37. Lumbar Plexus. Sacral Plexus. Coccygeal Plexus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinical Presentations of Lumbar Disc Degeneration and Lumbosacral Nerve Lesions
Hindawi International Journal of Rheumatology Volume 2020, Article ID 2919625, 13 pages https://doi.org/10.1155/2020/2919625 Review Article Clinical Presentations of Lumbar Disc Degeneration and Lumbosacral Nerve Lesions Worku Abie Liyew Biomedical Science Department, School of Medicine, Debre Markos University, Debre Markos, Ethiopia Correspondence should be addressed to Worku Abie Liyew; [email protected] Received 25 April 2020; Revised 26 June 2020; Accepted 13 July 2020; Published 29 August 2020 Academic Editor: Bruce M. Rothschild Copyright © 2020 Worku Abie Liyew. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Lumbar disc degeneration is defined as the wear and tear of lumbar intervertebral disc, and it is mainly occurring at L3-L4 and L4-S1 vertebrae. Lumbar disc degeneration may lead to disc bulging, osteophytes, loss of disc space, and compression and irritation of the adjacent nerve root. Clinical presentations associated with lumbar disc degeneration and lumbosacral nerve lesion are discogenic pain, radical pain, muscular weakness, and cutaneous. Discogenic pain is usually felt in the lumbar region, or sometimes, it may feel in the buttocks, down to the upper thighs, and it is typically presented with sudden forced flexion and/or rotational moment. Radical pain, muscular weakness, and sensory defects associated with lumbosacral nerve lesions are distributed on -

4-Brachial Plexus and Lumbosacral Plexus (Edited).Pdf
Color Code Brachial Plexus and Lumbosacral Important Doctors Notes Plexus Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of this lecture, the students should be able to : Describe the formation of brachial plexus (site, roots) List the main branches of brachial plexus Describe the formation of lumbosacral plexus (site, roots) List the main branches of lumbosacral plexus Describe the important Applied Anatomy related to the brachial & lumbosacral plexuses. Brachial Plexus Formation Playlist o It is formed in the posterior triangle of the neck. o It is the union of the anterior rami (or ventral) of the 5th ,6th ,7th ,8th cervical and the 1st thoracic spinal nerves. o The plexus is divided into 5 stages: • Roots • Trunks • Divisions • Cords • Terminal branches Really Tired? Drink Coffee! Brachial Plexus A P A P P A Brachial Plexus Trunks Divisions Cords o Upper (superior) trunk o o Union of the roots of Each trunk divides into Posterior cord: C5 & C6 anterior and posterior From the 3 posterior division divisions of the 3 trunks o o Middle trunk Lateral cord: From the anterior Continuation of the divisions of the upper root of C7 Branches and middle trunks o All three cords will give o Medial cord: o Lower (inferior) trunk branches in the axilla, It is the continuation of Union of the roots of the anterior division of C8 & T1 those will supply their respective regions. the lower trunk The Brachial Plexus Long Thoracic (C5,6,7) Anterior divisions Nerve to Subclavius(C5,6) Posterior divisions Dorsal Scapular(C5) Suprascapular(C5,6) upper C5 trunk Lateral Cord C6 middle (2LM) trunk C7 lower C8 trunk T1 Posterior Cord (ULTRA) Medial Cord (4MU) In the PowerPoint presentation this slide is animated. -

LECTURE (SACRAL PLEXUS, SCIATIC NERVE and FEMORAL NERVE) Done By: Manar Al-Eid Reviewed By: Abdullah Alanazi
CNS-432 LECTURE (SACRAL PLEXUS, SCIATIC NERVE AND FEMORAL NERVE) Done by: Manar Al-Eid Reviewed by: Abdullah Alanazi If there is any mistake please feel free to contact us: [email protected] Both - Black Male Notes - BLUE Female Notes - GREEN Explanation and additional notes - ORANGE Very Important note - Red CNS-432 Objectives: By the end of the lecture, students should be able to: . Describe the formation of sacral plexus (site & root value). List the main branches of sacral plexus. Describe the course of the femoral & the sciatic nerves . List the motor and sensory distribution of femoral & sciatic nerves. Describe the effects of lesion of the femoral & the sciatic nerves (motor & sensory). CNS-432 The Mind Maps Lumber Plexus 1 Branches Iliohypogastric - obturator ilioinguinal Femoral Cutaneous branches Muscular branches to abdomen and lower limb 2 Sacral Plexus Branches Pudendal nerve. Pelvic Splanchnic Sciatic nerve (largest nerves nerve), divides into: Tibial and divides Fibular and divides into : into: Medial and lateral Deep peroneal Superficial planter nerves . peroneal CNS-432 Remember !! gastrocnemius Planter flexion – knee flexion. soleus Planter flexion Iliacus –sartorius- pectineus – Hip flexion psoas major Quadriceps femoris Knee extension Hamstring muscles Knee flexion and hip extension gracilis Hip flexion and aids in knee flexion *popliteal fossa structures (superficial to deep): 1-tibial nerve 2-popliteal vein 3-popliteal artery. *foot drop : planter flexed position Common peroneal nerve injury leads to Equinovarus Tibial nerve injury leads to Calcaneovalgus CNS-432 Lumbar Plexus Formation Ventral (anterior) rami of the upper 4 lumbar spinal nerves (L1,2,3 and L4). Site Within the substance of the psoas major muscle. -

Study of Anatomical Pattern of Lumbar Plexus in Human (Cadaveric Study)
54 Az. J. Pharm Sci. Vol. 54, September, 2016. STUDY OF ANATOMICAL PATTERN OF LUMBAR PLEXUS IN HUMAN (CADAVERIC STUDY) BY Prof. Gamal S Desouki, prof. Maged S Alansary,dr Ahmed K Elbana and Mohammad H Mandor FROM Professor Anatomy and Embryology Faculty of Medicine - Al-Azhar University professor of anesthesia Faculty of Medicine - Al-Azhar University Anatomy and Embryology Faculty of Medicine - Al-Azhar University Department of Anatomy and Embryology Faculty of Medicine of Al-Azhar University, Cairo Abstract The lumbar plexus is situated within the substance of the posterior part of psoas major muscle. It is formed by the ventral rami of the frist three nerves and greater part of the fourth lumbar nerve with or without a contribution from the ventral ramus of last thoracic nerve. The pattern of formation of lumbar plexus is altered if the plexus is prefixed (if the third lumbar is the lowest nerve which enters the lumbar plexus) or postfixed (if there is contribution from the 5th lumbar nerve). The branches of the lumbar plexus may be injured during lumbar plexus block and certain surgical procedures, particularly in the lower abdominal region (appendectomy, inguinal hernia repair, iliac crest bone graft harvesting and gynecologic procedures through transverse incisions). Thus, a better knowledge of the regional anatomy and its variations is essential for preventing the lesions of the branches of the lumbar plexus. Key Words: Anatomical variations, Lumbar plexus. Introduction The lumbar plexus formed by the ventral rami of the upper three nerves and most of the fourth lumbar nerve with or without a contribution from the ventral ramous of last thoracic nerve. -

Lower Extremity Focal Neuropathies
LOWER EXTREMITY FOCAL NEUROPATHIES Lower Extremity Focal Neuropathies Arturo A. Leis, MD S.H. Subramony, MD Vettaikorumakankav Vedanarayanan, MD, MBBS Mark A. Ross, MD AANEM 59th Annual Meeting Orlando, Florida Copyright © September 2012 American Association of Neuromuscular & Electrodiagnostic Medicine 2621 Superior Drive NW Rochester, MN 55901 Printed by Johnson Printing Company, Inc. 1 Please be aware that some of the medical devices or pharmaceuticals discussed in this handout may not be cleared by the FDA or cleared by the FDA for the specific use described by the authors and are “off-label” (i.e., a use not described on the product’s label). “Off-label” devices or pharmaceuticals may be used if, in the judgment of the treating physician, such use is medically indicated to treat a patient’s condition. Information regarding the FDA clearance status of a particular device or pharmaceutical may be obtained by reading the product’s package labeling, by contacting a sales representative or legal counsel of the manufacturer of the device or pharmaceutical, or by contacting the FDA at 1-800-638-2041. 2 LOWER EXTREMITY FOCAL NEUROPATHIES Lower Extremity Focal Neuropathies Table of Contents Course Committees & Course Objectives 4 Faculty 5 Basic and Special Nerve Conduction Studies of the Lower Limbs 7 Arturo A. Leis, MD Common Peroneal Neuropathy and Foot Drop 19 S.H. Subramony, MD Mononeuropathies Affecting Tibial Nerve and its Branches 23 Vettaikorumakankav Vedanarayanan, MD, MBBS Femoral, Obturator, and Lateral Femoral Cutaneous Neuropathies 27 Mark A. Ross, MD CME Questions 33 No one involved in the planning of this CME activity had any relevant financial relationships to disclose. -

New Insights in Lumbosacral Plexopathy
New Insights in Lumbosacral Plexopathy Kerry H. Levin, MD Gérard Said, MD, FRCP P. James B. Dyck, MD Suraj A. Muley, MD Kurt A. Jaeckle, MD 2006 COURSE C AANEM 53rd Annual Meeting Washington, DC Copyright © October 2006 American Association of Neuromuscular & Electrodiagnostic Medicine 2621 Superior Drive NW Rochester, MN 55901 PRINTED BY JOHNSON PRINTING COMPANY, INC. C-ii New Insights in Lumbosacral Plexopathy Faculty Kerry H. Levin, MD P. James. B. Dyck, MD Vice-Chairman Associate Professor Department of Neurology Department of Neurology Head Mayo Clinic Section of Neuromuscular Disease/Electromyography Rochester, Minnesota Cleveland Clinic Dr. Dyck received his medical degree from the University of Minnesota Cleveland, Ohio School of Medicine, performed an internship at Virginia Mason Hospital Dr. Levin received his bachelor of arts degree and his medical degree from in Seattle, Washington, and a residency at Barnes Hospital and Washington Johns Hopkins University in Baltimore, Maryland. He then performed University in Saint Louis, Missouri. He then performed fellowships at a residency in internal medicine at the University of Chicago Hospitals, the Mayo Clinic in peripheral nerve and electromyography. He is cur- where he later became the chief resident in neurology. He is currently Vice- rently Associate Professor of Neurology at the Mayo Clinic. Dr. Dyck is chairman of the Department of Neurology and Head of the Section of a member of several professional societies, including the AANEM, the Neuromuscular Disease/Electromyography at Cleveland Clinic. Dr. Levin American Academy of Neurology, the Peripheral Nerve Society, and the is also a professor of medicine at the Cleveland Clinic College of Medicine American Neurological Association. -

35. Lumbar Plexus. Sacral Plexus. Coccygeal Plexus
GUIDELINES Students’ independent work during preparation to practical lesson Academic discipline HUMAN ANATOMY Topic LUMBAR PLEXUS. SACRAL PLEXUS. COCCYGEAL PLEXUS 1. Relevance of the topic Lumbar, sacral and coccygeal plexuses innervate the skin of the abdomen, lower back and lower extremities and all the muscles of the lower limbs. Acquired knowledge is the basis for many fields of practical medicine, such as neurology, surgery and traumatology. 2. Specific objectives After the lesson the student should know and be able to: - describe the sources of the formation of the lumbar plexus; - classify the nerves of the lumbar plexus; - to be able to demonstrate and define the branches of the lumbar plexus; - describe sources of sacral plexus formation; - classify sacral plexus nerves; - be able to demonstrate and identify short and long branches of the sacral plexus; - describe the sources of formation coccygeal plexus; - classify coccygeal plexus nerves; - be able to demonstrate and identify branches of coccygeal plexus; - to explain the innervation of muscles and skin in the areas of the lower back and lower extremity. 3. Basic level of preparation For practical this lesson a student should know and be able: - to know the anatomy of the spine, pelvis, lower extremities; - to analyze and show large and small pelvis, their bones; - to analyze and demonstrate bones and joints of the lower limbs; - to demonstrate muscles of the abdomen, perineum, pelvic girdle and lower limbs; - to know the anatomy (external and internal structure) of the spinal cord; - to know the spinal nerve anatomy. 4. Tasks for independent work during preparation for the classes 4.1. -

ANATOMICAL VARIATIONS and DISTRIBUTIONS of OBTURATOR NERVE on ETHIOPIAN CADAVERS Berhanu KA, Taye M, Abraha M, Girma A
https://dx.doi.org/10.4314/aja.v9i1.1 ORIGINAL COMMUNICATION Anatomy Journal of Africa. 2020. Vol 9 (1): 1671 - 1677. ANATOMICAL VARIATIONS AND DISTRIBUTIONS OF OBTURATOR NERVE ON ETHIOPIAN CADAVERS Berhanu KA, Taye M, Abraha M, Girma A Correspondence to Berhanu Kindu Ashagrie Email: [email protected]; Tele: +251966751721; PO Box: 272 Debre Tabor University , North Central Ethiopia ABSTRACT Variations in anatomy of the obturator nerve are important to surgeons and anesthesiologists performing surgical procedures in the pelvic cavity, medial thigh and groin regions. They are also helpful for radiologists who interpret computerized imaging and anesthesiologists who perform local anesthesia. This study aimed to describe the anatomical variations and distribution of obturator nerve. The cadavers were examined bilaterally for origin to its final distribution and the variations and normal features of obturator nerve. Sixty-seven limbs sides (34 right and 33 left sides) were studied for variation in origin and distribution of obturator nerve. From which 88.1% arises from L2, L3 and L4 and; 11.9% from L3 and L4 spinal nerves. In 23.9%, 44.8% and 31.3% of specimens the bifurcation levels of obturator nerve were determined to be intrapelvic, within the obturator canal and extrapelvic, respectively. The anterior branch subdivided into two, three and four subdivisions in 9%, 65.7% and 25.4% of the specimens, respectively, while the posterior branch provided two subdivisions in 65.7% and three subdivisions in 34.3% of the specimens. Hip articular branch arose from common obturator nerve in 67.2% to provide sensory innervation to the hip joint. -

The Lumbosacral Plexus: Anatomic Considerations for Minimally Invasive Retroperitoneal Transpsoas Approach
Surg Radiol Anat (2012) 34:151–157 DOI 10.1007/s00276-011-0881-z ORIGINAL ARTICLE The lumbosacral plexus: anatomic considerations for minimally invasive retroperitoneal transpsoas approach Patrick Gue´rin • Ibrahim Obeid • Anouar Bourghli • Thibault Masquefa • Ste´phane Luc • Olivier Gille • Vincent Pointillart • Jean-Marc Vital Received: 2 May 2011 / Accepted: 21 September 2011 / Published online: 5 October 2011 Ó Springer-Verlag 2011 Abstract plexus was performed. All nerve branches and sympathetic Purpose The minimally invasive transpsoas approach can chain were identified. Intervertebral disc space from L1L2 be employed to treat various spinal disorders, such as disc to L4L5 was divided into four zones. Zone 1 being the degeneration, deformity, and lateral disc herniation. With anterior quarter of the disc, zone 2 being the middle this technique, visualization is limited in comparison with anterior quarter, zone 3 the posterior middle quarter and the open procedure and the proximity of the lumbar plexus zone 4 the posterior quarter. Crossing of each nervous to the surgical pathway is one limitation of this technique. branch with the disc was reported and a safe working zone Precise knowledge of the regional anatomy of the lumbar was determined for L1L2 to L4L5 disc levels. A safe plexus is required for safe passage through the psoas working zone was defined by the absence of crossing of a muscle. The primary objective of this study was to deter- lumbar plexus branch. mine the anatomic position of the lumbar plexus branches Results No anatomical variation was found during blunt and sympathetic chain in relation to the intervertebral disc dissection. -
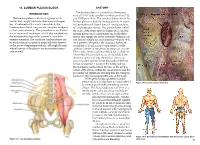
Lumbar Plexus Block Anatomy
14. LUMBAR PLEXUS BLOCK ANATOMY INTRODUCTION The lumbar plexus is formed from the ventral rami of L1–L4 with variable contributions from T12 The lumbar plexus consists of a group of six and L5 (Figure 14-1). The peripheral branches of the nerves that supply the lower abdomen and upper lumbar plexus include the iliohypogastric, ilioingui- leg. Combined with a sciatic nerve block, the nal, genitofemoral, lateral femoral cutaneous, femo- lumbar plexus block can provide complete analgesia ral, and obturator nerves. The plexus forms within to the lower extremity. This procedure is an alterna- the body of the psoas muscle (Figure 14-2), and the tive to neuraxial anesthesia, which also anesthetizes lumbar plexus block consistently blocks the three the nonoperative leg and occasionally results in nerves that supply the lower extremity (femoral, lat- urinary retention. The complete lumbar plexus can eral femoral cutaneous, and obturator—Figure 14-3). be blocked from a posterior approach (also known As it passes to the pelvis, the obturator has more as the psoas compartment block), although the indi- variability of location and is separated from the vidual nerves of the plexus can be accessed anteri- other two nerves of the plexus by the psoas muscle. orly as well. This is why the femoral nerve block (also called the “3-in-1 block”) often fails to successfully block the obturator nerve and why the lumbar plexus ap- proach is often selected when blockade of all three nerves is required. However, the lumbar plexus block remains controversial because of the deep lo- cation of the plexus within the psoas muscle and the possibility for significant bleeding into the retroperi- toneum in this noncompressible area of the body. -

Quickstudy.Comhundreds of Titles at Written Permission from the Publisher
BarCharts, Inc.® WORLD’S #1 ACADEMIC OUTLINE CERVICOBRACHIAL PLEXUS LUMBOSACRAL PLEXUS Cerebellum 1st cervical vertebrae (transverse process)** 12th thoracic vertebrae (pedicle)** Brain 1st lumbar vertebrae (pedicle)** Trace of the mandible th Supraclavicular n. 5 lumbar vertebrae (pedicle)** T11 Thoracic st n.n. Cervical C1 th 1 cervical n. plexus 7 cervicle vertebrae Sacrum, is made up of 5 fused T12 T1-T12 C2 (pedicle & transverse process)** vertebrae (pedicles)** C1-C4 C3 L1 Lumbar Cervical C4 Upper trunk 1st thoracic vertebrae Iliohypogastric n. plexus n.n. C5 (pedicle)** L2 T12-L4 C1-C8 C6 Middle trunk Ilioinguinal n. Trace of the scapula Cervical Lumbar Brachial C7 Inferior trunk Genitofemoral n. L3 plexus C8 Lateral cord plexus Brachial n.n. L4 L1-L5 C5-T1 T1 Posterior cord 8th cervical n. plexus Lateral femoral cutaneous n. Trace of the pelvis T2 Medial cord 1st thoracic n. L5 Sacral Intercostal n.n. Femoral n. T3 Humerus plexus Spinal cord Superior gluteal n. S1 T4 L5-S4 Thoracic Musculocutaneous n. Inferior gluteal n. S2 Sacral n.n. T5 Trace of the scapula S3 T1-T12 Axillary n. S4 n.n. T6 Trace of the spinal column Posterior femoral S1-S5 cutaneous n. S5 T7 Conus medullaris Musculocutaneous n. Coccygeal T8 Axillary n. n. Radial n. Sciatic n. T9 Cauda equina Pudendal n. Radial n. Median n. T10 Cutaneous n. Ulnar n. Inferior rectal n. of forearm Posterior brachial cutaneous n. Ulnar n. Femur Median n. Subcostal n. Muscular Dorsal n. of Iliohypogastric n. branches penis (clitoris) Ilioinguinal n. Deep branch Perineal n. m. = muscle Superficial branch n. -

Sacral Plexus and the Pudendal Nerve in Man by Use of Computer Aided Three-Dimensional Reconstruction
Okajimas Folia Anat. Jpn., 72(1): 29-36, May, 1995 An Anatomical Analysis of the Dorsoventral Relationship between the Sacral Plexus and the Pudendal Nerve in Man by Use of Computer Aided Three-Dimensional Reconstruction By Keiichi AKITA and Hitoshi YAMAMOTO Department of Anatomy, School of Medicine, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, Tokyo, 113, Japan -Received for Publication, January 30, 1995- Key Words: Pudendal nerve, Sacral Plexus, 3-D reconstruction, Human gross anatomy Summary: In order to investigate the dorsoventral relationship between the sacral plexus and the pudendal nerve in man, morphological examination was performed on one pelvic half of a male cadaver. The second and third spinal nerves were removed en bloc and sectioned serially for three-dimensional reconstruction imaging of the selected sections. Comparison of the sequential images revealed that the root of the pudendal nerve is first situated ventral to the caudal root of the sacral plexus, and that the former and the latter are shifted cranialward and caudalward, respectively, at the point of exit from the second anterior sacral foramen. Abbreviation (Macaw mulatta) in order to determine the detailed relationships between the innervation of the pelvic Bis nerveto the short head of the bicepsfemoris limb and the pelvic outlet muscles. These findings Br (ex. Br1) branchof the spinalnerve revealed that the origins of the pudendal nerves Cfp posteriorfemoral cutaneous nerve were situated ventrocaudal to the sacral plexus. Co nerveto the coccygeus D dorsalprimary rami The present study was undertaken to confirm the Fx femoralflexor nerve dorsoventral relationship between the sacral plexus Gi inferiorgluteal nerve and the pudendal nerve in man by using computer Gs superiorgluteal nerve aided three-dimensional reconstruction imaging of La nerveto the levatorani serial sections of the second sacral nerve.