Use of Transdermal Nicotine Systems in a Possible Suicide Attempt
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Substance Use Resources for Grades 7-12
1 Substance Use Resources for Grades 7-12 Online Resource Library Search: https://www.voa-dakotas.org/resource-library Addiction: page 1 Alcohol: page 1 Drugs: page 4 Vaping/tobacco: page 10 Addiction Addiction and the Human Brain o DVD, 2006, HRM, 27 minutes, Grades 7-12 o Drug addiction is a disease of the brain and teens are at highest risk for acquiring this disease. This DVD explains the changes to the brain caused by prolonged use of drugs and shows why voluntary drug use eventually becomes involuntary and compulsive. Studies indicate that drugs affect the developing brain more than the brain of someone more mature, thus putting teens at a higher risk of addiction. Interviews with recovering teen addicts, an addiction counselor, and brain experts and researchers provide sobering considerations to viewers. Pre- and Post-tests are included. How Addiction Hijacks the Brain o DVD, 2016, HRM, CC, 24 minutes, Grades 7-College o This film drives home the message that drug and alcohol addiction are a disease of the brain and that teens are at highest risk for acquiring this disease. Leading scientists detail how drugs like heroin, nicotine, cocaine and marijuana change the brain, subvert the way it registers pleasure, and corrupt learning and motivation. Young recovering addicts provide a human face to the effects of drugs and alcohol as they describe how addiction involves intense craving for a drug and loss of control over its use. Viewers also learn that the brain’s plasticity, or ability to change, offers hope for addicts that they can turn their lives around. -

Smoking Cessationreview Smoking Cessation YEARS Research Review MAKING EDUCATION EASY SINCE 2006
RESEARCH Smoking CessationREVIEW Smoking Cessation YEARS Research Review MAKING EDUCATION EASY SINCE 2006 Making Education Easy Issue 24 – 2016 In this issue: Welcome to issue 24 of Smoking Cessation Research Review. Encouraging findings suggest that varenicline may increase smoking abstinence rates in light smokers Have combustible cigarettes (5–10 cigarettes per day). However, since the study was conducted in a small cohort of predominantly White met their match? cigarette smokers, it will be interesting to see whether the results can be generalised to a larger population Supporting smokers with that is more representative of the real world. depression wanting to quit Computer-generated counselling letters that target smoking reduction effectively promote future cessation, Helping smokers quit after report European researchers. Their study enrolled smokers who did not intend to quit within the next diagnosis of a potentially 6 months. At the end of this 24-month investigation, 6-month prolonged abstinence was significantly higher curable cancer amongst smokers who received individually tailored letters compared with those who underwent follow-up assessments only. Preventing postpartum return to smoking We hope you enjoy the selection in this issue, and we welcome any comments or feedback. Varenicline assists smoking Kind Regards, cessation in light smokers Brent Caldwell Natalie Walker [email protected] [email protected] Novel pMDI doubles smoking quit rates Progress towards the Smokefree 2025 goal: too slow Independent commentary by Dr Brent Caldwell. Brent Caldwell was a Senior Research Fellow at Wellington Asthma Research Group, and worked on UK data show e-cigarettes are the Inhale Study. His main research interest is in identifying and testing improved smoking cessation linked to successful quitting methods, with a particular focus on clinical trials of new smoking cessation pharmacotherapies. -

Epidemic of Prescription Drug Overdose in Ohio
EPIDEMIC OF PRESCRIPTION There were more deaths in 2008 and 2009 in Ohio from D RUG OVERDOSE IN OHIO unintentional drug overdose than from DID YOU KNOW? motor vehicle In 2007, unintentional drug poisoning became the leading crashes! cause of injury death in Ohio, surpassing motor vehicle crashes and suicide for the first time on record. This trend continued in 2009. (See Figure 1) Among the leading causes of injury death (see below), unintentional poisonings increased from the cause of the fewest number of annual deaths in 1999 (369 deaths) to the greatest in 2009 (1,817).i (See Figure 2) From 1999 to 2009, Ohio’s death rate due to unintentional drug poisonings increased 335 percent, and the increase in deaths has been driven largely by prescription drug overdoses. In Ohio, there were 327 fatal unintentional drug overdoses in 1999 growing to 1,423 annual deaths in 2009. On average, from 2006 to 2009, approximately four people died each day in Ohio due to drug overdose.v Figure 1. Number of deaths from MV traffic Figure 2 . Percent change in the number of deaths for and unintentional drug poisonings by year, the leading causes of injury, Ohio 1999-20091,2 Ohio, 2000-20091,2 1800 all unintentional 39% 1600 firearm related 15% 1400 1200 homicide 34% 1000 unintentional suicide 17% 800 poisoning 600 unintentional poisoning 301% unt MV traffic Number of deathsNumber 400 unt MV traffic -31% 200 unintentional falls 100% 0 -100% 0% 100% 200% 300% 400% Percent change from 2000-2009 Year 1Source: Ohio Department of Health, Office of Vital Statistics; 2 Unintentional Poisoning includes non-drug and drug-related poisoning. -

Healthy Mouth, Healthy You the Connection Between Oral and Overall Health
Healthy Mouth, Healthy You The connection between oral and overall health Your dental health is part of a bigger picture: whole-body wellness. Learn more about the relationship between your teeth, gums and the rest of your body. We keep you smiling® deltadentalins.com/enrollees Pregnancy Pregnancy is a crucial time to take care of your oral health. Hormonal changes may increase the risk of gingivitis, or inflammation of the gums. Symptoms include tenderness, swelling and bleeding of the gums. Without proper care, these problems may become more serious and can lead to gum disease. Gum disease is linked to premature birth and low birth weight. If you notice any changes in your mouth during pregnancy, see your dentist. WHAT YOU CAN DO • Be vigilant about your oral health. Brush twice daily and floss at least once a day — these basic oral health practices will help reduce plaque buildup and keep your mouth healthy. • Talk to your dentist. Always let your dentist know that you are pregnant. • Eat well. Choose nutritious, well-balanced meals, including fresh fruits, raw vegetables and dairy products. Athletics Sports and exercise are great ways to build muscle and improve cardiovascular health, but they can also increase risks to your oral health. Intense exercise can dry out the mouth, leading to a greater chance of tooth decay. If you play a high-impact sport without proper protection, you risk knocking out a tooth or dislocating your jaw. WHAT YOU CAN DO • Hydrate early. Prevent dehydration by drinking water during your workout — and several hours beforehand. • Skip the sports drinks. -

July 2021 L.A. Care Health Plan Medi-Cal Dual Formulary
L.A. Care Health Plan Medi-Cal Dual Formulary Formulary is subject to change. All previous versions of the formulary are no longer in effect. You can view the most current drug list by going to our website at http://www.lacare.org/members/getting-care/pharmacy-services For more details on available health care services, visit our website: http://www.lacare.org/members/welcome-la-care/member-documents/medi-cal LA1308E 02/20 EN lacare.org Last Updated: 07/01/2021 INTRODUCTION Foreword Te L.A. Care Health Plan (L.A. Care) Medi-Cal Dual formulary is a preferred list of covered drugs, approved by the L.A. Care Health Plan Pharmacy Quality Oversight Committee. Tis formulary applies only to outpatient drugs and self-administered drugs not covered by your Medicare Prescription Drug Beneft. It does not apply to medications used in the inpatient setting or medical ofces. Te formulary is a continually reviewed and revised list of preferred drugs based on safety, clinical efcacy, and cost-efectiveness. Te formulary is updated on a monthly basis and is efective the frst of every month. Tese updates may include, and are not limited to, the following: (i) removal of drugs and/or dosage forms, (ii) changes in tier placement of a drug that results in an increase in cost sharing, and (iii) any changes of utilization management restrictions, including any additions of these restrictions. Updated documents are available online at: lacare.org/members/getting-care/pharmacy-services. If you have questions about your pharmacy coverage, call Customer Solutions Center at 1-888-839-9909 (TTY 711), available 24 hours a day, 7 days a week. -

Suicides Due to Alcohol And/Or Drug Overdose
Suicides Due to Alcohol and/or Drug Overdose A Data Brief from the National Violent Death Reporting System National Center for Injury Prevention and Control Division of Violence Prevention Background Suicide occurs when a person ends his or her own life. It is the 11th leading cause of death among NVDRS is a state-based system for Americans, and every year more than 33,000 providing detailed information about people end their own lives. Suicide is found in violent deaths, such as when, where, every age, racial, and ethnic group to differing and how they happen and other possible degrees (1). contributing factors. This information can be used to monitor homicides and There are a number of factors that increase the suicides and design and evaluate prevention likelihood a person will take his or her own life; strategies. Benefits of NVDRS include the one of these is abusing substances such as alcohol following: and drugs (1). Alcohol and drug abuse are second only to depression and other mood disorders as• Linked records describing the detailed the most frequent risk factors for suicidal behavior circumstances that may contribute to a (2, 3). Alcohol and some drugs can result in a loss violent death of inhibition, may increase impulsive behavior, can lead to changes in the brain that result in • Identification of violent deaths occurring depression over time, and can be disruptive to together to help describe the circumstance relationships— resulting in alienation and a loss of multiple homicides or homicide- of social connection (4). Furthermore, excessive suicides acute drug and/or alcohol ingestion could result in death. -

Juul and Other High Nicotine E-Cigarettes Are Addicting a New Generation of Youth
JUUL AND OTHER HIGH NICOTINE E-CIGARETTES ARE ADDICTING A NEW GENERATION OF YOUTH Launched in 2015, JUUL quickly disrupted the e-cigarette marketplace, popularizing e-cigarette devices that are sleek, discreet and have sweet flavors and a powerful nicotine hit. Nicotine is highly addictive, can negatively impact the development of the adolescent brain, and can harm the cardiovascular system.1 Youth e-cigarette use in the United States has skyrocketed to what the U.S. Surgeon General and the FDA have called “epidemic” levels, with 3.6 million middle and high school students using e- cigarettes. 2 Former FDA Commissioner Scott Gottlieb has stated, “There’s no question the Juul product drove a lot of the youth use.”3 The Surgeon General has called for “aggressive steps to protect our children from these highly potent products that risk exposing a new generation of young people to nicotine.”4 Use of Nicotine Salts Makes it Easier for New Users to Try E-Cigarettes Just like the tobacco industry has used additives and design changes to make cigarettes more addictive and appealing to new users (particularly youth),5 JUUL pioneered a new e-liquid formulation that delivers nicotine more effectively and with less irritation than earlier e-cigarette models. According to the company, the nicotine in JUUL is made from “nicotine salts found in leaf tobacco, rather than free-base nicotine,” in order to “accommodate cigarette-like strength nicotine levels.”6 JUUL’s original patent stated that, “certain nicotine salt formulations provide satisfaction in an individual superior to that of free base nicotine, and more comparable to the satisfaction in an individual smoking a traditional cigarette. -

The Biden-Harris Administration's Statement of Drug Policy Priorities
EXECUTIVE OFFICE OF THE PRESIDENT OFFICE OF NATIONAL DRUG CONTROL POLICY Washington, DC 20503 The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One The overdose and addiction crisis has taken a heartbreaking toll on far too many Americans and their families. Since 2015, overdose death numbers have risen 35 percent, reaching a historic high of 70,630 deaths in 2019.1 This is a greater rate of increase than for any other type of injury death in the United States.2 Though illicitly manufactured fentanyl and synthetic opioids other than methadone (SOOTM) have been the primary driver behind the increase, overdose deaths involving cocaine and other psychostimulants, like methamphetamine,3 have also risen in recent years, particularly in combination with SOOTM. New data suggest that COVID-19 has exacerbated the epidemic,4, 5 and increases in overdose mortality6 have underscored systemic inequities in our nation’s approach to criminal justice and prevention, treatment, and recovery. President Biden has made clear that addressing the overdose and addiction epidemic is an urgent priority for his administration. In March, the President signed into law the American Rescue Plan, which appropriated nearly $4 billion to enable the Substance Abuse and Mental Health Services Administration and the Health Resources and Services Administration to expand access to vital behavioral health services. President Biden has also said that people should not be incarcerated for drug use but should be offered treatment instead. The President has also emphasized the need to eradicate racial, gender, and economic inequities that currently exist in the criminal justice system. -
Bupropion + Patch
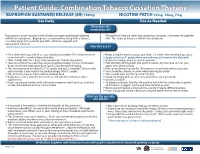
Patient Guide: Combination Tobacco Cessation Therapy BUPROPION SUSTAINED RELEASE (SR) 150mg NICOTINE PATCH 21mg, 14mg, 7mg Use Daily Use As Needed What does this medication do? Bupropion is a non-nicotine aid that helps you quit smoking by reducing The patch will release small, but continuous amounts of nicotine through the withdrawal symptoms. Bupropion is recommended along with a tobacco skin. This helps to decrease withdrawal symptoms. cessation program to provide you with additional support and educational materials. How do I use it? BUPROPION SUSTAINED RELEASE (SR) 150mg NICOTINE PATCH 21mg, 14mg, 7mg Set a date when you intend to stop smoking (quit date). The medicine needs Begin using the patch on your quit date, 1-2 weeks after starting bupropion. to be started 1-2 weeks before that date. Apply only one (1) patch when you wake up and remove the old patch. Take 1 tablet daily for 3 days, then increase to 1 tablet twice daily. If you miss a dose, use it as soon as you can. Take at a similar time each day, allowing approximately 8 hours in between Peel the back off the patch and put it on clean, dry, hair-free skin on your doses. Don’t take bupropion past 5pm to avoid trouble sleeping. upper arm, chest or back. This medicine may be taken for 7-12 weeks and up to 6 months. Discuss with Press patch firmly in place for 10 seconds so it will stick well to your skin. your provider if you need to be treated longer than 12 weeks. -
Use of Non Cigarette Tobacco Products (NCTP) Smokeless
Non Cigarette Tobacco Products (NCTP) and Electronic cigarettes (e-cigs) Michael V. Burke EdD Asst: Professor of Medicine Nicotine Dependence Center Mayo Clinic, Rochester, MN Email: [email protected] ©2011 MFMER | slide-1 Goals & Objectives • Review NCTP definitions & products • Discuss prevalence/trends of NCTP • Discuss NCTP and addiction • Review recommended treatments for NCTP ©2011 MFMER | slide-2 NCTP Definitions & Products ©2011 MFMER | slide-3 Pipes ©2011 MFMER | slide-4 Cigars Images from www.trinketsandtrash.org ©2011 MFMER | slide-5 Cigar Definition U.S. Department of Treasury (1996): Cigar “Any roll of tobacco wrapped in leaf tobacco or any substance containing tobacco.” vs. Cigarette “Any roll of tobacco wrapped in paper or in any substance not containing tobacco.” ©2011 MFMER | slide-6 NCI Monograph 9. Cigars: Health Effects and Trends. ©2011 MFMER | slide-7 ©2011 MFMER | slide-8 Smokeless Tobacco Chewing tobacco • Loose leaf (i.e., Redman) • Plugs • Twists Snuff • Moist (i.e., Copenhagen, Skoal) • Dry (i.e., Honest, Honey bee, Navy, Square) ©2011 MFMER | slide-9 “Chewing Tobacco” = Cut tobacco leaves ©2011 MFMER | slide-10 “Snuff” = Moist ground tobacco ©2011 MFMER | slide-11 Type of ST Used in U.S. Chewing Tobacco Snuff National Survey on Drug Use and Health (NSDUH) ©2011 MFMER | slide-12 “Spitless Tobacco” – Star Scientific ©2011 MFMER | slide-13 RJ Reynold’s ©2011 MFMER | slide-14 “Swedish Style” ST ©2011 MFMER | slide-15 Phillip Morris (Altria) ©2011 MFMER | slide-16 New Product: “Fully Dissolvables” ©2011 MFMER -

Transdermal Nicotine Maintenance Attenuates the Subjective And
Neuropsychopharmacology (2004) 29, 991–1003 & 2004 Nature Publishing Group All rights reserved 0893-133X/04 $25.00 www.neuropsychopharmacology.org Transdermal Nicotine Maintenance Attenuates the Subjective and Reinforcing Effects of Intravenous Nicotine, but not Cocaine or Caffeine, in Cigarette-Smoking Stimulant Abusers 1 1 ,1,2 Bai-Fang X Sobel , Stacey C Sigmon and Roland R Griffiths* 1Department of Psychiatry and Behavioral Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Department of Neuroscience, Johns Hopkins University School of Medicine, Baltimore, MD, USA The effects of transdermal nicotine maintenance on the subjective, reinforcing, and cardiovascular effects of intravenously administered cocaine, caffeine, and nicotine were examined using double-blind procedures in nine volunteers with histories of using tobacco, caffeine, and cocaine. Each participant was exposed to two chronic drug maintenance phases (21 mg/day nicotine transdermal patch and placebo transdermal patch). Within each drug phase, the participant received intravenous injections of placebo, cocaine (15 and 30 mg/70 kg), caffeine (200 and 400 mg/70 kg), and nicotine (1.0 and 2.0 mg/70 kg) in mixed order across days. Subjective and cardiovascular data were collected before and repeatedly after drug or placebo injection. Reinforcing effects were also assessed after each injection with a Drug vs Money Multiple-Choice Form. Intravenous cocaine produced robust dose-related increases in subjective and reinforcing effects; these effects were not altered by nicotine maintenance. Intravenous caffeine produced elevations on several subjective ratings; nicotine maintenance did not affect these ratings. Under the placebo maintenance condition, intravenous nicotine produced robust dose-related subjective effects, with maximal increases similar to the high dose of cocaine; nicotine maintenance significantly decreased the subjective and reinforcing effects of intravenous nicotine. -

April 9, 2021 Addiction in the News
UC CAR Weekly Newsletter 4.9.2021 Welcome to the weekly newsletter from the Center for Addiction Research! Each newsletter includes highlights from addiction in the news topics, active funding opportunities offered by NIDA/NIAAA, and information about any new publications from CAR members. Please email Jen Rowe ([email protected]) to change your communication preferences. Thank you. Thank you for your interest in the Center for Addiction Research - our mission is to accelerate scientific progress in the prevention and treatment of substance use disorders and their consequences by fostering research collaborations across: 1) UC departments, colleges, and centers including Cincinnati Children’s Hospital Medical Center; 2) Local, regional, and state community and governmental partners; and 3) Other academic institutions and industry." April 9, 2021 Addiction in the News UC/ Regional News Opinion: Our society often punishes individuals struggling with addiction The recent settlement announced between the state of Ohio and consulting business McKinsey & Co. for the firm's role in creating and fueling the opioid epidemic is a perfect example of how we unfairly punish Ohioans dealing with substance-use disorder while allowing the engineers of this crisis to escape with just a slap on the wrist. More than 200,000 lives have been lost to the opioid… The Opioid Crisis Was America’s Epidemic Before COVID. Research Suggests that Overdoses Hurt Student Achievement Long before the emergence of COVID-19, the United States was struggling to contain a years-long opioid crisis that took tens of thousands of lives every year. Now, with Oxycontin manufacturer Purdue Pharma still negotiating billion-dollar penalties for its role in the two-decade drug epidemic, experts have begun taking the measure of its impact on student learning.