Case Report Bilateral TMJ Involvement in Rheumatoid Arthritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Gujarat Government Gazette SUPPLEMENT to the CENTRAL GAZETTE and CENTRAL SECTION PUBLISHED by AUTHORITY
© The Gujarat Government Gazette SUPPLEMENT TO THE CENTRAL GAZETTE AND CENTRAL SECTION PUBLISHED BY AUTHORITY VOL. LIX ] THURSDAY, 31st MAY, 2018/JYAISTHA 10, 1940 [ Issue No. 22 PART-II Miscellaneous notices and advertiseMents No Legal Responsibility Is Accepted For The Publication of Advertisement Regarding Change Of Name In Gazette Of Gujarat Persons Notifying The Changes Will Remain Solely Responsible For The Legal Consequences And Also For Any Other Misrepresentation Etc. No. OLD NAME/SURNAME NEW NAME/SURNAME 1 Ketankumar Sumanbhai Vaidh Ketankumar Sumanbhai Vaidya Rajput Para, At Po. Bantwa, Ta. Manavadar, Dist. Junagadh-362620. 2 Chandrakant Dayabhai Patel Chandrakant Dayabhai Bhalani 9, Vibhapark Society, Anantwadi, Ramabag, Bhavnagar-364001. 3 Shah Anjuben Shrenik Shah Alka Shrenik B-102, Aarsh Flats, Opp. Palak Enclave, Prerna Tirth Derasar, Ahmedabad-380015. 4 Gokul Dhanasegar Mudaliyar Gokul Dhanasegar Sengundhar 16/396, Old Slum Quarters, Khokhara, Maninagar, Ahmedabad-380008. 5 Rashmiben Vinubhai Vankar Rashmiben Vinubhai Kapadia A/6, Bansari Duplex-1, Nr. Bapodgam, Waghodia Road, Vadodara-390019. 6 Rajnikant Maheshkumar Modi Rajnikant Maheshkumar Modh 13, Balaji City, Nr. Gayatri Temple, Opp. Tirupatirajnagar, Abu Road highway, Palanpur, Dist. Banaskantha-385001. 7 Miss Patel Rekhabahen Dayaljibhai Mrs. Patel Rekhaben Nareshbhai 42, Madhav Homes, Nr. Eklavya School, Opp. Galaxy Opel, Nirant Cross Road, Vastral Road, Ahmedabad-382418. 8 Kishan Nitin Raghuvanshi Yuvraj Nitin Raghuvanshi 14-4, Devas Flat, Nr. Rajwadu Hotel, Ahmedabad-380007. 9 Judal Dansungbhai Hemarajbhai Choudhary Dansinghbhai Hemarajbhai Limdivas, At Sagrosana, Ta. Palanpur, Dist. Banaskantha-385001. 10 Judal Ambaben Dansinghbhai Choudhary Ambaben Dansinghbhai Limdivas, At Sagrosana, Ta. Palanpur, Dist. Banaskantha-385001. 11 Judal Shaileshkumar Dansinghbhai Choudhary Shaileshkumar Dansinghbhai Limdivas, At Sagrosana, Ta. -

Addor Ambition
https://www.propertywala.com/addor-ambition-ahmedabad Addor Ambition - Navrangpura, Ahmedabad Commercial and Official space available at Addor Ambition Addor Realty presents Addor Ambition with Commercial and Official space available at Navrangpura, Ahmedabad Project ID : J300822119 Builder: Addor Realty Properties: Shops, Office Spaces Location: Addor Ambition, Navrangpura, Ahmedabad (Gujarat) Completion Date: Jun, 2014 Status: Started Description Addor Ambition is a new place to do business is the start of a new era. A vibrant place like Addor Ambitiun is the inspiration to attain heights that haven't been seen before. It is the motivation to set landmarks that others will strive to conquer. A flourishing business is one that never stops growing. To nurture a business is like watering a plant. It takes an extreme amount of care and dedication. And such commitment comes only from an environment of growth like Addor Ambition. Amenities Ground + 2 level Parking Well Designed Entrance Lobby Decorative Foyer Area All common areas covered with CCTV Vitrified Tiles in Offices and Showrooms Superior Class Electrical Accessories with fire guard cables 24 hour Security & water supply Provision for Concealed Telephone, DTH & Broadband lines in each office Ultra modern elevation Showroom & offices height 10 ft Specification Structure: Earthquake resistant R.C.C frame structure Toilets: Well designed toilets for each space for your convenience Electrical: Concealed copper wiring with adequate number of points, inclusive of three phase points in all units Parking: Allotted parking for members, Ample parking space for visitors Elevators: 2 MNC Brand 10 person fully automatic Elevators. Founded as "Satva realty" about four years back by the visionary Mr Vikas Shah, and now making a global presence as Addor Realty, we are a dedicated company working towards our main mission "Delivering more than Promised". -

Ministry of Shipping
Page 1 None should be stigmatised for a crime committed as a juvenile: SC2 Transgenders’ Bill 2019 denies the community to decide their own identity — a right granted by the SC4 The Prohibition of Electronic Cigarettes (Production, Manufacture, Import, Export, Transport, Sale, Distribution, Storage and Advertisement) Bill, 20196 Taking stock of the anti-AIDS fight8 Primitive Tribals in Hilly/Forest Areas11 National Pension Scheme for Traders, Shopkeepers and Self-Employed Persons15 Residential Coaching Programmes for Sportspersons17 19 21 The many structural flaws in India’s higher education system28 Another quota question: On creamy layer for SCs30 32 Launch of 'Going Online as Leaders' Programme35 Crimes against Children36 Children in Shelter Homes39 Setting Up of Indian Institute of Skills41 National AYUSH Grid43 Counselling Programmes and Vocational Training Standards45 Sexual Cases under POCSO47 Maternity Benefits under PMMVY51 National Commission for Women54 Bharatiya POSHAN Krishi Kosh57 National Nutrition Mission59 Maternity Entitlements Under NFSA61 Promotion of AYUSH in Rural Areas66 Tertiary Care and Medical Education under PMSSY69 Funds for Anaemia Control75 Amrit Pharmacy84 Measles outbreaks continue unabated: WHO90 2.3 million children in India unvaccinated for measles92 Diversion of Tribal Land for Development Projects94 National Fellowship and Scholarship of ST Students96 Rashtriya Vayoshri Yojana for Disabled Persons99 Drug Abuse Among Youths101 The Constitution (One Hundred and Twenty-Sixth Amendment) Bill, 2019104 Measures taken by Government to prevent Crime against Women105 CAG hints at massive diversion of LPG107 Status of Women and Child Development Under SDGs of UN109 Page 2 Source : www.thehindu.com Date : 2019-12-01 NONE SHOULD BE STIGMATISED FOR A CRIME COMMITTED AS A JUVENILE: SC Relevant for: Developmental Issues | Topic: Rights & Welfare of Children - Schemes & their Performance, Mechanisms, Laws Institutions and Bodies A person should not be stigmatised for a crime committed as a juvenile, the Supreme Court has held. -

S.No. Name of Ethics Committee RC No
S.No. Name of Ethics Committee RC No. Address State All India Institute of Medical Sciences, Room No.102, 1st floor, OT Block, 1 Ethics Committee ECR/538/Inst/DL/2014/RR-17 Delhi Ansari Nagar, New Delhi-110029 Aster Aadhar Hospital, R.S. NO. 628, 'B' Ward, Near Shastri Nagar, KMT 2 Aster Aadhar Ethics Committee ECR/470/Inst/MH/2013/RR-16 Maharashtra Workshop, Kohlapur-416012 3 Visakha Institutional Review Board ECR/4/Indt/AP/2013/RR-16 A-11, Prince Villae Royal Appartment, Siripuram, Visakhapatnam- 530003 Andhra Pradesh SAUMYAA, C-321, Behind Ganesh Temple N-1, CIDCO, Aurangabad- 4 Aurangabad Ethics Committee ECR/122/Indt/MH/2013/RR-16 Maharashtra 431003 Ethics Committee of Diabetes Thyroid BCM Health Island, PU4, Scheme 54, Behind Prestige Management 5 ECR/409/Inst/MP/2013/RR-16 Madhya Pradesh Hormone Research Institute Institute, Near Bombay Hospital, Indore- 452010 Jehangir Clinical Development Centre Pvt. Ltd., Jehangir Hospital 6 Ethics Committee ECR/352/Inst/MH/2013/RR-19 Maharashtra Premises, 32 Sassoon Road, Pune- 411001 89, 3rd Cross, S V K Layout, Basaveshwar Nagar, Banagalore, Urban- 7 Lifeline Ethics Committee ECR/76/Indt/KA/2013/RR-16 Karnataka 560079 Instutional Ethics Committee-Clinical Indraprastha Apollo Hospitals, Sarita Vihar, Delhi- Mathura road, New 8 ECR/5/Inst/DL/2013/RR-16 Delhi Studies Delhi- 110076 H.No.- D/129, St. No.-13 Opp-Durga Mandir, Ashok Nagar, Shahdara- 9 Good Society for Ethical Research ECR/69/Indt/DL/2013/RR-19 Delhi 110093 Ethics Committee, S.P. Medical College & S.P Medical College & A.G Hospitals, HRMC Cardiovascular Sciences & 10 ECR/27/SP/Inst/RJ/2013/RR-16 Rajasthan A.G. -
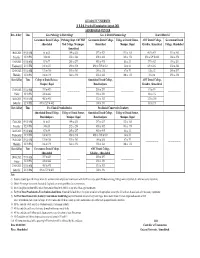
II BDS Practical Aug-2021 Ahmedabad Center
GUJARAT UNIVERSITY II B.D.S. Practical Examination August-2021 AHMEDABAD CENTER Date & Day Time Gen. Pathology & Bacteriology Gen. & Dental Pharmacology Dental Material Government Dental College, Pathology Dept, AMCMET Government Dental College, College of Dental Science, AMC Dental College, Government Dental Ahmedabad Med College, Maninagar, Ahmedabad Manipur, Bopal Khokhra, Ahmedabad College, Ahmedabad Ahmedabad 10-08-2021 09:00 AM 01 to 33 199 to 231 397 to 429 133 to 165 463 to 495 331 to 363 Tuesday 12:30 PM 34 to 66 232 to 264 430 to 462 166 to 198 496 to 529 & 602 364 to 396 11-08-2021 09:00 AM 67 to 99 265 to 297 463 to 495 01 to 33 397 to 429 199 to 231 Wednesday 12:30 PM 100 to 132 298 to 330 496 to 529 & 602 34 to 66 430 to 462 232 to 264 12-08-2021 09:00 AM 133 to 165 331 to 363 199 to 231 67 to 99 01 to 33 265 to 297 Thursday 12:30 PM 166 to 198 364 to 396 232 to 264 100 to 132 34 to 66 298 to 330 Date & Day Time College of Dental Science, Ahmedabad Dental College, AMC Dental College, Manipur, Bopal Ranchhodpura Khokhra, Ahmedabad 13-08-2021 09:00 AM 397 to 429 265 to 297 67 to 99 ------------------- ------------------- ------------------- Friday 12:30 PM 430 to 462 298 to 330 100 to 132 14-08-2021 09:00 AM 463 to 495 331 to 363 133 to 165 Saturday 12:30 PM 496 to 529 & 602 364 to 396 166 to 198 Date & Day Time Pre-Clinical Prosthodontics Pre-clinical Conservative Dentistry Ahmedabad Dental College, College of Dental Science, Ahmedabad Dental College, College of Dental Science, Ranchhodpura Manipur, Bopal Ranchhodpura Manipur, -

Merit Cum Means Scholarship for Minority Communities Sanctioned Students List - Total ( 2011-2012 ) State : Gujarat Date :16/11/2013
Merit Cum Means Scholarship for Minority Communities Sanctioned Students List - Total ( 2011-2012 ) State : Gujarat Date :16/11/2013 S.No Student Name Parent Name Institution Name Course Total Amount IV - B.E. ( Computer 1 AADIL ABDULSALAM SECAB Institute of Engineering and Technology 30000.00 Science and Eng. ) II - B.E. ( Civil 2 AADIL TAIYABBHAI GOVERNMENT ENGINEERING COLLEGE GODHARA 6645.00 Engineering ) II - M.Tech. ( Civil 3 Aadil Ghelani Parvez Ghelani CEPT University 25000.00 Engineering ) II - M.Tech. ( Civil 4 Aadil Ghelani Parvez Ghelani CEPT University 25000.00 Engineering ) III - B.Tech. ( Computer ROYAL INSTITUTE OF TECHNOLOGY AND SCIENCE. 5 AAKIB JAVIDBHAI Science and Eng. ) 30000.00 CHEVELLA IV - B.Tech. ( Computer ROYAL INSTITUTE OF TECHNOLOGY AND SCIENCE. 6 AAKIB JAVIDBHAI Science and Eng. ) 30000.00 CHEVELLA I - B.Tech. ( Information AAKIB ABDULRAZAK Nirma Institute of Technology Sarkhej Gandhinagar 7 Abdulrazak Mansuri Technology ) 30000.00 MANSURI Highway Ahemdabad II - B.Tech. ( Information AAKIB ABDULRAZAK Nirma Institute of Technology Sarkhej Gandhinagar 8 Abdulrazak Mansuri Technology ) 30000.00 MANSURI Highway Ahemdabad Sarvajanik College of Engineering & II - B.E. ( Information Merit9 Aaliyabanu CumAbdul Hafiz Means Scholarship25000.00 Technology(SFI),SURAT. Technology ) Sarvajanik College of Engineering & III - B.E. ( Information 10 Aaliyabanu Abdul Hafiz 25000.00 Technology(SFI),SURAT. Technology ) MOHAMED SHABBIR C.N.Kothari Homeopathic Medical College Research 11 AAMENA II - BHMS ( BHMS ) 25000.00 BHESANIYA Center IV - B.E. ( Electrical 12 AAMIR MAHEMUDBHAI MERCHANT ENGG. COLLEGE BASNA. VISNAGAR S 25000.00 Engineering ) Aamir imtiyazbhai mansuri II - B.E. ( Mechanical 13 Imtiyazbhai ALPHA COLLEGE OF ENGG. TECH. KHATRAJ 25000.00 Engineering ) KALOL Aamir imtiyazbhai mansuri III - B.E. -

The Gujarat Government Gazette SUPPLEMENT to the CENTRAL GAZETTE and CENTRAL SECTION PUBLISHED by AUTHORITY
© The Gujarat Government Gazette SUPPLEMENT TO THE CENTRAL GAZETTE AND CENTRAL SECTION PUBLISHED BY AUTHORITY VOL. LIX ] THURSDAY, 07th JUNE, 2018/JYAISTHA 17, 1940 [ Issue No. 23 PART-II Miscellaneous notices and advertiseMents No Legal Responsibility Is Accepted For The Publication of Advertisement Regarding Change Of Name In Gazette Of Gujarat Persons Notifying The Changes Will Remain Solely Responsible For The Legal Consequences And Also For Any Other Misrepresentation Etc. No. OLD NAME/SURNAME NEW NAME/SURNAME 1 Indradevi Ganpatlal Bhandari Indradevi Ganpatlal Jain A-701, Rameshwaram Palace, Canal Road, Vesu, Surat-395007. 2 Singha Jayaben Shanabhai Sindha Jadaben Shanabhai E-78, GSECL Shaktinagar Colony, Nr. Power House, Utran, Surat-394105. 3 Solanki Kokilaben Girishbhai Solanki Kajalben Girishbhai 624, Mandir Faliya, Harijanvas, Mota Varachha, Surat-394101. 4 Miss Swati Bhagwandas Lalwani Mrs. Amaya Gaurav Wadhwani B-102, Flamingo Residency, Nr. Sarsana Check Post, Bhimrad, Canal Road, Surat-395017. 5 Javerbhai Dhanjibhai Patel Zaverbhai Dhanjibhai Shingala 35, Nijanand Society, Nr. Khodiyarnagar, A.K. Road, Varachha, Surat-395006. 6 Divyaben Ashokbhai Modi Chandaben Ashokbhai Modi 98, Third Floor, Bhaktinagar Society-2, Nr. Jalkranti Medan, Hirabaug, Mota Varachha, Surat-395006. 7 Patil Jyoti Premnath Kate Jyoti Premnath 194, 1st Floor, Mahadevnagar-3, Opp. Maharana Pratap Bridge, BRTS Bus Stand, Dindoli, Surat-394210. 8 Miss Prajapati Meghnaben Somabhai Mrs. Sharma Meghnaben Sumit B-204, Sagini Gardenia, Opp. Krishna Park Row House, Landmark, Subhash Garden, Jahangirabad, Dandi Road, Surat-395005. 9 Vinodbhai Babubhai Patel Vinodbhai Babubhai Limbasiya A-29, Sarita Society, Nr. Ankur School, Amba Talavadi, Katargam, Surat-395004. 10 Dhameliya Jagadishbhai Bharatbhai Dhameliya Jagdishbhai Bharatbhai C/o. -

Notice Inviting On-Line Tender
TENDER NOTICE Tender No. 76 Tender is invited for the Civil work at AMC Dental College & Hospital of AMC Medical Education Trust, Ahmedabad. Department Name AMC MEDICAL EDUCATIION TRUST Circle/Division AMC DENTAL COLLEGE & HOSPITAL IFB No / Tender Notice No. Tender No.76 / e-Tender Notice No. 76 / 2019-20 (AMC MET) PROVIDING AND LAYING CHINA MOSAIC FLOORING Name of Project AND NECESSARY CIVIL WORK ON TERRACE OF THE HOSPITAL BUILDING OF AMC DENTAL COLLEGE. PROVIDING AND LAYING CHINA MOSAIC FLOORING Name of Work AND NECESSARY CIVIL WORK ON TERRACE OF THE HOSPITAL BUILDING OF AMC DENTAL COLLEGE. Estimated Contract Value (INR) Rs. 21,26,628.20 Period Of Completion(in Months) 4 Months Bidding Type Open Bid Call (Nos) 2 Tender Currency Type Single Tender Currency Settings Indian Rupee(INR) Joint Venture Not Applicable Rebate Not Applicable Eligible bidder, if interested may download the two-bid tender document from website: www.nprocure.com and www.amcdentalcollege.edu.in . Dean, AMC Dental College & Hospital, Opp. Anupam Cinema, Khokhara, Ahmedabad - 380008. Ph. (079) 22934301, 22932501 Fax. (079) 2293 1249, E-mail: [email protected] Chairman, AMC-MET reserves the right to reject any or all tenders without assigning any reason AMC Medical Education Trust N.B. - Tender Conditions & Specifications Must Be Attached Along with The Tender. Seal and Signature of the Bidder AMC DENTAL COLLEGE & HOSPITAL Page 1 AMC MEDICAL EDUCATION TRUST AMC DENTAL COLLEGE & HOSPITAL TENDER NO: - 76 TENDER DOCUMENT Volume -I General Conditions & Technical Specification Volume -II Price Bid Dean, AMC Dental College & Hospital, Opp. Anupam Cinema, Khokhara, Ahmedabad - 380008. -

Dr. Ashish Sharma Lecturer, Department of Public Health Dentistry, AMC Dental College & Hospital Khokhara, Ahmedabad Alumni IIPHG 02
IIPHG CONTRIBUTIONTO THECOMMUNITY DURINGTHIS PANDEMICCOVID-19 Report by Dr. Ashish Sharma Lecturer, Department of Public Health Dentistry, AMC Dental College & Hospital Khokhara, Ahmedabad Alumni IIPHG 02 PREFACE The interns of the AMC Dental College are the actual front line corona warriors of these two Covid 19 field projects. IIPHG is proud to have alumni such as Dr.Ashish Sharma, who have been pivotal part of the surveillance team of these two eminent projects in red zone areas of Ahmedabad city for Corona virus infection implemented by the interns of the AMC Dental College to serve the community despite the situation of COVID-19 pandemic. Dr.Ashish is presently working as Lecturer in Department of Public Health Dentistry at AMC Dental College and Hospital,Khokhara, Ahmedabad. “The sky is not the limit; the mind that sees the sky is the limit”; the interns of AMC Dental college has imitated this quote guided by the surveillance team consisiting of Dean, Dr. Dolly Patel, Dr. Ashish Sharma, Dr.Vipul Munia, Dr. Dhairya Shah and Dr. Dhawal Prajapati. They have modified their minds and capacities to work beyond their horizons of dentistry to achieve this mammoth task in a prolific manner. They have done two projects consecutively with full vigor and enthusiasm,whenever called for field duty for Covid-19 infection as mentioned below: 1.Covid-19 duty at thirteen Corona Check Posts in cluster quarantined Red Zone areas of Ahmedabad. 2.Covid 19 duty with a different challenge at twenty three wards in South, Northwest, Southwest and Central Zone of Ahmedabad. Dr. Ashish has also worked at Control Room for G-17 OPD of AMC at Covid 19 Civil Hospital, Ahmedabad for period of nine days from 19 July to 27 July 2020. -

Addor Aspire
https://www.propertywala.com/addor-aspire-ahmedabad Addor Aspire - Ambavadi, Ahmedabad Commercial and Official space available at Addor Aspire Addor Realty presents Addor Aspire with Commercial and Official space available at Ambawadi, Ahmedabad Project ID : J119008201 Builder: Addor Realty Properties: Showrooms, Office Spaces Location: Addor Aspire, Ambavadi, Ahmedabad (Gujarat) Completion Date: Dec, 2015 Status: Started Description Grab The Best Location Advantage!Business Require A Specific Location &That's What We Offer!We proudly announce Addor Aspire,an absolute prime commercial building located within Ahmedabad's premier retail precinct to meet the needs of 21st Century Professionals, Corporate & Business Owners. Features: A brilliant combination of space, location, and amenities-Addor Aspire will set new standards in life. 13 Floor + Ground with two level of basement and surface parking Total Built up area is 1,80,000/sq.ft. Ground floor ht: 14 feet First Floor ht: 12 feet 2nd to 13th floors are devoted for offices with ht of 10 feet. Amenities Ground + 2 level Parking Well Designed Entrance Lobby Decorative Foyer Area All common areas covered with CCTV Vitrified Tiles in Offices and Showrooms Superior Class Electrical Accessories with fire guard cables 24 hour Security & water supply Provision for Concealed Telephone, DTH & Broadband lines in each office Ultra modern elevation Showroom & offices height 10 ft Founded as "Satva realty" about four years back by the visionary Mr Vikas Shah, and now making a global presence as Addor Realty, we are a dedicated company working towards our main mission "Delivering more than Promised". Ardor Realty was established with an aim to nurture creativity and focus on development through innovation. -

Our Institute
Our institute The AMC Dental College & Hospital is spread in sprawling 6 acre of land in Khokhra; Located in the heart of the vibrant Ahmedabad city. The foundation of this Institute was laid by present Honourable Prime Minister SHRI NARENDRA MODI on February 2009 and hospital building was inaugurated on June 2011. AMC Dental College & Hospital is recognized by Dental council of India and is affiliated to Gujarat University. The college has recognised under-graduate (BDS) program with total intake capacity of 100 admissions annually. BDS has curriculum spanning over 4 years plus compulsory 1-year rotating internship. This college also has recognised post-graduate (MDS) program in five clinical branches with total intake capacity of 15 admissions annually. MDS program is of 3 years during which student must undertake and perform many academic, clinical and research activities. Though being centrally located in a mega city like Ahmedabad; Institute boasts of having one of the largest campus exclusively for Dental college with extraordinary infrastructure. The institute has been planned with such a care keeping student at mind that it has two separate buildings for college and hospital. College building entirely dedicated to academics with multiple lecture rooms, library, examination hall (capacity of 300) and a lavish auditorium (capacity to seat more than 400). Hospital boasts of having state of the art dental equipment and most importantly enormous amount of patient flow which is necessary for providing unparallel patient exposure and experience in student life. In-campus hostel facility for the students is also available. Separate boys and Girls 6 storeyed hostels are situated within campus with hostel mess.