Evaluation of Covid-19 Pandemic in Azad Jammu And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

S# BRANCH CODE BRANCH NAME CITY ADDRESS 1 24 Abbottabad
BRANCH S# BRANCH NAME CITY ADDRESS CODE 1 24 Abbottabad Abbottabad Mansera Road Abbottabad 2 312 Sarwar Mall Abbottabad Sarwar Mall, Mansehra Road Abbottabad 3 345 Jinnahabad Abbottabad PMA Link Road, Jinnahabad Abbottabad 4 131 Kamra Attock Cantonment Board Mini Plaza G. T. Road Kamra. 5 197 Attock City Branch Attock Ahmad Plaza Opposite Railway Park Pleader Lane Attock City 6 25 Bahawalpur Bahawalpur 1 - Noor Mahal Road Bahawalpur 7 261 Bahawalpur Cantt Bahawalpur Al-Mohafiz Shopping Complex, Pelican Road, Opposite CMH, Bahawalpur Cantt 8 251 Bhakkar Bhakkar Al-Qaim Plaza, Chisti Chowk, Jhang Road, Bhakkar 9 161 D.G Khan Dera Ghazi Khan Jampur Road Dera Ghazi Khan 10 69 D.I.Khan Dera Ismail Khan Kaif Gulbahar Building A. Q. Khan. Chowk Circular Road D. I. Khan 11 9 Faisalabad Main Faisalabad Mezan Executive Tower 4 Liaqat Road Faisalabad 12 50 Peoples Colony Faisalabad Peoples Colony Faisalabad 13 142 Satyana Road Faisalabad 585-I Block B People's Colony #1 Satayana Road Faisalabad 14 244 Susan Road Faisalabad Plot # 291, East Susan Road, Faisalabad 15 241 Ghari Habibullah Ghari Habibullah Kashmir Road, Ghari Habibullah, Tehsil Balakot, District Mansehra 16 12 G.T. Road Gujranwala Opposite General Bus Stand G.T. Road Gujranwala 17 172 Gujranwala Cantt Gujranwala Kent Plaza Quide-e-Azam Avenue Gujranwala Cantt. 18 123 Kharian Gujrat Raza Building Main G.T. Road Kharian 19 125 Haripur Haripur G. T. Road Shahrah-e-Hazara Haripur 20 344 Hassan abdal Hassan Abdal Near Lari Adda, Hassanabdal, District Attock 21 216 Hattar Hattar -

I. Organizational Chart
I. Organizational Chart SBP BANKING SERVICES CORPORATION Board of Directors Managing Director Aftab Mustafa Khan MD Secretariat Head Office Field Offices Personnel Management Currency Management Department Karachi Office Lahore Office Department Javaid Iqbal Taslim Kazi Dr.Muhammad Saleem Amjad Manzoor Chief Manager Chief Manager Director Director Islamabad Office Peshawar Office Foreign Exchange Operations Development Finance Support Tariq Riaz Muhammad Tanwirul Islam Department Department Chief Manager Chief Manager Syed Shahzad Safdar Zaidi Muhammad Mazharul Haq Director Director Rawalpindi Office Quetta Office Asad Shah Ali Hussain Chief Manager Chief Manager * Training & Development Department Accounts Department Amjad Manzoor Muhammad Habib Khan Director* Director Hyderabad Office Faisalabad Office Ali Hussain Sajjad Ali Shah Chief Manager Chief Manager General Services Department Internal Audit Department Zafar Iqbal Maraj Mahmood Director Head Multan Office North Nazimabad Office Javaid Iqbal Marath Ansar Iftikhar Butt Chief Manager Chief Manager Quality Assurance Department Engineering Department Feroza Nabeel Qureshi Fazli Hameed Director Head Muzaffarabad Office Sukkur Office Muhammad Tahir Malik Muhammad Ashraf Khokhar Chief Manager (A) Chief Manager Foreign Exchange Adjudication Department Internal Bank Security Muhammed Saleem Rehmani Department Brig.(R) M. Pervez Akbar Bahawalpur Office Gujranwala Office Director Khadim Hussain Aamir Nazir Bhatti Director Chief Manager (A) Chief Manager (A) * Additional Charge Sialkot Office D.I. Khan Office ( A) Acting Basis Azhar Iqbal Muhammad Humayun Khan Chief Manager Chief Manager Annual Performance Review of SBP BSC FY12 II. Board of Directors S # Name Status 1 Mr. Yaseen Anwar Governor SBP/ Chairman of SBP BSC Board 2 Mr. Abdul Wajid Rana Member/ Principal Officer, Finance Division, GoP 3 Mr. Mirza Qamar Beg Member 4 Mr. -

WMMR Pakistan
Epidemiological Week No. 49 (2-8 Dec 2006) 14 Dec 06/ Vol. 55/ DEWS 2006-49 Reporting Units...............................................................2 Total number of consultations ........................................2 DEWS Data, Epidemiological Week N0 49 2006............3 DEWS Data, Monthly Summary (Epidemiological Weeks N0 46-49) ........................................................................4 Acute Watery Diarrhoea .................................................5 Bloody Diarrhoea............................................................6 Acute Jaundice Syndrome..............................................6 Malaria ............................................................................7 Measles ..........................................................................7 Acute Respiratory Infection ............................................8 Other Reportable Diseases and Conditions ...................8 Outbreak Alert and Response ........................................9 Number of reported cases and deaths per District, AJK ......................................................................................10 Muzaffarabad in Winter Number of reported cases and deaths per District, Picture by Shahzad Alam Khan NWFP ...........................................................................11 In the past month (Epidemiological In week 49, there were 2 deaths weeks 46-49 inclusive), 143,111 health reported from acute Watery diarrhoea events under surveillance were reported One from Muzaffarabad district -

Muzaffarabad District Disaster Risk Management Plan
Muzaffarabad District Disaster Risk Management Plan i Muzaffarabad District Disaster Risk Management Plan This Plan is available from: 1. District Disaster Management Authority / Deputy Commissioner Office, Muzaffarabad Phone : 05822 920055 Fax : 05822 920056 2. State Disaster Management Authority, Muzaffarabad Block No. 10, First Floor (Left Wing), Opposite to AJK Legislative Assembly, New Civil Secretariat, Muzaffarabad Azad Kashmir. Phone No. +92-5822-921536, 921643 Fax No. +92-5822-921537 www.sdmagok.pk 3. National Disaster Management Authority Prime Minister’s Office, Islamabad. UAN #: 051-111-157-157 Tel #: +92 51 9205037 Fax #: +92 51 9205086 www.ndma.gov.pk Copyright © Disaster & Climate Resilience Improvement Project (DCRIP) Planning & Development Department, Azad Govt. of State of Jammu & Kashmir ii Muzaffarabad District Disaster Risk Management Plan This Plan has been prepared with the support from the World Bank under “Disaster & Climate Resilience Improvement Project (DCRIP)” in close consultation with State Disaster Management Authority and concerned stakeholders by the consultant firm “Solutions for Development Support” comprised of following team: 1. Sardar Muhammad Nawaz Khan, Team Lead 2. Ms. Amber Masud, Member 3. Mr. Waseem Ahmed, Member 4. Mr. Muhammad Imran Ayub, Member 5. Mr. Rafiullah Khan, Member 6. Mr. Arbab Taimur Khan, Member Solutions for Development Support House No 320, Al-Mustafa Tower, Sector F-10, Islamabad, Ph: 051-8737183, Email: [email protected] iii Muzaffarabad District Disaster Risk Management Plan -

COI QUERY Disclaimer
COI QUERY Country of Origin Pakistan Main subject Situation in Pakistan-administered Kashmir Question(s) 1. General information Historical background Population and ethnic groups Returnees in Kashmir and Punjab Religious demography 2. Political situation 3. Human rights situation General overview Ethnic conflict Sectarian conflict 4. Security situation Conflict-related violence Line of control violations Cross-border attacks Examples of cross-border violence in 2020 Armed groups Hizb-ul-Mujahideen (HM) Jaish-e Muhammad (JeM) Lashkar-e Taiba (LeT) Harakat ul-Mujahidin (HuM) Date of completion 6 October 2020 Query Code Q27-2020 Contributing EU+ COI -- units (if applicable) Disclaimer This response to a COI query has been elaborated according to the EASO COI Report Methodology and EASO Writing and Referencing Guide. The information provided in this response has been researched, evaluated and processed with utmost care within a limited time frame. All sources used are referenced. A quality review has been performed in line with the above mentioned methodology. This document does not claim to be exhaustive neither conclusive as to the merit of any particular claim to international protection. If a certain event, person or organisation is not mentioned in the report, this does not mean that the event has not taken place or that the person or organisation does not exist. Terminology used should not be regarded as indicative of a particular legal position. 1 The information in the response does not necessarily reflect the opinion of EASO and makes no political statement whatsoever. The target audience is caseworkers, COI researchers, policy makers, and decision making authorities. The answer was finalised on 6 October 2020. -
According to the Syllabus of University of Azad Jammu & Kashmir
LLB FIVE YEARS DEGREE PROGRAMME NOTES According to the Syllabus of University of Azad Jammu & Kashmir Muzaffarabad and Other Public, Private Sector Universities of Pakistan Prepared By Advocate Muhammad Adnan Masood Joja Sardar Javed Zahoor Khan (Advocate) CITI Law College Rawalakot 05824-442207, 444222, 0332-4573251, 051-4852737 Near CMH Rawalakot AJK Web:-www.clc.edu.pk Citi Law College, Near CMH, Rawalakot Ph: 05824-442207, 051-4852737 www.clc.edu.pk Page | 1 Citi Law College, Near CMH, Rawalakot Ph: 05824-442207, 051-4852737 www.clc.edu.pk Page | 2 Citi Law College, Near CMH, Rawalakot Ph: 05824-442207, 051-4852737 www.clc.edu.pk Page | 3 Citi Law College, Near CMH, Rawalakot Ph: 05824-442207, 051-4852737 www.clc.edu.pk Page | 4 Citi Law College, Near CMH, Rawalakot Ph: 05824-442207, 051-4852737 www.clc.edu.pk Page | 5 FUNCTIONAL ENGLISH Citi Law College, Near CMH, Rawalakot Ph: 05824-442207, 051-4852737 www.clc.edu.pk Page | 6 Parts of Speech NOUNS A noun is the word that refers to a person, thing or abstract idea. A noun can tell you who or what. There are several different types of noun: - There are common nouns such as dog, car, chair etc. Nouns that refer to things which can be counted (can be singular or plural) are countable nouns. Nouns that refer to some groups of countable nouns, substances, feelings and types of activity (can only be singular) are uncountable nouns. Nouns that refer to a group of people or things are collective nouns. Nouns that refer to people, organizations or places are proper nouns, only proper nouns are capitalized. -

MBBS / BDS ADMISSIONS Government Medical Colleges of Azad Jammu & Kashmir (AJ&K) and Reserved Seats for AJ&K Nationals in Pakistan, Session 2019-2020
University of Health Sciences Lahore MBBS / BDS ADMISSIONS Government Medical Colleges of Azad Jammu & Kashmir (AJ&K) and Reserved Seats for AJ&K Nationals in Pakistan, Session 2019-2020 Online applications are invited from eligible (First Class State Subject) candidates for admissions in First Year MBBS and BDS against reserved seats for AJ&K Nationals, Refugees 1947and Refugees 1989 (conditions apply), in the following Public Sector Medical/Dental Colleges of Pakistan (Punjab, Khyber Pakhtunkhwa, Balochistan & Sindh) and Public Sector Medical Colleges of AJ&K. Admissions will be made strictly on merit basis as per PM&DC Admission Regulations and Admission Policy of AJ&K Government in vogue: Medical/Dental Institutions of Pakistan Punjab (MBBS) Khyber Pakhtunkhwa (MBBS) Allama Iqbal Medical University Lahore Ayub Medical College Abbottabad Fatima Jinnah Medical University Lahore Gomal Medical College D.I Khan King Edward Medical University Lahore Khyber Medical University Peshawar Nishtar Medical University Multan Saidu Sharif Medical College Swat Punjab Medical University Faisalabad Khyber Pakhtunkhwa (BDS) Quaid e Azam Medical College Bahawalpur Dental Unit Ayub Medical College Abbottabad Rawalpindi Medical University Rawalpindi Sindh (MBBS) Services Institute of Medical Sciences Lahore Chandka Medical College Larkana Sheikh Zayad Medical College Rahim Yar Khan Balochistan (MBBS) Punjab (BDS) Bolan Medical College Quetta de’Montmorency College of Dentistry Lahore Medical Institutions of AJ&K Azad Jammu Kashmir Medical College Muzaffarabad Mohtarma Be’Nazir Bhutto Shaheed Medical College Mirpur Poonch Medical College Rawalakot 1. ELIGIBILITY CRITERIA i) Qualifications: In accordance with “MBBS and BDS (Admissions, House Job and Internship) Regulations, 2018, as amended on 30th May, 2019” of Pakistan Medical and Dental Council, the required qualifications for admissions are as follows: The applicant has passed, obtaining minimum Seventy percent (770/1100) marks, in Higher Secondary School Certificate (HSSC) or F.Sc. -

Prevalence of Diabetes Mellitus in Mirpur and Kotli Districts of Azad Jammu & Kashmir (Aj&K)
Sarhad J. Agric. Vol. 23, No. 4, 2007 PREVALENCE OF DIABETES MELLITUS IN MIRPUR AND KOTLI DISTRICTS OF AZAD JAMMU & KASHMIR (AJ&K) Saleem Khan *, M. Abbas *, Fozia Habib ** , Iftikhar H. Khattak *, and N. Iqbal * ABSTRACT Prevalence of Diabetes Mellitus was investigated in the two districts of AJ&K, Mirpur and Kotli. A total of 600 families were randomly selected from both districts for the study. A questionnaire, containing information about diabetes and diet, was filled from a responsible individual of above 30 years of each family. The mean prevalence of diabetes mellitus was 1.77% in the target area. The prevalence was higher in male (1.01%) than female (0.76%). The consumption of milk and meat of people in the area was lower than the recommended amount. The findings indicated that at present, the prevalence of diabetes is not of great concern in AJ&K. However, preventive measure should be taken to avoid the serious consequences of this killer disease. Keywords: Azad Jammu and Kashmir, Diabetes mellitus, Nutrition, Pakistan, Prevalence INTRODUCTION Diabetes mellitus is a major health problem around MATERIALS AND METHODS the globe (King and Rewers, 1993). According to The survey was conducted in the districts Kotli and WHO, prevalence of diabetes mellitus in Pakistan Mirpur of Azad Jammu & Kashmir (AJ&K) from ranked 8 in the world and with present lifestyle this April 20 to September 23, 2005. One city, one ratio will increase (King and Rewers, 1993; King town and one village were selected from each et al., 1995). The prevalence of diabetes in the district as shown in Table I. -
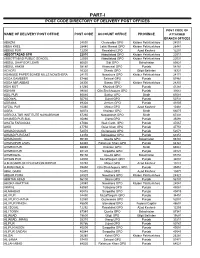
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Surface Rupture of the 2005 Kashmir, Pakistan, Earthquake and Its Active
Bulletin of the Seismological Society of America, Vol. 98, No. 2, pp. 521–557, April 2008, doi: 10.1785/0120070073 Ⓔ Surface Rupture of the 2005 Kashmir, Pakistan, Earthquake and Its Active Tectonic Implications by Heitaro Kaneda, Takashi Nakata, Hiroyuki Tsutsumi, Hisao Kondo, Nobuhiko Sugito, Yasuo Awata, Sardar S. Akhtar, Abdul Majid, Waliullah Khattak, Adnan A. Awan, Robert S. Yeats, Ahmad Hussain, Muhammad Ashraf, Steven G. Wesnousky, and Allah B. Kausar Abstract To provide a detailed record of a relatively rare thrust surface rupture and examine its active tectonic implications, we have conducted field mapping of the sur- M face rupture associated with the 2005 w 7.6 Kashmir earthquake. Despite the diffi- culty arising from massive earthquake-induced landslides along the surface rupture, we found that typical pressure ridges and warps extend northwestward for a distance of ∼70 km, with a northeast-side-up vertical separation of up to ∼7 m. Neither the main frontal thrust nor the main boundary thrust is responsible for the earthquake, but three active faults or fault segments within the Sub-Himalaya, collectively called the Balakot–Bagh fault, compose the causative fault. Although the fault exhibits sub- stantial geomorphic expression of repeated similar surface ruptures, only a part of it had been mapped as active before the earthquake. The location of the hypocenter suggests that the rupture was initiated at a deep portion of the northern–central seg- ment boundary and propagated bilaterally to eventually break all three segments. Our obtained surface rupture traces and the along-strike-slip distribution are both in good agreement with results of prompt analyses of satellite images, indicating that space geodesy can greatly aid in time-consuming field mapping of surface ruptures. -

A Preliminary Study on Distribution of Avian Fauna of Muzaffarabad–Azad Jammu and Kashmir, Pakistan
INTERNATIONAL JOURNAL OF AGRICULTURE & BIOLOGY 1560–8530/2004/06–2–300–302 http://www.ijab.org A Preliminary Study on Distribution of Avian Fauna of Muzaffarabad–Azad Jammu and Kashmir, Pakistan MUHAMMAD NAEEM AWAN, MUHAMMAD SIDDIQUE AWAN, KHAWAJA BASHARAT AHMED, ALEEM AHMED KHAN† AND NAEEM IFTIKHAR DAR‡ Department of Zoology, University of Azad Jammu & Kashmir, Muzaffarabad–Azad Jammu and Kashmir, Pakistan †Institute of Pure and Applied Biology, Baha-ud-din Zakaria University, Multan ‡Department of Wildlife, Muzaffarabad–Azad Jammu and Kashmir, Pakistan ABSTRACT Survey of avian fauna along both sides of river Neelum and Jhelum in Muzaffarabad city was conducted from June 2000 to February 2001. A total of 59 species belonging to nine orders and 31 families were recorded. Out of these: 24 were resident, 14 were winter visitor, 11 were summer visitor and 10 were rare. The distribution and abundance varied with season and maximum number of species was found during the monsoon season when most of the birds migrate for breeding. Among bird species, adapted to diverse habitat in the city, Black Drongos, House Sparrows, Common Mynas, Red vented Bulbuls, White cheeked Bulbul and House Swifts were prominent. Human related impacts such as grazing by livestock, removal of shrub cover, disturbance of habitat etc. were also studied. Key Words: Avian fauna; Distribution; Muzaffarabad; Azad Kashmir; Pakistan INTRODUCTION objectives: a) To study the distribution and status of Avian fauna of Muzaffarabad city and its relation to other fauna, Azad Jammu and Kashmir is situated at foothills of flora and agricultural crops present in the area, b) To find Himaliyas. -

Find Address of Your Nearest Loan Center and Phone Number of Concerned Focal Person
Find address of your nearest loan center and phone number of concerned focal person Loan Center/ S.No. Province District PO Name City / Tehsil Focal Person Contact No. Union Council/ Location Address Branch Name Akhuwat Islamic College Chowk Oppsite Boys College 1 Azad Jammu and Kashmir Bagh Bagh Bagh Nadeem Ahmed 0314-5273451 Microfinance (AIM) Sudan Galli Road Baagh Akhuwat Islamic Muzaffarabad Road Near main bazar 2 Azad Jammu and Kashmir Bagh Dhir Kot Dhir Kot Nadeem Ahmed 0314-5273451 Microfinance (AIM) dhir kot Akhuwat Islamic Mang bajri arja near chambar hotel 3 Azad Jammu and Kashmir Bagh Harighel Harighel Nadeem Ahmed 0314-5273451 Microfinance (AIM) Harighel Akhuwat Islamic 4 Azad Jammu and Kashmir Bhimber Bhimber Bhimber Arshad Mehmood 0346-4663605 Kotli Mor Near Muslim & School Microfinance (AIM) Akhuwat Islamic 5 Azad Jammu and Kashmir Bhimber Barnala Barnala Arshad Mehmood 0346-4663605 Main Road Bimber & Barnala Road Microfinance (AIM) Akhuwat Islamic Main choki Bazar near Sir Syed girls 6 Azad Jammu and Kashmir Bhimber Samahni Samahni Arshad Mehmood 0346-4663605 Microfinance (AIM) College choki Samahni Helping Hand for Adnan Anwar HHRD Distrcict Office Relief and Hattian,Near Smart Electronics,Choke 7 Azad Jammu and Kashmir Hattian Hattian UC Hattian Adnan Anwer 0341-9488995 Development Bazar, PO, Tehsil and District (HHRD) Hattianbala. Helping Hand for Adnan Anwar HHRD Distrcict Office Relief and Hattian,Near Smart Electronics,Choke 8 Azad Jammu and Kashmir Hattian Hattian UC Langla Adnan Anwer 0341-9488995 Development Bazar, PO, Tehsil and District (HHRD) Hattianbala. Helping Hand for Relief and Zahid Hussain HHRD Lamnian office 9 Azad Jammu and Kashmir Hattian Hattian UC Lamnian Zahid Hussain 0345-9071063 Development Main Lamnian Bazar Hattian Bala.