Draft Outline
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
BUD2-21-Report-On-Th
PARLIAMENT OF UGANDA THE REPORT OF THE COMMITTEE ON BUDGET ON THE APPROPRIATION BILL 2021 OFFICE OF THE CTERK TO PARIIAMENT PARTIAMENT BUILDINGS KAMPAI.A. UGANDA =') Moy 2021 (.., THE REPORT OF THE COMMITTEE ON BUDGET ON THE APPROPRIATION BItL 2O2I I.O INTRODUCTION Rt. Hon. Speoker ond Hon. Members, on lsrApril 2021 the Appropnotion Brll 202lwos reod for lhe first time ond subsequently referred to the Committee on Budgel for considerotion. ln occordonce with rule 170(3) (c), the commiltee considered the Bill ond reports os follows; I.'I MEIHODOLOGY The Commrltee held consullolive meetrngs with the Minrster of Frnonce, Plonning ond Economic Development; ond exomined the Appropriotion Brll to oscertoin lhe consistency ond occurocy of the estimotes os indicoted in the Schedule to the Appropriotion Bill ogoinst ihe Resolution by Porlioment on the some. 1,2 OBJECT OF THE BITL The object of the Bill is to provide for; o) lhe outhorizotron of public expendilure oui of the Consolidoled Fund of o sum of twenty-seven lrillion, six hundred twenty billion, seven hundred ninely six million, lhree hundred sixty lhree lhousond shillings only; ond b) wilhdrowol of Funds from ihe Petroleum Fund into the Consolidoled Fund o sum of two hundred billion shillings only, to meet expendilure for the Finonciol Yeor 2021 /2022 ond to oppropriote the supplies gronted. 2.OLEGAL FRAMEWORK ,l55 2.1 Arlicle ( l ) provides thot; "fhe heods of expendilure confoined in ,he esfimoles, other lhon expendilure chatged on lhe Consolidoted Fund by lhis Conslilulion or ony Act of Porliomenf, sholl be included in o bill lo be known os on Appropriotion Bill which sholl be inlroduced into Porlioment to provide for fhe issue from the Consolidofed Fund of lhe sums necessory meel lhal expenditure ond the oppropriotion of lhose sums for lhe purposes speclfled in the bill." J 2 u 2.2 Additionolly under S. -

The Electoral Commission
THE REPUBLIC OF UGANDA THE ELECTORAL COMMISSION Telephone: +256-41-337500/337508-11 Plot 55 Jinja Road Fax: +256-31-262207/41-337595/6 P. O. Box 22678 Kampala, Uganda E-mail: [email protected] Website: www.ec.or.ug th Ref: ………………………………………Adm72/01 Date: ....9 ......................................... July 2019 Press Statement Programme for Elections of Interim Chairpersons in the Seven Newly-created Districts The Electoral Commission informs the general public that the following seven (7) newly- created districts came into effect on 1st July 2019: 1. Madi-Okollo District, which has been created out of Arua District; 2. Karenga District, which has been created out of Kaabong District; 3. Kalaki District, which has been created out of Kaberamaido District; 4. Kitagwenda District, which has been created out of Kamwenge District; 5. Kazo District, which has been created out of Kiruhura District; 6. Rwampara District, which has been created out of Mbarara District; and, 7. Obongi District, which has been created out of Moyo District. Accordingly, the Electoral Commission has appointed Thursday, 25th July, 2019 as the polling day for Elections of Interim District Chairperson in the above seven newly- created districts. Voting shall be by Electoral College and secret ballot and will be conducted at the headquarters of the respective new district, starting at 9:00am. The Electoral College shall comprise District Directly Elected Councillors and District Women Councillors representing the electoral areas forming the new districts. Please note that the elections of District Woman Representative to Parliament in the above newly-created districts will be conducted in due course. -

The Contents of the Different Baskets Are Listed Below
MINISTRY OF HEALTH PHARMACY DEPARTMENT JUNE 2020 FACILITY TRACER MEDICINES STOCK STATUS REPORT A Publication of the Ministry of Health Uganda This monthly report on the facility stock status of the 41 tracer items (in different baskets) provides information about the stock situation of health facilities in the country in order to inform the Ministry of Health and all stakeholders to make appropriate logistics decisions that ensure an effective health commodities supply chain. The report shows the number and percentages of facilities that are appropriately stocked, over stocked or out of stock by level of care and ownership based on Months of Stock (MOS). The MOS highlights the number of months a product will last based on the present consumption rate. It also further indicates facilities that have over 8 months of stock (MOS) broken down by level of care and ownership. The report shows the availability of the different and overall baskets using two indicators i.e. 1) Average percentage availability of a basket of 41 commodities based on all reporting facilities in the previous cycle Definition : Availability is measured as the number of days for which a specific commodity was in stock at the facility store during the reporting period. 2) Percentage of facilities that had over 95% availability of a basket of commodities in the previous cycle Definition : This indicator measures the % of health facilities that reported having the basket of commodities available during the reporting period. The contents of the different baskets are listed -

Message from DGF Welcome to Yet Another Issue of the Special Newsletter on Our Implementing Partners’ Response to Governance Issues Related to the COVID-19 Outbreak
Message from DGF Welcome to yet another issue of the special newsletter on our implementing partners’ response to governance issues related to the COVID-19 outbreak. In this issue, we continue to share with you the various interventions and innovations our partners are pursuing to strengthen governance in Uganda, amidst the outbreak of corona virus. SPECIAL NEWSLETTER ON DGF IMPLEMENTING PARTNERS’ In responding to the challenges caused RESPONSE TO COVID-19, ISSUE 3, JULY 2020 by COVID-19 related restriction on their programme operations, many of our partners have adopted new Women Organisations Caution the Electoral Commission on approaches to their programming in order to adhere to the Ministry of Using Media as the Only Campaign Platform for 2021 Elections Health guidelines on COVID-19. forthcoming campaigns because they lead to huge congregations and physical contacts For example, some of our partners have opted for online technologies known for spreading the COVID-19. and various media channels to engage with their beneficiaries on issues At the press conference, UWONET such as prevention of COVID-19; noted that whereas they appreciate the accountability for COVID-19 resources; gender-based violence; leadership creativity of the EC in organising a scientific and governance; access to service election given the unprecedented times delivery; and citizens’ rights, roles and Representatives of women organisatons address of COVID-19, they are concerned that responsibilities, among others. journalists at a Press Conference in Kampala. ‘digitalising elections’ might combine with (Source: UWONET) pre-existing inequalities to undermine We appreciate our partners for the commendable work they are doing omen organisations through their women, youth and rural populations from even during these uncertain times network, the Uganda Women’s participating in the forthcoming election, to ensure continuation of their WNetwork (UWONET), held a press both as voters and candidates. -

Annual Crime Report 2020
P ANDA OLIC THE UGANDAUG POLICEE PR E th OTE RV 4 Draft AnnualCT &CrimeSE Report 2020 Annual06th AprilCrime, 2021 Report 2020 Mandate The Uganda Police Force draws its mandate from the constitution of Uganda Chapter Twelve, Article 212 that stipulates the functions of the force as: (a) to protect life and property; (b) to preserve law and order; (c) to prevent and detect crime; and - (d) to cooperate with the civilian authority and other security organs estab lished under this Constitution and with the population generally. Vision “An Enlightened, Motivated, Community Oriented, Accountable and Modern Police Force; geared towards a Crime free society”. Mission - “To secure life and property in a committed and Professional manner, in part nership with the public, in order to promote development ADMINISTRATIVE AND PLANNING MACRO STRUCTURE FOR THE UGANDA POLICE FORCE The Inspector General Police Authority of Police The Deputy Inspector General of Police Directorate of Police Fire Directorate of Human Rights Directorate of Traffic & Road Directorate of Opera�ons Preven�on and Rescue and Legal Services Safety Services Directorate of ICT Directorate of Counter Directorate of Police Health Directorate of INTERPOL and Terrorism Services Interna�onal Rela�ons Directorate of Poli�cal Directorate of Criminal Directorate of Logis�cs and Directorate of Police Welfare Inves�ga�ons Commissariat Engineering Directorate of Research, Directorate of HRA Directorate of Forensic Directorate of Parliamentary Planning and Development Services Police Directorate of Crime Directorate of HRD Field Force Unit Kampala Metropolitan Police Intelligence Police Force Professional Department Department Police Senior Police Inspectorate Department Department Department Press Unit Standards of Flying of Physical Command Academy Dep artment of Finance of Protocol, of Police and Office Honours & Women Unit Squad Fitness College and Command Support Ceremonies Affairs Services ii P ANDA OLIC UG E PR E OTE RV CT & SE JM Okoth Ochola (Esq) Inspector General of Police Maj. -
The Ifms Journey 2003 - 2020
MINISTRY OF FINANCE PLANNING AND ECONOMIC DEVELOPMENT ACCOUNTANT GENERAL’S OFFICE THE IFMS JOURNEY 2003 - 2020 Document Control Version Author / Updated Reviewed by Reviewed by Date 1.0 Rogers Baguma Aiden Rujumba - April 2020 Commissioner, FMSD 1.1 Rogers Baguma Aiden Rujumba Godfrey Ssemugooma May 2020 Commissioner, FMSD Director, FMSD 1.2 Rogers Baguma Aiden Rujumba Godfrey Ssemugooma June 2020 Commissioner, FMSD Director, FMSD Contents 1 INTRODUCTION ................................................................................. 9 1.1 IFMS .................................................................................................................................... 9 1.1.1 The Integrated Financial Management System ..................................................................................................... 9 2 IFMS OPERATION ............................................................................. 11 2.1 IFMS MODULES ............................................................................................................... 11 2.2 IFMS DATA LINKS ........................................................................................................... 11 3 BRINGING UP AN IFMS SITE ........................................................... 13 3.1 PRE-REQUISITES FOR IFMS ............................................................................................ 13 3.1.1 Infrastructure Readiness ........................................................................................................................................ -
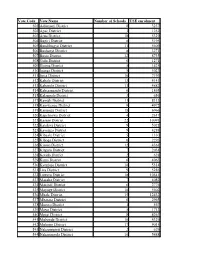
Vote Code Vote Name Number of Schools USE Enrolment 501
Vote Code Vote Name Number of Schools USE enrolment 501 Adjumani District 8 3237 502 Apac District 3 1252 503 Arua District 18 5329 504 Bugiri District 8 5195 505 Bundibugyo District 11 5609 506 Bushenyi District 8 3271 507 Busia District 12 8735 508 Gulu District 6 1271 509 Hoima District 5 1425 510 Iganga District 5 5023 511 Jinja District 10 7193 512 Kabale District 13 4143 513 Kabarole District 11 4882 514 Kaberamaido District 6 1865 515 Kalangala District 3 656 517 Kamuli District 11 8313 518 Kamwenge District 9 4972 519 Kanungu District 18 6966 520 Kapchorwa District 4 2617 521 Kasese District 22 10091 522 Katakwi District 9 5021 523 Kayunga District 9 4288 524 Kibaale District 5 1330 525 Kiboga District 6 2293 526 Kisoro District 12 4361 527 Kitgum District 7 2034 528 Kotido District 2 628 529 Kumi District 6 4063 530 Kyenjojo District 10 5314 531 Lira District 9 5286 532 Luwero District 18 10541 533 Masaka District 7 4082 534 Masindi District 6 2776 535 Mayuge District 10 5602 536 Mbale District 15 12432 537 Mbarara District 6 2965 538 Moroto District 1 567 539 Moyo District 5 1713 540 Mpigi District 8 4263 541 Mubende District 10 4329 542 Mukono District 17 9015 543 Nakapiripirit District 2 629 544 Nakasongola District 10 5488 545 Nebbi District 5 2257 546 Ntungamo District 18 8412 547 Pader District 8 2856 548 Pallisa District 8 6661 549 Rakai District 14 7586 550 Rukungiri District 21 11111 551 Sembabule District 8 4162 552 Sironko District 10 5552 553 Soroti District 5 3421 554 Tororo District 17 13341 555 Wakiso District 14 -

Guidelines 2020-21 (1).Pdf
THE REPUBLIC OF UGANDA MINISTRY OF HEALTH Sector Grant and Budget Guidelines to Local Governments FY 2020/21 i FOREWORD These guidelines are issued by the Ministry of Health to Local Governments to provide information about the sector conditional grants and to guide on utilization and accountability of these grants during the Financial Year 2020/21. The guidelines are tools to prepare accurate work plans and budget estimates for health service delivery in each District Local Government. The guidelines consist of; National Policies for the sector, an overview of Central Government Grants to Local Governments, the role and mandate of Local Governments in the sector, an explanation of how these are allocated to each Local Government, and budget requirements. The sector continues to implement policies that are aligned to H.E the President’s 23 Strategic Guidelines and Directives that will deliver a minimum development package for every Ugandan in order to attain the middle income status by 2020. During FY 2020/21 the sector continues to re-prioritize Health Promotion, Disease Prevention, hygiene and Sanitation and 30% of Non-wage Recurrent has been earmarked to undertake activities related to these priority areas across the spectrum. Thirty percent (30%) of the Non- Wage Recurrent at each level, i.e. Local Government Health Office, District Hospital and each Facility shall be used for this purpose. It will be at the discretion of the Local Government to appropriately agree on the percentage based on the need and performance in these priority areas. The sector grants to Local Governments are divided into seven categories: namely; the Conditional Wage Grant, Conditional Non-Wage Grant, The Transitional Development Sanitation Grant, the Transitional Development Ad Hoc Grant, Result Based Financing (RBF), GFTAM and GAVI HSS2 subventions. -
Health Sub Programme Grant, Budget and Implementation Guidelines for Local Governments
THE REPUBLIC OF UGANDA MINISTRY OF HEALTH Health Sub Programme Grant, Budget and Implementation Guidelines for Local Governments FINANCIAL YEAR 2021/22 Foreword These guidelines are issued by the Ministry of Health to Local Governments to provide them with information that is used during budgeting and implementation. Where necessary, there are cross-references to other guidelines and policies which provide more details. The Health Sub Programme grants to Local Governments are divided into six categories: namely, the Conditional Wage Grant, Conditional Non-Wage Grant, the Transitional Development Ad Hoc Grant, Result Based Financing (RBF), Global Fund for Tuberculosis, HIV/AIDS, and Malaria (GFTAM) and The Global Alliance for Vaccines and Immunization (GAVI) Health Systems Strengthening (HSS2) subventions. Local Governments are required to provide timely accountabilities for these grants. During FY 2021/22 the Health Sub Programme will continue to re-prioritize Health Promotion, Disease Prevention, hygiene, and Sanitation and 30% of Non-Wage Recurrent has been earmarked to undertake activities related to these priority areas across the spectrum i.e., Local Government Health Office, District Hospital and each health facility. Lastly, allow me to re-echo my appeal that during FY 2021/22 we all refocus on activities associated with immediate reduction of incidence of communicable and non-communicable disease including public health emergencies like the COVID-19 pandemic, and improving and sustaining high coverage of health care services to reduce the cost of health care in localities using a multisectoral approach. I therefore call upon all Local Government Accounting Officers to ensure that the Health Sector detailed work plans, and estimates are finalized and implemented on time in line with these Health Sub-Programme Grant and Budget Guidelines. -

IG Report to Parliament July
THE REPUBLIC OF UGANDA BI- ANNUAL INSPECTORATE OF GOVERNMENT PERFORMANCE REPORT TO PARLIAMENT JULY – DECEMBER 2020 BI- ANNUAL INSPECTORATE OF VISION MISSION GOVERNMENT PERFORMANCE REPORT A just and corruption TO PARLIAMENT free Uganda. To promote good governance through prevention of corruption, enforcement of the law and citizens’ MANDATE engagement. Promoting just Utilization of Public Resources. CUSTOMER VALUE VALUES PROPOSITION 1. Integrity IG Undertakes to promote distributive 2. Professionalism justice and 3. Teamwork Administrative justice 4. Innovativesness to all People 5. Impartiality JULY – DECEMBER 2020 6. Gender Equality & Equity BI- ANNUAL INSPECTORATE OF VISION MISSION GOVERNMENT PERFORMANCE REPORT A just and corruption TO PARLIAMENT free Uganda. To promote good governance through prevention of corruption, enforcement of the law and citizens’ MANDATE engagement. Promoting just Utilization of Public Resources. CUSTOMER VALUE VALUES PROPOSITION 1. Integrity IG Undertakes to promote distributive 2. Professionalism justice and 3. Teamwork Administrative justice 4. Innovativesness to all People 5. Impartiality JULY – DECEMBER 2020 6. Gender Equality & Equity THE INSPECTORATE OF DIRECTORATES GOVERNMENT Directorate of Finance and Administration Jubilee Insurance Centre, Secretary to the Inspectorate of Government Plot 14, Parliament Avenue Ms. Rose N. Kafeero P.O. Box 1682 Kampala, Uganda Tel: 0414-359788/0414-236038 General Lines: Fax: 0414-257590 0414- 255892/259738/310000/344219 Email: [email protected] Hotlines: 0414-347387/0312-101346 Directorate of Research, Education Fax: 0414-344810 and Advocacy [email protected] Email: Director: Mr. Okiror Stephen Website: www.igg.go.ug Tel: 0414-348613 Facebook: Inspectorate of Government Email: [email protected] Twitter: @IGGUganda YouTube: Inspectorate of Government Directorate of Leadership Code Director: Ms Annet Twine Tel: 0414-251526 Email: [email protected] OFFICE OF THE INSPECTOR GENERAL OF GOVERNMENT Directorate of Legal Affairs Director: Ms. -

Facility Tracer Medicines Stock Status Report As Of
MINISTRY OF HEALTH PHARMACY DEPARTMENT APRIL 2020 FACILITY TRACER MEDICINES STOCK STATUS REPORT A Publication of the Ministry of Health Uganda This monthly report on the facility stock status of the 41 tracer items (in different baskets) provides information about the stock situation of health facilities in the country in order to inform the Ministry of Health and all stakeholders to make appropriate logistics decisions that ensure an effective health commodities supply chain. The report shows the number and percentages of facilities that are appropriately stocked, over stocked or out of stock by level of care and ownership based on Months of Stock (MOS). The MOS highlights the number of months a product will last based on the present consumption rate. It also further indicates facilities that have over 8 months of stock (MOS) broken down by level of care and ownership. The report shows the availability of the different and overall baskets using two indicators i.e. 1) Average percentage availability of a basket of 41 commodities based on all reporting facilities in the previous cycle Definition : Availability is measured as the number of days for which a specific commodity was in stock at the facility store during the reporting period. 2) Percentage of facilities that had over 95% availability of a basket of commodities in the previous cycle Definition : This indicator measures the % of health facilities that reported having the basket of commodities available during the reporting period. The contents of the different baskets are listed -

UWEP) Ministry of Gender, Labour and Social Development Simbamanyo House, Plot 2, George Street
BUSINESS & TENDERS UGANDA WOMEN ENTREPRENEURSHIP PROGRAMME (UWEP) Ministry of Gender, Labour and Social Development Simbamanyo House, Plot 2, George Street. P.O Box 7136, Kampala Tel: 041-4 343572/ 0414 699219/ 0414 699220, Facebook: @uwep.mglsd ON THE OCCASION TO MARK THE International Women’s Day, 2021 H.E. Yoweri Kaguta Museveni HON. Frank K. Tumwebaze HON. Mutuuzo Peace Regis Aggrey David Kibenge Winifred Komuhangi Masiko THE PRESIDENT OF THE MINISTER OF GENDER, LABOUR MINISTER OF STATE FOR PERMANENT SECRETARY National Programme REPUBLIC OF UGANDA AND SOCIAL DEVELOPMENT GENDER AND CULTURE Coordinator - UWEP Programme Background: h) The group approach has given Women an opportunity to improve Over the years, majority of women in Uganda have been disenfranchised knowledge and skill through mentoring each other. The greater from the formal business sector due to limited access to affordable involvement of the Women in mobilization, sensitization, prioritization credit, limited technical knowledge on business entrepreneurship and and planning for their needs, implementation and monitoring and management, limited access to markets as well as information regarding evaluation of Programme activities has created a sense of business opportunities. To address that problem, Government of Uganda empowerment and confidence to take charge of their destiny. in the FY 2015/2016 initiated the Uganda Women Entrepreneurship Programme (UWEP) with a core goal of empowering Ugandan women to improve their income levels and their contribution to economic