Some Variations in the Formation of the Brachial Plexus in Infants*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomical Study of the Brachial Plexus in Human Fetuses and Its Relation with Neonatal Upper Limb Paralysis
ORIGINAL ARTICLE Anatomical study of the brachial plexus Official Publication of the Instituto Israelita de Ensino e Pesquisa Albert Einstein in human fetuses and its relation with neonatal upper limb paralysis ISSN: 1679-4508 | e-ISSN: 2317-6385 Estudo anatômico do plexo braquial de fetos humanos e sua relação com paralisias neonatais do membro superior Marcelo Rodrigues da Cunha1, Amanda Aparecida Magnusson Dias1, Jacqueline Mendes de Brito2, Cristiane da Silva Cruz1, Samantha Ketelyn Silva1 1 Faculdade de Medicina de Jundiaí, Jundiaí, SP, Brazil. 2 Centro Universitário Padre Anchieta, Jundiaí, SP, Brazil. DOI: 10.31744/einstein_journal/2020AO5051 ❚ ABSTRACT Objective: To study the anatomy of the brachial plexus in fetuses and to evaluate differences in morphology during evolution, or to find anatomical situations that can be identified as the cause of obstetric paralysis. Methods: Nine fetuses (12 to 30 weeks of gestation) stored in formalin were used. The supraclavicular and infraclavicular parts of the brachial plexus were dissected. Results: In its early course, the brachial plexus had a cord-like shape when it passed through the scalene hiatus. Origin of the phrenic nerve in the brachial plexus was observed in only one fetus. In the deep infraclavicular and retropectoralis minor spaces, the nerve fibers of the brachial plexus were distributed in the axilla and medial bicipital groove, where they formed the nerve endings. Conclusion: The brachial plexus of human fetuses presents variations and relations with anatomical structures that must be considered during clinical and surgical procedures for neonatal paralysis of the upper limbs. How to cite this article: Cunha MR, Dias AA, Brito JM, Cruz CS, Silva Keywords: Brachial plexus/anatomy & histology; Fetus/abnormalities; Paralysis SK. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -

High-Resolution 3T MR Neurography of the Brachial Plexus and Its Branches, with Emphasis on 3D Imaging
REVIEW ARTICLE High-Resolution 3T MR Neurography of the Brachial Plexus and Its Branches, with Emphasis on 3D Imaging A. Chhabra, G.K. Thawait, T. Soldatos, R.S. Thakkar, F. Del Grande, M. Chalian, and J.A. Carrino ABSTRACT SUMMARY: With advancement in 3D imaging, better fat-suppression techniques, and superior coil designs for MR imaging and the increasing availability and use of 3T magnets, the visualization of the complexity of the brachial plexus has become facile. The relevant imaging findings are described for normal and pathologic conditions of the brachial plexus. These radiologic findings are supported by clinical and/or EMG/surgical data, and corresponding high-resolution MR neurography images are illustrated. Because the brachial plexus can be affected by a plethora of pathologies, resulting in often serious and disabling complications, a better radiologic insight has great potential in aiding physicians in rendering superior services to patients. ABBREVIATIONS: EMG ϭ electromyography; MIP ϭ maximum intensity projection; MRN ϭ MR neurography; SPACE ϭ sampling perfection with application- optimized contrasts by using different flip angle; STIR ϭ short tau inversion recovery, TOS ϭ thoracic outlet syndrome he brachial plexus is a network of nerve confluences and ram- nerve (C5-C7) to the serratus anterior muscle arise directly from Tifications, which combine to form the large terminal branches the nerve roots.1,2,5 that supply motor and sensory branches to the upper extremities. The clinical differentiation of brachial plexopathy from other Trunks and Their Anatomic Relations spine-related abnormalities often poses a considerable diagnostic The C5 and C6 nerve roots compose the upper trunk, C7 contin- challenge, and electrodiagnostic tests are difficult to perform due ues as the middle trunk, and C8 and T1 compose the lower trunk. -

Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies
Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies Zachary Simmons, MD* KEYWORDS Brachial plexus Brachial plexopathy Axillary nerve Musculocutaneous nerve Suprascapular nerve Nerve conduction studies Electromyography KEY POINTS The brachial plexus provides all motor and sensory innervation of the upper extremity. The plexus is usually derived from the C5 through T1 anterior primary rami, which divide in various ways to form the upper, middle, and lower trunks; the lateral, posterior, and medial cords; and multiple terminal branches. Traction is the most common cause of brachial plexopathy, although compression, lacer- ations, ischemia, neoplasms, radiation, thoracic outlet syndrome, and neuralgic amyotro- phy may all produce brachial plexus lesions. Upper extremity mononeuropathies affecting the musculocutaneous, axillary, and supra- scapular motor nerves and the medial and lateral antebrachial cutaneous sensory nerves often occur in the context of more widespread brachial plexus damage, often from trauma or neuralgic amyotrophy but may occur in isolation. Extensive electrodiagnostic testing often is needed to properly localize lesions of the brachial plexus, frequently requiring testing of sensory nerves, which are not commonly used in the assessment of other types of lesions. INTRODUCTION Few anatomic structures are as daunting to medical students, residents, and prac- ticing physicians as the brachial plexus. Yet, detailed understanding of brachial plexus anatomy is central to electrodiagnosis because of the plexus’ role in supplying all motor and sensory innervation of the upper extremity and shoulder girdle. There also are several proximal upper extremity nerves, derived from the brachial plexus, Conflicts of Interest: None. Neuromuscular Program and ALS Center, Penn State Hershey Medical Center, Penn State College of Medicine, PA, USA * Department of Neurology, Penn State Hershey Medical Center, EC 037 30 Hope Drive, PO Box 859, Hershey, PA 17033. -
Brachial Plexus Injury
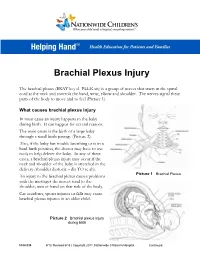
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

5. Upper Extremity Neuroanatomy
5. UPPER EXTREMITY compartments of the NEUROANATOMY arm). The brachial plexus divisions INTRODUCTION pass posterior to the mid-point of Regional anesthesia of the upper extremity in- the clavicle through volves two major nerve plexuses, the cervical plexus the cervico-axillary and the brachial plexus. A detailed understanding of canal. the anatomy of these nerve plexuses and surrounding • Three cords. The structures is essential for the safe and successful prac- divisions coalesce tice of regional anesthesia in this area of the body. to form three cords. The anterior CERVICAL PLEXUS divisions of the superior and middle The cervical plexus is formed from a series of nerve trunk form the loops between adjacent anterior rami of cervical nerve lateral cord. The roots C1 through C4. The cervical plexus is deep to the anterior division of sternocleidomastoid muscle and medial to the scalene the inferior trunk muscles. The deep branches of the plexus are motor becomes the medial nerves. They include the phrenic nerve (diaphragm cord. The posterior muscle) and the ansa cervicalis nerve (omohyoid, divisions of all sternothyroid, and sternohyoid muscles). The named three trunks unite nerves of the superficial cervical plexus are branches to form the posterior from the loops and emerge from the middle of the ster- Figure 5-1. Dissection of the superficial cervical plexus in the posterior triangle cord. The cords are nocleidomastoid muscle (Figure 5-1): BRACHIAL PLEXUS named based on their relationship to the axillary artery (as this • Lesser occipital nerve (C2): innervates the skin The brachial plexus is formed from the five roots neurovascular bundle passes in its sheath into posterior to the ear. -

Study of Variations in the Origin and Distance of Origin of Axillary Nerve Ijcrr of the Posterior Cord of Brachial Plexus
Original Article STUDY OF VARIATIONS IN THE ORIGIN AND DISTANCE OF ORIGIN OF AXILLARY NERVE IJCRR OF THE POSTERIOR CORD OF BRACHIAL PLEXUS Santosh M. Bhosale, Nagaraj S. Mallashetty Assistant Professor, Department of Anatomy, S.S.I.M.S & R.C, Davangere-577004, Karnataka, India. ABSTRACT Background: Variations in the origin of axillary nerve from the posterior cord of brachial plexus and its distance of origin from mid clavicular point are important during surgical approaches to the axilla and upper arm, administration of anesthetic blocks, interpreting effects of nervous compressions and in repair of plexus injuries. The patterns of branching show population differ- ences. Data from the South indian population is scarce. Objective: To describe the variations in the origin of the axillary nerve from the posterior cord of brachial plexus and its distance of origin from mid- clavicular point in the South Indian population. Materials and methods: Forty brachial plexuses from twenty formalin fixed cadavers were explored by gross dissection. Origin and order of branching of axillary nerve and its distance of origin from mid- clavicualr point was recorded. Representative pho- tographs were then taken using a digital camera (Sony Cybershot R, W200, 7.2 Megapixels). Results: In forty specimens studied, 87.5% of axillary nerve originated from the posterior cord of brachial plexus and in 12.5% of specimens axillary nerve took origin from common trunk along with thoracodorsal or lower subscapular nerve or both. In 32.5% of the specimens axillary nerve had origin from posterior cord of brachial plexus at a distance of 4.6-5.0cm from mid-clavicular point. -

A Review of Brachial Plexus Birth Palsy: Injury and Rehabilitation
PEDIATRIC REHABILITATION MEDICINE (PRM) A Review of Brachial Plexus Birth Palsy: Injury and Rehabilitation JEREMY E. RADUCHA, MD; BRIAN COHEN, MD; TRAVIS BLOOD, MD; JULIA KATARINCIC, MD ABSTRACT ANATOMY Brachial plexus injuries during the birthing process can The brachial plexus is derived from the fifth cervical (C5) to leave infants with upper extremity deficits corresponding the first thoracic (T1) nerve roots. It undergoes a complex to the location of the lesion within the complex plexus pattern of branching and convergence before terminating as anatomy. Manifestations can range from mild injuries with peripheral nerves that provide motor and sensory innervation complete resolution to severe and permanent disability. to the upper extremity. (Figure 1, Table 1) The plexus can be Overall, patients have a high rate of spontaneous recovery divided into supraclavicular (roots and trunks) and sub-cla- (66–92%).1,2 Initially, all lesions are managed with passive vicular (cords and terminal branches) for prognostic pur- range motion and observation. Prevention and/or correc- poses, with supraclavicular injuries having worse outcomes.9 tion of contractures with occupational therapy and serial splinting/casting along Figure 1. Brachial Plexus Anatomy with encouraging normal development are the main goals of non-operative treat- ment. Surgical intervention may be war- ranted, depending on functional recovery. KEYWORDS: Brachial plexus, Erb’s palsy, Klumpke’s palsy, serial splinting INTRODUCTION Brachial plexus birth palsy (BPBP) involves injury -

Download the Brachial Plexus Center Brochure
BRACHIAL PLEXUS CENTER DEPARTMENT OF NEUROSURGERY, NEUROLOGY, AND ORTHOPEDIC SURGERY ESTABLISHED IN 1991 EXPERTISE OF THE ST. LOUIS CHILDREN’S BRACHIAL PLEXUS CENTER HOSPITAL • 390 beds • 3,330 employees • 818 medical staff members • 1,300 auxiliary members and volunteers • More than 45 pediatric subspecialty departments and divisions • Level I Pediatric Trauma Center, the highest level of emergency care available Founded in 1879, St. Louis Children’s Left to Right: Tae Sung Park, MD, Nicole Meyer, PA-C, Lindley Wall, MD, Michael Noetzel, MD Hospital is one of the premier • Recognized as one of the best children’s children’s hospitals in the nation. It hospitals in the nation serves not just the children of St. Established in 1991, the Brachial Plexus Center has extensive by U.S. News & Louis, but children across the world. experience in the treatment of birth brachial plexus injury. World Report As the pediatric teaching hospital Our Center has cared for over 1,000 infants with brachial plexus for Washington University School of injury and performed brachial plexus repair procedures on over • Received the nation’s 250 infants. highest honor for Medicine, St. Louis nursing excellence, Children’s Hospital The Center’s team consists of pediatric neurosurgeons, neurologist, the Magnet designation, offers nationally orthopedic surgeon, occupational and physical therapists, from the American recognized neuroradiologist, and clinical coordinator. Nurses Credentialing programs for At the Brachial Plexus Center at St. Louis Children’s Hospital, Center. physician training parents find hope and unparalleled pediatric expertise. and research. 1 2 The Brachial Plexus THE CAUSE OF BIRTH BRACHIAL PLEXUS PALSY The brachial plexus is a complex arrangement of nerves that controls Diagram 3: Shoulder Dystocia the muscles of the shoulder, arms and hands. -

Shoulder and Scapular Rehabilitation for Adult Brachial Plexus Injuries
Shoulder and Scapular Rehabilitation for Adult Brachial Plexus Injuries Lynnette Rasmussen, OTRL Brachial Plexus and Peripheral Nerve Program I have no financial relationships relevant to this presentation. Objectives • Participants will be provided with a brief overview of the anatomy of the brachial plexus. • Participants will understand the difference between nerve graft and nerve transfers and how it relates to rehabilitation techniques. • Participants will learn activation techniques for 3 common brachial plexus reconstructions. • Participants will understand the progression of exercises. Outline Surgical Interventions Formulating a Treatment Plan • Brief anatomy Review • What you need to know • Surgical Procedures from the Surgeon • Healing Process • Restrictions • Timing for Interventions • Activation Techniques • Therapy Progressions • Managing Patient Expectations The Brachial Plexus The Muscles Robert Taylor Drinks Cold Beer Two Main Surgical Procedures Nerve Grafts Nerve Transfer Science of Healing • Nerve repair= 3-6 weeks to regain enough strength to tolerate mobilization • Tendon Transfers= 6 weeks to heal • Axonal regeneration= “1 mm per day” or 1” per month”. Prior to Surgery • Full assessment • Focus on joint protection • Range of Motion • No e-stim • Gravity eliminated exercises • Strengthen uninvolved muscles Formulating Your Treatment Plan Following Surgery • How long to immobilize • Protective orthosis? • Starting PROM • Movement Restrictions • Expectations • Donor used will dictate activation process Get the Scoop -

Variations in Subscapularis Muscle Innervation—A Report on Case Series
medicina Article Variations in Subscapularis Muscle Innervation—A Report on Case Series Martin Siwetz 1, Niels Hammer 1,2,3,*, Benjamin Ondruschka 4 and David C. Kieser 5 1 Department of Macroscopic and Clinical Anatomy, Medical University of Graz, 8010 Graz, Austria; [email protected] 2 Fraunhofer IWU, Medical Branch, 01187 Dresden, Germany 3 Department of Orthopedic and Trauma Surgery, University of Leipzig, 04109 Leipzig, Germany 4 Institute of Legal Medicine, University Medical Center Hamburg-Eppendorf, 22529 Hamburg, Germany; [email protected] 5 Department of Orthopaedic Surgery and Musculoskeletal Medicine, University of Otago, 8140 Christchurch, New Zealand; [email protected] * Correspondence: [email protected] or [email protected]; Tel.: +43-316-385-71100 Received: 31 August 2020; Accepted: 10 October 2020; Published: 12 October 2020 Abstract: Background and objectives: The subscapularis muscle is typically innervated by two distinct nerve branches, namely the upper and lower subscapular nerve. These usually originate from the posterior cord of the brachial plexus. A large number of variations have been described in previous literature. Materials and Methods: Dissection was carried out in 31 cadaveric specimens. The frequency of accessory subscapular nerves was assessed and the distance from the insertion points of these nerves to the myotendinous junction was measured. Results: Accessory subscapular nerves were found in three cases (9.7%). According to their origin from the posterior cord of the brachial plexus proximal to the thoracodorsal nerve all three nerves were identified as accessory upper subscapular nerves. No accessory lower subscapular nerves were found. Conclusion: Accessory nerves occur rather commonly and need to be considered during surgery, nerve blocks, and imaging procedures. -

Brachial Plexus Injury
Brachial Plexus Injury What is the brachial plexus? The brachial plexus is a network of nerves that originate near the neck Figure 1: The brachial plexus is a network of nerves that originate near the neck and shoulder, whose branches form the and shoulder. These nerves begin at the spinal cord in the neck and nerves that go into the arm, forearm, and hand. control the hand, wrist, elbow, and shoulder (see Figure 1). Nerves are the electrical wiring system in all people that carry messages from the brain to the rest of the body. A nerve is like an electrical cable wrapped in insulation. nerves artery Motor nerves carry messages from the brain to muscles to make the body move. Sensory nerves carry messages to the brain from different parts of the body to signal pain, pressure, and temperature. The brachial plexus has nerves that are both motor and sensory. What happens when the brachial plexus is injured? The network of nerves is fragile and can be damaged by pressure, stretching, or cutting. Stretching can occur when the head and neck are forced away from the shoulder, such as might happen in a fall off a scapula motorcycle. If severe enough, the nerves can actually avulse, or tear out of, their roots in the neck. Pressure could occur from crushing of the brachial plexus between the collarbone and first rib, or swelling in this area from injured muscles or other structures. brachial artery Injury to a nerve can stop signals to and from the brain, preventing the muscles of the arm and hand from working properly, and causing loss of feeling in the area supplied by the injured nerve.