytosolic iron-sulfur clusters, a family of cofactors critical for many cellular functions (Lipper et al. -
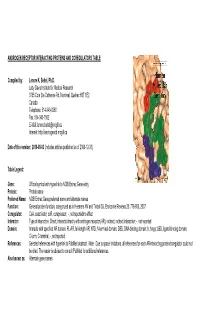
Androgen Receptor Interacting Proteins and Coregulators Table
ANDROGEN RECEPTOR INTERACTING PROTEINS AND COREGULATORS TABLE Compiled by: Lenore K. Beitel, Ph.D. Lady Davis Institute for Medical Research 3755 Cote Ste Catherine Rd, Montreal, Quebec H3T 1E2 Canada Telephone: 514-340-8260 Fax: 514-340-7502 E-Mail: [email protected] Internet: http://androgendb.mcgill.ca Date of this version: 2010-08-03 (includes articles published as of 2009-12-31) Table Legend: Gene: Official symbol with hyperlink to NCBI Entrez Gene entry Protein: Protein name Preferred Name: NCBI Entrez Gene preferred name and alternate names Function: General protein function, categorized as in Heemers HV and Tindall DJ. Endocrine Reviews 28: 778-808, 2007. Coregulator: CoA, coactivator; coR, corepressor; -, not reported/no effect Interactn: Type of interaction. Direct, interacts directly with androgen receptor (AR); indirect, indirect interaction; -, not reported Domain: Interacts with specified AR domain. FL-AR, full-length AR; NTD, N-terminal domain; DBD, DNA-binding domain; h, hinge; LBD, ligand-binding domain; C-term, C-terminal; -, not reported References: Selected references with hyperlink to PubMed abstract. Note: Due to space limitations, all references for each AR-interacting protein/coregulator could not be cited. The reader is advised to consult PubMed for additional references. Also known as: Alternate gene names Gene Protein Preferred Name Function Coregulator Interactn Domain References Also known as AATF AATF/Che-1 apoptosis cell cycle coA direct FL-AR Leister P et al. Signal Transduction 3:17-25, 2003 DED; CHE1; antagonizing regulator Burgdorf S et al. J Biol Chem 279:17524-17534, 2004 CHE-1; AATF transcription factor ACTB actin, beta actin, cytoplasmic 1; cytoskeletal coA - - Ting HJ et al. -

Redefining the Specificity of Phosphoinositide-Binding by Human
bioRxiv preprint doi: https://doi.org/10.1101/2020.06.20.163253; this version posted June 21, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. Redefining the specificity of phosphoinositide-binding by human PH domain-containing proteins Nilmani Singh1†, Adriana Reyes-Ordoñez1†, Michael A. Compagnone1, Jesus F. Moreno Castillo1, Benjamin J. Leslie2, Taekjip Ha2,3,4,5, Jie Chen1* 1Department of Cell & Developmental Biology, University of Illinois at Urbana-Champaign, Urbana, IL 61801; 2Department of Biophysics and Biophysical Chemistry, Johns Hopkins University School of Medicine, Baltimore, MD 21205; 3Department of Biophysics, Johns Hopkins University, Baltimore, MD 21218; 4Department of Biomedical Engineering, Johns Hopkins University, Baltimore, MD 21205; 5Howard Hughes Medical Institute, Baltimore, MD 21205, USA †These authors contributed equally to this work. *Correspondence: [email protected]. bioRxiv preprint doi: https://doi.org/10.1101/2020.06.20.163253; this version posted June 21, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. ABSTRACT Pleckstrin homology (PH) domains are presumed to bind phosphoinositides (PIPs), but specific interaction with and regulation by PIPs for most PH domain-containing proteins are unclear. Here we employed a single-molecule pulldown assay to study interactions of lipid vesicles with full-length proteins in mammalian whole cell lysates. -
Mechanisms Directing Receptor-Specific Gene Regulation
Mechanisms Directing Receptor-Specific Gene Regulation by the Androgen and Glucocorticoid Receptor Inaugural-Dissertation to obtain the academic degree Doctor rerum naturalium (Dr. rer. nat.) submitted to the Department of Biology, Chemistry, Pharmacy of Freie Universität Berlin by Marina Kulik • 2021 The dissertation was prepared under the supervision of Dr. Sebastiaan H. Meijsing at the Max Planck Institute for Molecular Genetics in Berlin from September 2015 to February 2021. 1st Reviewer: Dr. Sebastiaan Meijsing 2nd Reviewer: Prof. Dr. Markus Wahl Date of defense: 21.05.2021 1 Selbstständigkeitserklärung Hiermit bestätige ich, dass ich die vorliegende Arbeit selbstständig und unter Zuhilfenahme der angegebenen Literatur erstellt habe. Acknowledgments First of all, I would like to express my gratitude to my supervisor Sebastiaan Meijsing for his support and guidance during my PhD. I would like to thank Martin Vingron for the opportunity to be part of his research group and for the great collaborations. Especially, I would like to thank Stefan Haas for introducing me to the world of RNA-seq and Gözde Kibar, who contributed with her bioinformatical analyses to this work. I would like to thank Sarah Kinkley for her support and for giving me the opportunity to finish my PhD in her group. I wish to thank Stefan Prekovic, Isabel Mayayo-Peralta and Wilbert Zwart from the NKI in Amsterdam for sharing their expertise in “nuclear signaling” and the great collaboration. I am particularly grateful to Melissa Bothe, her computational analyses and support in the lab contributed a lot to this work. My special gratitude goes to Laura Glaser for her continuous advice and for freezing my cells in the evening countless times. -

Down Regulation of CIAPIN1 Reverses Multidrug Resistance in Human Breast Cancer Cells by Inhibiting MDR1
Molecules 2012, 17, 7595-7611; doi:10.3390/molecules17067595 OPEN ACCESS molecules ISSN 1420-3049 www.mdpi.com/journal/molecules Article Down Regulation of CIAPIN1 Reverses Multidrug Resistance in Human Breast Cancer Cells by Inhibiting MDR1 Dan Lu 1,†,*, Zhibo Xiao 2,†, Wenxiu Wang 1, Yuqing Xu 1, Shujian Gao 1, Lili Deng 1, Wen He 1, Yu Yang 1, Xiaofei Guo 1 and Xuemei Wang 1 1 Department of Oncology, the Second Affiliated Hospital of Harbin Medical University, Harbin 150086, China 2 Department of Plastic Surgery, the Second Affiliated Hospital of Harbin Medical University, Harbin 150086, China † These authors contributed equally to this work. * Author to whom correspondence should be addressed; E-Mail: [email protected]. Received: 13 March 2012; in revised form: 11 June 2012 / Accepted: 11 June 2012 / Published: 20 June 2012 Abstract: Cytokine-induced apoptosis inhibitor 1 (CIAPIN1), initially named anamorsin, a newly indentified antiapoptotic molecule is a downstream effector of the receptor tyrosine kinase-Ras signaling pathway. Current study has revealed that CIAPIN1 may have wide and important functions, especially due to its close correlations with malignant tumors. However whether or not it is involved in the multi-drug resistance (MDR) process of breast cancer has not been elucidated. To explore the effect of CIAPIN1 on MDR, we examined the expression of P-gp and CIAPIN1 by immunohistochemistry and found there was positive correlation between them. Then we successfully interfered with RNA translation by the infection of siRNA of CIAPIN1 into MCF7/ADM breast cancer cell lines through a lentivirus, and the expression of the target gene was significantly inhibited. -

Noelia Díaz Blanco
Effects of environmental factors on the gonadal transcriptome of European sea bass (Dicentrarchus labrax), juvenile growth and sex ratios Noelia Díaz Blanco Ph.D. thesis 2014 Submitted in partial fulfillment of the requirements for the Ph.D. degree from the Universitat Pompeu Fabra (UPF). This work has been carried out at the Group of Biology of Reproduction (GBR), at the Department of Renewable Marine Resources of the Institute of Marine Sciences (ICM-CSIC). Thesis supervisor: Dr. Francesc Piferrer Professor d’Investigació Institut de Ciències del Mar (ICM-CSIC) i ii A mis padres A Xavi iii iv Acknowledgements This thesis has been made possible by the support of many people who in one way or another, many times unknowingly, gave me the strength to overcome this "long and winding road". First of all, I would like to thank my supervisor, Dr. Francesc Piferrer, for his patience, guidance and wise advice throughout all this Ph.D. experience. But above all, for the trust he placed on me almost seven years ago when he offered me the opportunity to be part of his team. Thanks also for teaching me how to question always everything, for sharing with me your enthusiasm for science and for giving me the opportunity of learning from you by participating in many projects, collaborations and scientific meetings. I am also thankful to my colleagues (former and present Group of Biology of Reproduction members) for your support and encouragement throughout this journey. To the “exGBRs”, thanks for helping me with my first steps into this world. Working as an undergrad with you Dr. -

Variation in Protein Coding Genes Identifies Information
bioRxiv preprint doi: https://doi.org/10.1101/679456; this version posted June 21, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Animal complexity and information flow 1 1 2 3 4 5 Variation in protein coding genes identifies information flow as a contributor to 6 animal complexity 7 8 Jack Dean, Daniela Lopes Cardoso and Colin Sharpe* 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Institute of Biological and Biomedical Sciences 25 School of Biological Science 26 University of Portsmouth, 27 Portsmouth, UK 28 PO16 7YH 29 30 * Author for correspondence 31 [email protected] 32 33 Orcid numbers: 34 DLC: 0000-0003-2683-1745 35 CS: 0000-0002-5022-0840 36 37 38 39 40 41 42 43 44 45 46 47 48 49 Abstract bioRxiv preprint doi: https://doi.org/10.1101/679456; this version posted June 21, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Animal complexity and information flow 2 1 Across the metazoans there is a trend towards greater organismal complexity. How 2 complexity is generated, however, is uncertain. Since C.elegans and humans have 3 approximately the same number of genes, the explanation will depend on how genes are 4 used, rather than their absolute number. -

Identification of Potential Key Genes and Pathway Linked with Sporadic Creutzfeldt-Jakob Disease Based on Integrated Bioinformatics Analyses
medRxiv preprint doi: https://doi.org/10.1101/2020.12.21.20248688; this version posted December 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. Identification of potential key genes and pathway linked with sporadic Creutzfeldt-Jakob disease based on integrated bioinformatics analyses Basavaraj Vastrad1, Chanabasayya Vastrad*2 , Iranna Kotturshetti 1. Department of Biochemistry, Basaveshwar College of Pharmacy, Gadag, Karnataka 582103, India. 2. Biostatistics and Bioinformatics, Chanabasava Nilaya, Bharthinagar, Dharwad 580001, Karanataka, India. 3. Department of Ayurveda, Rajiv Gandhi Education Society`s Ayurvedic Medical College, Ron, Karnataka 562209, India. * Chanabasayya Vastrad [email protected] Ph: +919480073398 Chanabasava Nilaya, Bharthinagar, Dharwad 580001 , Karanataka, India NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. medRxiv preprint doi: https://doi.org/10.1101/2020.12.21.20248688; this version posted December 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. Abstract Sporadic Creutzfeldt-Jakob disease (sCJD) is neurodegenerative disease also called prion disease linked with poor prognosis. The aim of the current study was to illuminate the underlying molecular mechanisms of sCJD. The mRNA microarray dataset GSE124571 was downloaded from the Gene Expression Omnibus database. Differentially expressed genes (DEGs) were screened. -

Metastatic Adrenocortical Carcinoma Displays Higher Mutation Rate and Tumor Heterogeneity Than Primary Tumors
ARTICLE DOI: 10.1038/s41467-018-06366-z OPEN Metastatic adrenocortical carcinoma displays higher mutation rate and tumor heterogeneity than primary tumors Sudheer Kumar Gara1, Justin Lack2, Lisa Zhang1, Emerson Harris1, Margaret Cam2 & Electron Kebebew1,3 Adrenocortical cancer (ACC) is a rare cancer with poor prognosis and high mortality due to metastatic disease. All reported genetic alterations have been in primary ACC, and it is 1234567890():,; unknown if there is molecular heterogeneity in ACC. Here, we report the genetic changes associated with metastatic ACC compared to primary ACCs and tumor heterogeneity. We performed whole-exome sequencing of 33 metastatic tumors. The overall mutation rate (per megabase) in metastatic tumors was 2.8-fold higher than primary ACC tumor samples. We found tumor heterogeneity among different metastatic sites in ACC and discovered recurrent mutations in several novel genes. We observed 37–57% overlap in genes that are mutated among different metastatic sites within the same patient. We also identified new therapeutic targets in recurrent and metastatic ACC not previously described in primary ACCs. 1 Endocrine Oncology Branch, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892, USA. 2 Center for Cancer Research, Collaborative Bioinformatics Resource, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892, USA. 3 Department of Surgery and Stanford Cancer Institute, Stanford University, Stanford, CA 94305, USA. Correspondence and requests for materials should be addressed to E.K. (email: [email protected]) NATURE COMMUNICATIONS | (2018) 9:4172 | DOI: 10.1038/s41467-018-06366-z | www.nature.com/naturecommunications 1 ARTICLE NATURE COMMUNICATIONS | DOI: 10.1038/s41467-018-06366-z drenocortical carcinoma (ACC) is a rare malignancy with types including primary ACC from the TCGA to understand our A0.7–2 cases per million per year1,2. -
Thermal Manipulation of the Chicken Embryo Triggers Differential Gene
Loyau et al. BMC Genomics (2016) 17:329 DOI 10.1186/s12864-016-2661-y RESEARCH ARTICLE Open Access Thermal manipulation of the chicken embryo triggers differential gene expression in response to a later heat challenge Thomas Loyau1, Christelle Hennequet-Antier1, Vincent Coustham1, Cécile Berri1, Marie Leduc1, Sabine Crochet1, Mélanie Sannier1, Michel Jacques Duclos1, Sandrine Mignon-Grasteau1, Sophie Tesseraud1, Aurélien Brionne1, Sonia Métayer-Coustard1, Marco Moroldo2, Jérôme Lecardonnel2, Patrice Martin3, Sandrine Lagarrigue4, Shlomo Yahav5 and Anne Collin1* Abstract Background: Meat type chickens have limited capacities to cope with high environmental temperatures, this sometimes leading to mortality on farms and subsequent economic losses. A strategy to alleviate this problem is to enhance adaptive capacities to face heat exposure using thermal manipulation (TM) during embryogenesis. This strategy was shown to improve thermotolerance during their life span. The aim of this study was to determine the effects of TM (39.5 °C, 12 h/24 vs 37.8 °C from d7 to d16 of embryogenesis) and of a subsequent heat challenge (32 °C for 5 h) applied on d34 on gene expression in the Pectoralis major muscle (PM). A chicken gene expression microarray (8 × 60 K) was used to compare muscle gene expression profiles of Control (C characterized by relatively high body temperatures, Tb) and TM chickens (characterized by a relatively low Tb) reared at 21 °C and at 32 °C (CHC and TMHC, respectively) in a dye-swap design with four comparisons and 8 broilers per treatment. Real-time quantitative PCR (RT-qPCR) was subsequently performed to validate differential expression in each comparison.