Pressure Ulcers: Prevention, Evaluation, and Management
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Brief History of Pressure Ulcer Measurement in England: the Last 20 Years
EDITORIAL A brief history of pressure ulcer measurement in England: the last 20 years ressure ulcers (PU) have long been Measuring pressure ulcers: recognised as a challenge to healthcare, are prevalence and incidence a cause of significant pain and distress for During this time, the most reported forms of Ppatients and are costly for healthcare providers measurement have been prevalence and incidence. in term of finances and use of human resource Prevalence is the proportion of a population (Guest et al, 2020). who have a specific characteristic in a given This paper, the first in a series of three, describes time period. Therefore, the prevalence of PUs is the predominant methods that have been used to the proportion of a defined patient population JACQUI FLETCHER OBE capture the prevalence of PUs in England over the with pressure damage during a specified time Clinical Lead Pressure Ulcer last 20 years. The second paper will describe the period. Incidence is the number of specified new Workstream National Wound proposed system for national PU measurement events, during a specified period in a specified Care Strategy Clinical Editor, Wounds UK in England and the third paper will outline population. Therefore, the incidence of pressure proposals for implementing this system to drive damage is the number of people in a defined quality improvement. patient population who develop a new PU during a specified time period. BACKGROUND Prevalence of pressure damage is a good Measurement of the occurrence of PUs (also indicator of the overall burden and clinical known as pressure sores, decubitus ulcers, workload related to pressure damage but does pressure injury and bed sores) has been a part of not identify when and where the PU occurred, nursing activity for many years. -

The Pressure Sore Case: a Medical Perspective
Marquette Elder's Advisor Volume 2 Article 7 Issue 2 Fall The rP essure Sore Case: A Medical Perspective Jeffrey M. Levine Follow this and additional works at: http://scholarship.law.marquette.edu/elders Part of the Elder Law Commons Repository Citation Levine, Jeffrey M. (2000) "The rP essure Sore Case: A Medical Perspective," Marquette Elder's Advisor: Vol. 2: Iss. 2, Article 7. Available at: http://scholarship.law.marquette.edu/elders/vol2/iss2/7 This Featured Article is brought to you for free and open access by the Journals at Marquette Law Scholarly Commons. It has been accepted for inclusion in Marquette Elder's Advisor by an authorized administrator of Marquette Law Scholarly Commons. For more information, please contact [email protected]. The Pressure Sore Case: A Medical Perspective Although bedsores sometimes result dents.7 As a result, malpractice litigation related to pressure sores exploded in the 1990s.1 from inadequate care, not all cases Clinical Practice Guidelines involving pressure ulcers merit a law- Define Pressure Sores suit. This article adopts a medical per- Clinical practice guidelines define a pressure ulcer as "[a]ny skin lesion, usually over a bony promi- spective in its consideration of the pres- nence, caused by unrelieved pressure resulting in damage of underlying tissue." 9 The incidence of sure sore case, particularlywhen evalu- pressure ulcers in nursing homes is 0.20 to 0.56 per 1,000 resident-days, which may increase to 14 per ating deviation from the standard of 1,000 resident-days among those at high risk.' ° Commonly affected sites, comprising approximate- care. -
Arterial Leg Ulcer Clinical Pathway
Waterloo Wellington Integrated Wound Care Program Evidence-Based Wound Care Arterial Leg Ulcer Clinical Pathway 0-7 Days Expected Outcomes Notes Most Responsible Physician(MRP)/Nurse Practitioner (NP) Refer patient to ‘Care Connects’ if no responsible practitioner currently involved with patient identified/informed Determine if MRP/NP is part of Family Health Team (FHT) or Community Health Centre (CHC) and consider additional supports available Medical/surgical history and co-morbidity management Risk factors include: Chronic renal disease considered within care plan Smoking Congestive heart failure Diabetes mellitus Impaired liver function Hyperlipidemia Use of systemic steroids, Hypertension immunosuppressive and chemotherapy Coronary artery disease >70 years of age History of cerebral vascular accident Age 50-69 years with history of diabetes (CVA) or smoking Low hemoglobin < 50 years with diabetes and one other Obesity atherosclerotic factor Poor nutrition History of vascular surgery or deep vein Decreased thyroid function thrombosis Psoriasis Bleeding disorders Autoimmune diseases Family history of arterial disease Medication reconciliation and their impact on wound healing Prescription, non-prescription, naturopathic and illicit drug use (including e-cigarettes, reviewed inhaled substances and nicotine replacement therapy) Medications that can affect healing include: chemotherapy, anticoagulants, antiplatelets, corticosteroids, vasoconstrictors, antihypertensives, diuretics and immunosepressive drugs Other -

Wound Classification
Wound Classification Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State University Welcome! Thank you for joining this webinar about how to assess and measure a wound. 2 A Little About Myself… • Associate professor at Montana State University • Executive editor of the Journal of the World Council of Enterstomal Therapists (JWCET) and WCET International Ostomy Guidelines (2014) • Editorial board member of Ostomy Wound Management and Advances in Skin and Wound Care • Legal consultant • Former NPUAP board member 3 Today We Will Talk About • How to assess a wound • How to measure a wound Please make a note of your questions. Your Quality Improvement (QI) Specialists will follow up with you after this webinar to address them. 4 Assessing and Measuring Wounds • You completed a skin assessment and found a wound. • Now you need to determine what type of wound you found. • If it is a pressure ulcer, you need to determine the stage. 5 Assessing and Measuring Wounds This is important because— • Each type of wound has a different etiology. • Treatment may be very different. However— • Not all wounds are clear cut. • The cause may be multifactoral. 6 Types of Wounds • Vascular (arterial, venous, and mixed) • Neuropathic (diabetic) • Moisture-associated dermatitis • Skin tear • Pressure ulcer 7 Mixed Etiologies Many wounds have mixed etiologies. • There may be both venous and arterial insufficiency. • There may be diabetes and pressure characteristics. 8 Moisture-Associated Skin Damage • Also called perineal dermatitis, diaper rash, incontinence-associated dermatitis (often confused with pressure ulcers) • An inflammation of the skin in the perineal area, on and between the buttocks, into the skin folds, and down the inner thighs • Scaling of the skin with papule and vesicle formation: – These may open, with “weeping” of the skin, which exacerbates skin damage. -

Pressure Ulcer Staging Cards and Skin Inspection Opportunities.Indd
Pressure Ulcer Staging Pressure Ulcer Staging Suspected Deep Tissue Injury (sDTI): Purple or maroon localized area of discolored Suspected Deep Tissue Injury (sDTI): Purple or maroon localized area of discolored intact skin or blood-fi lled blister due to damage of underlying soft tissue from pressure intact skin or blood-fi lled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, fi rm, mushy, boggy, and/or shear. The area may be preceded by tissue that is painful, fi rm, mushy, boggy, warmer or cooler as compared to adjacent tissue. warmer or cooler as compared to adjacent tissue. Stage 1: Intact skin with non- Stage 1: Intact skin with non- blanchable redness of a localized blanchable redness of a localized area usually over a bony prominence. area usually over a bony prominence. Darkly pigmented skin may not have Darkly pigmented skin may not have visible blanching; its color may differ visible blanching; its color may differ from surrounding area. from surrounding area. Stage 2: Partial thickness loss of Stage 2: Partial thickness loss of dermis presenting as a shallow open dermis presenting as a shallow open ulcer with a red pink wound bed, ulcer with a red pink wound bed, without slough. May also present as without slough. May also present as an intact or open/ruptured serum- an intact or open/ruptured serum- fi lled blister. fi lled blister. Stage 3: Full thickness tissue loss. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. -
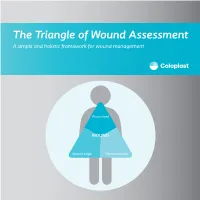
The Triangle of Wound Assessment a Simple and Holistic Framework for Wound Management
The Triangle of Wound Assessment A simple and holistic framework for wound management Wound bed WOUND Wound edge Periwound skin We asked healthcare professionals around the world about their priorities ? for wound care We found that most people Respondents said that treating wounds are not protecting the periwound specialists in a hospital1 skin is very important1 Approximately Up to 79% of wounds are 70% of being treated in wounds are the community2 surrounded by unhealthy skin3 2 ...none However, in a recent met all of the study of 14 wound criteria for assessment tools ... optimal wound assessment4 The Triangle of Wound Assessment is a holistic framework that allows practitioners üto assess and manage all areas of the wound, including the periwound skin. It is a simple and systematic approach that guides the user Wound bed from complete wound WOUND assessment to setting management goals, and Wound edge Periwound skin selecting the optimal treatment. 3 The Triangle of Wound Assessment offers a systematic approach to wound management Optimal wound management starts with a holistic wound assessment. This will help to more efficiently set management goals, which will increase the potential for better treatment outcomes. Assessment Management Goals Treatment 4 This is achieved through a holistic framework The Triangle of Wound Assessment provides a framework to assess all three areas of the wound while remembering the patient behind the wound within their social context. Patient Wound bed Social context WOUND Wound Wound edge Periwound skin 5 It’s not just about the wound but also the patient behind the wound Optimal management of the wound starts with assessing the patient behind the wound, and the social context in which the patient lives. -

Guideline: Wound Bed Preparation for Healable and Non Healable Wounds
British Columbia Provincial Nursing Skin and Wound Committee Guideline: Wound Bed Preparation for Healable and Non Healable Wounds Developed by the BC Provincial Nursing Skin and Wound Committee in collaboration with Wound Clinicians from: / TITLE Guideline: Wound Bed Preparation for Healable and Non-Healable Wounds in Adults & Children1 Practice Level Nurses in accordance with health authority and agency policy. Conservative sharp wound debridement (CSWD) is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 2 CRNBC states that registered nurses must successfully complete additional education and follow an established guideline when carrying out CSWD. Biological debridement therapy is a restricted activity according to the Nurse’s (Registered) and Nurse Practitioner Regulation. 3 CRNBC states that registered nurses must follow an established guideline when carrying out biological debridement. Clients 4 with wounds needing wound bed preparation require an interprofessional approach to provide comprehensive, evidence-based assessment and treatment. This clinical practice guideline focuses solely on the role of the nurse, as one member of the interprofessional team providing care to these clients. Background Factors affecting wound healability include the presence of adequate circulation in the area of the wound, wound related factors such as the size and duration of the wound, the ability to treat the cause of the wound and the presence of risk factors impacting wound healing. While many wounds heal, others are determined to be non-healing or slow-to-heal based on the presence or absence of these factors. Wound healability must be determined prior to debridement and moist wound healing. Although wound healing normally occurs in a predictable fashion, wound healing trajectories can be heterogeneous and non- uniform resulting is delayed wound healing for some clients. -

The Care of a Patient with Fournier's Gangrene
CASE REPORT The care of a patient with Fournier’s gangrene Esma Özşaker, Asst. Prof.,1 Meryem Yavuz, Prof.,1 Yasemin Altınbaş, MSc.,1 Burçak Şahin Köze, MSc.,1 Birgül Nurülke, MSc.2 1Department of Surgical Nursing, Ege University Faculty of Nursing, Izmir; 2Department of Urology, Ege University Faculty of Medicine Hospital, Izmir ABSTRACT Fournier’s gangrene is a rare, necrotizing fasciitis of the genitals and perineum caused by a mixture of aerobic and anaerobic microor- ganisms. This infection leads to complications including multiple organ failure and death. Due to the aggressive nature of this condition, early diagnosis is crucial. Treatment involves extensive soft tissue debridement and broad-spectrum antibiotics. Despite appropriate therapy, mortality is high. This case report aimed to present nursing approaches towards an elderly male patient referred to the urology service with a diagnosis of Fournier’s gangrene. Key words: Case report; Fournier’s gangrene; nursing diagnosis; patient care. INTRODUCTION Rarely observed in the peritoneum, genital and perianal re- perineal and genital regions, it is observed in a majority of gions, necrotizing fasciitis is named as Fournier’s gangrene.[1-5] cases with general symptoms, such as fever related infection It is an important disease, following an extremely insidious and weakness, and without symptoms in the perineal region, beginning and causing necrosis of the scrotum and penis by negatively influencing the prognosis by causing a delay in diag- advancing rapidly within one-two days.[1] The rate of mortal- nosis and treatment.[2,3] Consequently, anamnesis and physical ity in the literature is between 4 and 75%[6] and it has been examination are extremely important. -

Arthroscopic Versus Open Debridement of Penetrating Knee Joint Injuries
ARTHROSCOPIC VERSUS OPEN DEBRIDEMENT OF PENETRATING KNEE JOINT INJURIES John R. Raskind, M.D.* Richard A. Marder, M.D. ABSTRACT included in this study. The group treated with arthroscopic Arthroscopic debridement of penetrating knee joint debridement consisted of seven motor vehicle "dash- injuries has become a common treatment method. A board" injuries, five motorcycle/moped/bicycle injuries and comparative study was undertaken to compare this two low velocity gun shot wounds. The mean wound size method with open joint debridement. Fourteen penetrat- in this group was 3.8 centimeters (cms) (range one to ing knee joint injuries (fourteen patients) were treated by twelve cms) and the mean patient age was 26.6 (range arthroscopic examination and debridement and were com- nine to fifty-twelve years). The open debridement group pared to sixteen penetrating knee joint injuries (fifteen consisted of eight motor vehicle "dashboard" injuries, five patients) treated by open debridement. There were no motorcycle/moped injuries, one low velocity gunshot resultant infections or operative complications in either wound, one weed-trimmer laceration, and one power-saw group. Of note, the arthroscopic debridement group had a laceration. The mean wound size in this group was 4.6 cms shorter postoperative hospital stay [mean of 1.6 days (range one to twelve cms) and the mean patient age was compared to a mean of 2.6 days in the open debridement 26.9 years (range fifteen to forty-three years). group (p < 0.02)], a significant incidence of additional Diagnosis was based upon examination of the wound, intra-articular injuries detected (p < 0.01), less postoper- AP, lateral, and notch radiographic views of the knee, and ative pain, and a superior cosmetic result. -

The Role of Pressure Ulcers in the Fight Against Antimicrobial Resistance
The role of pressure ulcer prevention in the fight against antimicrobial resistance Every year over 25,000 patients die in the EU alone as a result of infections caused by antibiotic- resistant bacteria. Globally the number of deaths due to antimicrobial resistance (AMR) was estimated to be 700,0001 in 2014 and that number has been calculated to rise to at least 10 million by 2050. The continuing emergence of AMR has become a recurring topic in the international health agenda as the increasingly serious threat to cross-border public health is recognised. From WHO to OECD, international bodies are constantly monitoring, reporting and formulating strategies to contain AMR. AMR is defined by WHO as the ability of microorganisms to survive antimicrobial treatments; consequently, prophylactic and therapeutic regimens are ineffective in controlling infections caused by resistant bacteria, fungi, parasites and viruses.2 The situation has deteriorated dramatically in the past decade with AMR reaching levels of 80% in some countries.3 How has this happened? Whereas greater investment and skill in reporting of AMR may be one reason, an important consideration is that AMR is a natural and inevitable process which is aggravated by the inappropriate use of antimicrobial agents. Healthcare authorities have been aware of the consequences of overuse of antibiotics in animal and human health, yet relatively few actions have been implemented to slow the process down.4 The good news is that the EU has made a significant step forward to gain a global lead in the fight against AMR. In June 2017 the Commission adopted the ambitious EU One Health Action Plan against AMR5 (as requested by the Member States in the Council Conclusions of 17 June 2016). -

Test Your CPT Coding Knowledge for Penetrating Trauma
CODING AND PRACTICE MANAGEMENT CORNER Test your CPT coding knowledge for penetrating trauma by Jayme Lieberman, MD, FACS; Christopher Senkowski, MD, FACS; Charles Mabry, MD, FACS; and Jan Nagle, MS revious Bulletin articles thigh level. The emergency of all wounds, the tourniquet have provided Current medical service providers had is let down and hemostasis is PProcedural Terminology applied a tourniquet in the field, obtained. A 100 sq cm negative (CPT)* coding guidance for reducing the bleeding from the pressure dressing is placed on trauma cases, including: “Coding stump of the leg. The surgeon the amputated leg stump. At the for damage-control surgery”† and arrives at the ED and performs end of the operation, the patient “Effectively using E/M codes for the primary and secondary is maintained on a ventilator trauma care.”‡ This article presents Advanced Trauma Life Support® with ongoing resuscitation and is several clinical scenarios involving (ATLS®) surveys, an abdominal transferred to the intensive care penetrating trauma and challenges and retroperitoneal focused unit (ICU). (See Table 2, page 47.) 46 | the reader’s coding knowledge assessment with sonography for for each example provided. trauma (FAST) exam, and exams Postoperative work in the ICU of the patient’s leg. The surgeon Later the same day in ICU, the orders administration of blood, surgeon examines the patient Trauma Scenario 1 antibiotics, and fluids based on and orders a blood transfusion, the examination, vital signs, and adjusts intravenous (IV) fluids Initial work in ED available labs. It is determined that to stabilize electrolytes/ A 25-year-old male involved in the partially severed leg, which coagulopathy, titrates the an accident related to a tractor’s was mangled by the tractor, is ventilator settings, and orders power take-off mechanism arrives unsalvageable. -

Clinical Case of the Month Pressure Ulcer Treatment
Spinal Cord (1997) 35, 641 ± 646 1997 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/97 $12.00 Clinical Case of the Month Pressure ulcer treatment F Biering-Sùrensen1, JL Sùrensen2, TEP Barros3, AA Monteiro3, I Nuseibeh4, SM Shenaq5 and K Shibasaki6 1Centre for Spinal Cord Injured, the Neuroscience Centre, and 2Department of Plastic Surgery, Rigshospitalet, Copenhagen University Hospital, Denmark; 3Spinal Injury Unit, Department of Orthopaedics, University of Sao Paulo, Brazil; 4National Spinal Injuries Centre, Stoke Mandeville, England; 5Department of Surgery, Baylor College of Medicine, The Methodist Hospital, Houston, Texas, USA; 6Spinal Cord Division, Department of Orthopedic Surgery, National Murayama Hospital, Japan Keywords: spinal cord injury; paraplegia; pressure ulcer; management; treatment; surgery Introduction The complicated case story below was presented to and found. Over the sacrum there was an ulcer measuring discussed by senior colleagues from Brazil, England, 2.561.5 cm with bone at the base. The plastic surgeon Japan and USA. None of the the responders knew that concluded, not least because of the patient's mental the patient had sustained his injury in 1981, and the habitus, not to operate, but to try conservative initial report stopped at the New Year 1986/87. A treatment. X-ray gave no indication of osteitis. Three review of the patient's medical history for the following weeks later the left trochanteric ulcer measured 3.5 cm years up to date is presented. Finally a short discussion in diameter and 3.5 cm in depth with necrosis and an of the possibilities of treatment is given. iliotibial tract at the base.