A Variation in the Formation of the Median Nerve: Communicating Branch Between the Musculocutaneous and Median Nerves in Man
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomical Variations of the Brachial Plexus Terminal Branches in Ethiopian Cadavers
ORIGINAL COMMUNICATION Anatomy Journal of Africa. 2017. Vol 6 (1): 896 – 905. ANATOMICAL VARIATIONS OF THE BRACHIAL PLEXUS TERMINAL BRANCHES IN ETHIOPIAN CADAVERS Edengenet Guday Demis*, Asegedeche Bekele* Corresponding Author: Edengenet Guday Demis, 196, University of Gondar, Gondar, Ethiopia. Email: [email protected] ABSTRACT Anatomical variations are clinically significant, but many are inadequately described or quantified. Variations in anatomy of the brachial plexus are important to surgeons and anesthesiologists performing surgical procedures in the neck, axilla and upper limb regions. It is also important for radiologists who interpret plain and computerized imaging and anatomists to teach anatomy. This study aimed to describe the anatomical variations of the terminal branches of brachial plexus on 20 Ethiopian cadavers. The cadavers were examined bilaterally for the terminal branches of brachial plexus. From the 40 sides studied for the terminal branches of the brachial plexus; 28 sides were found without variation, 10 sides were found with median nerve variation, 2 sides were found with musculocutaneous nerve variation and 2 sides were found with axillary nerve variation. We conclude that variation in the median nerve was more common than variations in other terminal branches. Key words: INTRODUCTION The brachial plexus is usually formed by the may occur (Moore and Dalley, 1992, Standring fusion of the anterior primary rami of the C5-8 et al., 2005). and T1 spinal nerves. It supplies the muscles of the back and the upper limb. The C5 and C6 fuse Most nerves in the upper limb arise from the to form the upper trunk, the C7 continues as the brachial plexus; it begins in the neck and extends middle trunk and the C8 and T1 join to form the into the axilla. -

Anastomotic Branch from the Median Nerve to the Musculocutaneous Nerve: a Case Report
Case Report www.anatomy.org.tr Recieved: February 10, 2008; Accepted: April 22, 2008; Published online: October 31, 2008 doi:10.2399/ana.08.063 Anastomotic branch from the median nerve to the musculocutaneous nerve: a case report Feray Güleç Uyaro¤lu1, Gülgün Kayal›o¤lu2, Mete Ertürk2 1Department of Neurology, Ege University Faculty of Medicine, Izmir, Turkey 2Department of Anatomy, Ege University Faculty of Medicine, Izmir, Turkey Abstract Anomalies of the brachial plexus and its terminal branches are not uncommon. Communicating branch arising from the mus- culocutaneous nerve to the median nerve is a frequent variation, whereas the presence of an anastomotic branch arising from the median nerve and joining the musculocutaneous nerve is very rare. During routine dissection of cadaver upper limbs, we observed an anastomotic branch arising from the median nerve running distally to join with the branches of the musculocutaneous nerve in a left upper extremity. The anastomotic branch originated from the median nerve 11.23 cm prox- imal to the interepicondylar line. After running distally and coursing between the biceps brachii and the brachialis muscles, this anastomotic branch communicated with two branches of the musculocutaneous nerve separately. The presence of the communicating branches between these nerves should be considered during surgical interventions and clinical investigations of the arm. Key words: anatomy; brachial plexus; communicating branch; upper limb; variation Anatomy 2008; 2: 63-66, © 2008 TSACA Introduction neous nerve (C5, C6, and C7) connects with the median nerve in the arm.2,3 The musculocutaneous nerve is the Variations of the brachial plexus and its terminal continuation of the lateral cord of the brachial plexus. -

Anatomical Study of the Brachial Plexus in Human Fetuses and Its Relation with Neonatal Upper Limb Paralysis
ORIGINAL ARTICLE Anatomical study of the brachial plexus Official Publication of the Instituto Israelita de Ensino e Pesquisa Albert Einstein in human fetuses and its relation with neonatal upper limb paralysis ISSN: 1679-4508 | e-ISSN: 2317-6385 Estudo anatômico do plexo braquial de fetos humanos e sua relação com paralisias neonatais do membro superior Marcelo Rodrigues da Cunha1, Amanda Aparecida Magnusson Dias1, Jacqueline Mendes de Brito2, Cristiane da Silva Cruz1, Samantha Ketelyn Silva1 1 Faculdade de Medicina de Jundiaí, Jundiaí, SP, Brazil. 2 Centro Universitário Padre Anchieta, Jundiaí, SP, Brazil. DOI: 10.31744/einstein_journal/2020AO5051 ❚ ABSTRACT Objective: To study the anatomy of the brachial plexus in fetuses and to evaluate differences in morphology during evolution, or to find anatomical situations that can be identified as the cause of obstetric paralysis. Methods: Nine fetuses (12 to 30 weeks of gestation) stored in formalin were used. The supraclavicular and infraclavicular parts of the brachial plexus were dissected. Results: In its early course, the brachial plexus had a cord-like shape when it passed through the scalene hiatus. Origin of the phrenic nerve in the brachial plexus was observed in only one fetus. In the deep infraclavicular and retropectoralis minor spaces, the nerve fibers of the brachial plexus were distributed in the axilla and medial bicipital groove, where they formed the nerve endings. Conclusion: The brachial plexus of human fetuses presents variations and relations with anatomical structures that must be considered during clinical and surgical procedures for neonatal paralysis of the upper limbs. How to cite this article: Cunha MR, Dias AA, Brito JM, Cruz CS, Silva Keywords: Brachial plexus/anatomy & histology; Fetus/abnormalities; Paralysis SK. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -

Multiple Nerve Injuries Following Repair of a Distal Biceps Tendon Rupture Case Report and Review of the Literature
166 Bulletin of the Hospital for Joint Diseases 2013;71(2):166-9 Multiple Nerve Injuries Following Repair of a Distal Biceps Tendon Rupture Case Report and Review of the Literature Marc R. Fajardo, M.D., Zehava Rosenberg, M.D., Dimitrios Christoforou, M.D., and John A. I. Grossman, M.D., F.A.C.S. Abstract We present the case of a patient, with a surgically repaired Current repair of a distal biceps tendon rupture has reverted distal biceps tendon rupture performed through a single to the single incision technique. Postoperative complications incision, with injury to both the posterior interosseus and are rare, but the most common are due to neuropraxia. We lateral antebrachial cutaneous nerves. present the case of patient who sustained multiple nerve injuries following distal biceps repair. This case is presented Case Report with a review of the literature. A healthy, right-hand dominant 51-year-old man sustained injury to his right distal biceps while shoveling dirt. He was upture of the distal end of the biceps brachialis diagnosed with an acute right distal biceps rupture (con- tendon is a relatively uncommon injury that usually firmed by ultrasound, Fig. 1) and subsequently underwent Roccurs in active, middle-aged men after an eccentric operative repair within a week of the injury. muscle contracture (often during heavy lifting). Patients The surgery was performed via a single incision. Intra- often present with pain, ecchymosis, and swelling over operatively, it was found that 90% of the distal biceps ten- the antecubital region of the dominant arm. The physical don was avulsed from the radial tuberosity. -

Some Variations in the Formation of the Brachial Plexus in Infants*
Tr. J. of Medical Sciences 29 (1999) 573–577 © TÜBİTAK Ahmet UZUN1 Some Variations in the Formation of the Brachial Sait BİLGİÇ2 Plexus in Infants* Received: June 23.1998 Abstract: The anatomical variations of the directly from a branch of the anterior brachial plexus in human have clinical division of the middle trunk (Fig.3,A). Group significance to surgeons, radiologists and 2 had three anterior division cords: a) the anatomists. We studied some variations in lateral cord formed from anterior division the formation of 130 brachial plexuses in of the upper trunk (Fig.2, A); b) an sixty-five infant cadavers (34 males, 31 “intermediate” cord formed from the females; aged 1-7 days). The brachial plexus anterior division of the middle trunk and c) consisted of the 5th, 6th, 7th, and 8th cervical the medial cord formed from the anterior spinal nerves and 1st thoracic spinal nerve division of the lower trunk (3.07%). In (69.23%). We found that among the 130 group 3, there was a rare variation of the plexuses, 30.77% also received a medial cord (1.54%) which receives an contribution from C4 (Fig.1, A ) . The anastomotic branch from the posterior variations in the formation of brachial division of the middle trunk (Fig.4, B). The 1Department of Anatomy, Inonu University, plexuses were classified into three groups. anomalies of the human brachial plexus have School of Medicine, 44100 Malatya-Turkey Group 1 had a variation in the formation of clinical importence in diagnosis of injuries of 2Department of Anatomy, Ondokuz Mayis the median nerve (10.77%), with fusion of the brachial plexus. -

High-Resolution 3T MR Neurography of the Brachial Plexus and Its Branches, with Emphasis on 3D Imaging
REVIEW ARTICLE High-Resolution 3T MR Neurography of the Brachial Plexus and Its Branches, with Emphasis on 3D Imaging A. Chhabra, G.K. Thawait, T. Soldatos, R.S. Thakkar, F. Del Grande, M. Chalian, and J.A. Carrino ABSTRACT SUMMARY: With advancement in 3D imaging, better fat-suppression techniques, and superior coil designs for MR imaging and the increasing availability and use of 3T magnets, the visualization of the complexity of the brachial plexus has become facile. The relevant imaging findings are described for normal and pathologic conditions of the brachial plexus. These radiologic findings are supported by clinical and/or EMG/surgical data, and corresponding high-resolution MR neurography images are illustrated. Because the brachial plexus can be affected by a plethora of pathologies, resulting in often serious and disabling complications, a better radiologic insight has great potential in aiding physicians in rendering superior services to patients. ABBREVIATIONS: EMG ϭ electromyography; MIP ϭ maximum intensity projection; MRN ϭ MR neurography; SPACE ϭ sampling perfection with application- optimized contrasts by using different flip angle; STIR ϭ short tau inversion recovery, TOS ϭ thoracic outlet syndrome he brachial plexus is a network of nerve confluences and ram- nerve (C5-C7) to the serratus anterior muscle arise directly from Tifications, which combine to form the large terminal branches the nerve roots.1,2,5 that supply motor and sensory branches to the upper extremities. The clinical differentiation of brachial plexopathy from other Trunks and Their Anatomic Relations spine-related abnormalities often poses a considerable diagnostic The C5 and C6 nerve roots compose the upper trunk, C7 contin- challenge, and electrodiagnostic tests are difficult to perform due ues as the middle trunk, and C8 and T1 compose the lower trunk. -

Posterior Interosseous Neuropathy Supinator Syndrome Vs Fascicular Radial Neuropathy
Posterior interosseous neuropathy Supinator syndrome vs fascicular radial neuropathy Philipp Bäumer, MD ABSTRACT Henrich Kele, MD Objective: To investigate the spatial pattern of lesion dispersion in posterior interosseous neurop- Annie Xia, BSc athy syndrome (PINS) by high-resolution magnetic resonance neurography. Markus Weiler, MD Methods: This prospective study was approved by the local ethics committee and written Daniel Schwarz, MD informed consent was obtained from all patients. In 19 patients with PINS and 20 healthy con- Martin Bendszus, MD trols, a standardized magnetic resonance neurography protocol at 3-tesla was performed with Mirko Pham, MD coverage of the upper arm and elbow (T2-weighted fat-saturated: echo time/repetition time 52/7,020 milliseconds, in-plane resolution 0.27 3 0.27 mm2). Lesion classification of the radial nerve trunk and its deep branch (which becomes the posterior interosseous nerve) was performed Correspondence to Dr. Bäumer: by visual rating and additional quantitative analysis of normalized T2 signal of radial nerve voxels. [email protected] Results: Of 19 patients with PINS, only 3 (16%) had a focal neuropathy at the entry of the radial nerve deep branch into the supinator muscle at elbow/forearm level. The other 16 (84%) had proximal radial nerve lesions at the upper arm level with a predominant lesion focus 8.3 6 4.6 cm proximal to the humeroradial joint. Most of these lesions (75%) followed a specific somato- topic pattern, involving only those fascicles that would form the posterior interosseous nerve more distally. Conclusions: PINS is not necessarily caused by focal compression at the supinator muscle but is instead frequently a consequence of partial fascicular lesions of the radial nerve trunk at the upper arm level. -

Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies
Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies Zachary Simmons, MD* KEYWORDS Brachial plexus Brachial plexopathy Axillary nerve Musculocutaneous nerve Suprascapular nerve Nerve conduction studies Electromyography KEY POINTS The brachial plexus provides all motor and sensory innervation of the upper extremity. The plexus is usually derived from the C5 through T1 anterior primary rami, which divide in various ways to form the upper, middle, and lower trunks; the lateral, posterior, and medial cords; and multiple terminal branches. Traction is the most common cause of brachial plexopathy, although compression, lacer- ations, ischemia, neoplasms, radiation, thoracic outlet syndrome, and neuralgic amyotro- phy may all produce brachial plexus lesions. Upper extremity mononeuropathies affecting the musculocutaneous, axillary, and supra- scapular motor nerves and the medial and lateral antebrachial cutaneous sensory nerves often occur in the context of more widespread brachial plexus damage, often from trauma or neuralgic amyotrophy but may occur in isolation. Extensive electrodiagnostic testing often is needed to properly localize lesions of the brachial plexus, frequently requiring testing of sensory nerves, which are not commonly used in the assessment of other types of lesions. INTRODUCTION Few anatomic structures are as daunting to medical students, residents, and prac- ticing physicians as the brachial plexus. Yet, detailed understanding of brachial plexus anatomy is central to electrodiagnosis because of the plexus’ role in supplying all motor and sensory innervation of the upper extremity and shoulder girdle. There also are several proximal upper extremity nerves, derived from the brachial plexus, Conflicts of Interest: None. Neuromuscular Program and ALS Center, Penn State Hershey Medical Center, Penn State College of Medicine, PA, USA * Department of Neurology, Penn State Hershey Medical Center, EC 037 30 Hope Drive, PO Box 859, Hershey, PA 17033. -

Upper and Lower Extremity Nerve Conduction Studies Kelly G
2019 Upper and Lower Extremity Nerve Conduction Studies Kelly G. Gwathmey October 18, 2019 Virginia Commonwealth University 2019 Financial Disclosure I have received speaking and consulting honoraria from Alexion Pharmaceuticals. 2019 Warning Videotaping or taking pictures of the slides associated with this presentation is prohibited. The information on the slides is copyrighted and cannot be used without permission and author attribution. 2019 Outline for Today’s talk • Upper extremity nerve conduction studies o Median nerve o Ulnar nerve o Radial nerve o Median comparison studies o Medial antebrachial cutaneous nerve o Lateral antebrachial cutaneous nerve • Lower extremity nerve conduction studies o Fibular nerve o Tibial nerve o Sural nerve o Femoral nerve • Saphenous • Lateral femoral cutaneous • Phrenic nerve • Facial nerve • Anomalous Innervations 2019 Median nerve anatomy • Median nerve is formed by a combination of: o Lateral cord (C6-7) supplies the sensory fibers to the thumb, index, middle finger, proximal median forearm, and thenar eminence. o Medial cord (C8-T1) provides motor fibers to the distal forearm and hand. • The median nerve innervates the pronator teres, then gives branches to the flexor carpi radialis, flexor digitorum superficialis, and palmaris longus. • Anterior Interosseus Nerve (AIN)- innervates the flexor pollicis longus, flexor digitorum profundus (FDP) (digits 2 and 3), and pronator quadratus. Preston, David C., MD; Shapiro, Barbara E., MD, PhD. Published January 1, 2013. Pages 267-288. © 2013. 2019 Median nerve anatomy • Proximal to the wrist- the palmar cutaneous sensory branch (sensation over the thenar eminence) • Through the carpal tunnel- Motor division goes to first and second lumbricals o Recurrent thenar motor branch the thenar eminence (opponens, abductor pollicis brevis, and superficial head of flexor pollicis brevis) • Sensory branch that goes through the carpal tunnel supplies the medial thumb, index finger, middle finger and lateral half of the ring finger. -
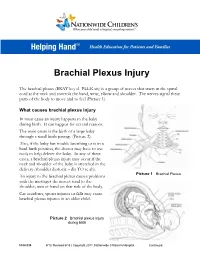
Brachial Plexus Injury
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

5. Upper Extremity Neuroanatomy
5. UPPER EXTREMITY compartments of the NEUROANATOMY arm). The brachial plexus divisions INTRODUCTION pass posterior to the mid-point of Regional anesthesia of the upper extremity in- the clavicle through volves two major nerve plexuses, the cervical plexus the cervico-axillary and the brachial plexus. A detailed understanding of canal. the anatomy of these nerve plexuses and surrounding • Three cords. The structures is essential for the safe and successful prac- divisions coalesce tice of regional anesthesia in this area of the body. to form three cords. The anterior CERVICAL PLEXUS divisions of the superior and middle The cervical plexus is formed from a series of nerve trunk form the loops between adjacent anterior rami of cervical nerve lateral cord. The roots C1 through C4. The cervical plexus is deep to the anterior division of sternocleidomastoid muscle and medial to the scalene the inferior trunk muscles. The deep branches of the plexus are motor becomes the medial nerves. They include the phrenic nerve (diaphragm cord. The posterior muscle) and the ansa cervicalis nerve (omohyoid, divisions of all sternothyroid, and sternohyoid muscles). The named three trunks unite nerves of the superficial cervical plexus are branches to form the posterior from the loops and emerge from the middle of the ster- Figure 5-1. Dissection of the superficial cervical plexus in the posterior triangle cord. The cords are nocleidomastoid muscle (Figure 5-1): BRACHIAL PLEXUS named based on their relationship to the axillary artery (as this • Lesser occipital nerve (C2): innervates the skin The brachial plexus is formed from the five roots neurovascular bundle passes in its sheath into posterior to the ear.