Lethargic Encephalitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
New Highpark and St Cuthbert's Primary Schools, Westercommon
Pre-12 Education Strategy Phase 4B– New Highpark and St Cuthbert’s Primary Schools, Westercommon Early Years Centre and Highpark Autistic Unit – Award of contract approved – Declaration of interest. 13 There was submitted a report by the Executive Director of Development and Regeneration Services regarding the tender received for Phase 4B of the pre-12 Education Strategy for New Highpark and St Cuthbert’s Primary Schools, Westercommon Early Years Centre and Highpark Autistic Unit, advising (1) that during the design and planning application process for the construction of a new multiplex primary school with early years facilities and autistic unit to replace the existing provision at Ruchill, Westercommon and Our Lady of the Assumption and St Cuthbert’s Primary Schools, Westercommon Nursery School and Ruchill Autistic Centre to be built in an area of Ruchill Park with access to the east through the disused Ruchill Hospital, it had become clear that the proposed access road would not be developed as part of the proposed residential development of the adjacent Ruchill Hospital site as was originally envisaged as the preferred developers appointed by Scottish Enterprise had withdrawn from the development; (2) that it had been necessary to procure the access road under a license agreement with Scottish Enterprise and Development and Regeneration Services had undertaken the design of the access road to tie in with the tender programme for the school and the procurement requirements and negotiations were underway with Scottish Enterprise to secure a 50% contribution; (3) that ABC had been requested to procure the works for the contract by producing traditional tender documentation and seeking a tender return from City Building (Glasgow) LLP; (4) of the tender process; and (5) that following a devised set of criteria by Development and Regeneration Services, it had been determined that the tender from City Building (Glasgow) LLP represented Best Value to the Council. -

Mental Health Services North East Sector Annual Report 2003/04
NorthEast Sector Annual Report 2003 – 2004 The new Arran Centre The new Easterhouse Community Health Centre – incorporating Auchinlea Resource Centre and the previous Health Centre 1 Section 1 EXECUTIVE SUMMARY The last year within the North East sector has been another period of significant activity. In comparing the prospective developments from last year’s report, much has been achieved and this introduction will cover some of these achievements later on. Firstly though it is worth recalling that the driver for the production of Annual Reports came from what was then the Divisional Clinical Governance Committee. The North East Sector received very positive feedback when the sector report was presented to the committee last year and also by written feedback in the form of a standard evaluation report. Looking back over the past year and the targets that were set then, the following key milestones have been achieved: • Wyndford Lock Nursing Home has been closed and patients have been accommodated in alternative forms of accommodation. All staff have been redeployed to alternative posts. • A new North East addiction Unit is about to open at Stobhill which will mean that Ruchill Hospital will at last benefit from improved patient activity space and staff will have some changing facilities. It will also result in a reduction of admission beds in each ward from 30 to 24, creating much needed patient activity space at Parkhead. • A new North East IPCU will open within the next few weeks at Stobhill which will have dedicated Consultant and Staff Grade Psychiatrist cover. This will also increase the amount of much patient activity space at Parkhead Hospital. -

Glasgow City Community Health Partnership Service Directory 2014 Content Page
Glasgow City Community Health Partnership Service Directory 2014 Content Page About the CHP 1 Glasgow City CHP Headquarters 2 North East Sector 3 North West Sector 4 South Sector 5 Adult Protection 6 Child Protection 6 Emergency and Out-of-Hours care 6 Addictions 7 - 9 Asylum Seekers 9 Breast Screening 9 Breastfeeding 9 Carers 10 - 12 Children and Families 13 - 14 Dental and Oral Health 15 Diabetes 16 Dietetics 17 Domestic Abuse / Violence 18 Employability 19 - 20 Equality 20 Healthy Living 21 Health Centres 22 - 23 Hospitals 24 - 25 Housing and Homelessness 26 - 27 Learning Disabilities 28 - 29 Mental Health 30 - 40 Money Advice 41 Nursing 41 Physiotherapy 42 Podiatry 42 Respiratory 42 Rehabilitation Services 43 Sexual Health 44 Rape and Sexual Assault 45 Stop Smoking 45 Transport 46 Volunteering 46 Young People 47-49 Public Partnership Forum 50 Comments and Complaints 51-21 About Glasgow City Community Health Partnership Glasgow City Community Health Partnership (GCCHP) was established in November 2010 and provides a wide range of community based health services delivered in homes, health centres, clinics and schools. These include health visiting, health improvement, district nursing, speech and language therapy, physiotherapy, podiatry, nutrition and dietetic services, mental health, addictions and learning disability services. As well as this, we host a range of specialist services including: Specialist Children’s Services, Homeless Services and The Sandyford. We are part of NHS Greater Glasgow & Clyde and provide services for 584,000 people - the entire population living within the area defined by the LocalAuthority boundary of Glasgow City Council. Within our boundary, we have: 154 GP practices 136 dental practices 186 pharmacies 85 optometry practices (opticians) The CHP has more than 3,000 staff working for it and is split into three sectors which are aligned to local social work and community planning boundaries. -
Updated Timetable
329 UPDATED TIMETABLE FROM 24th THIS JUNE 2018 SERVICE ACCEPTS CONTACTLESS PAYMENT GLASGOW CITY CENTRE THIS SERVICE IS OPERATED BY ROYSTON McGILL’S ON SPRINGBURN SHOPPING BEHALF OF SPT CENTRE STOBHILL HOSPITAL H www.mcgillsbuses.co.uk @Buses_McGills /McGillsBuses1 Glasgow - Stobhill Hospital H via Royston and Springburn 329 1 MONDAY – FRIDAY from 25 June 2018 Service No. 329 329 329 329 329 329 329 329 329 329 329 329 329 SPEED UP YOUR Glasgow, West Nile Street 06.11 07.11 08.11 09.11 10.11 11.11 12.11 13.11 14.11 15.11 16.11 17.11 18.11 Roystonhill 06.22 07.22 08.22 09.22 10.22 11.22 12.22 13.22 14.22 15.22 16.22 17.22 18.22 Springburn Shopping Centre 06.33 07.33 08.33 09.33 10.33 11.33 12.33 13.33 14.33 15.33 16.33 17.33 18.33 Stobhill Hospital H 06.39 07.39 08.39 09.39 10.39 11.39 12.39 13.39 14.39 15.39 16.39 17.39 18.39 JOURNEY WITH MONDAY – FRIDAY from 25 June 2018 FASTER WAYS TO PAY Service No. 329 329 329 329 329 329 329 329 329 329 329 329 Stobhill Hospital H 06.43 07.43 08.43 09.43 10.43 11.43 12.43 13.43 14.43 15.43 16.43 17.43 GOCONTACTLESS Springburn Shopping Centre 06.49 07.49 08.49 09.49 10.49 11.49 12.49 13.49 14.49 15.49 16.49 17.49 Use your contactless Roystonhill 07.00 08.00 09.00 10.00 11.00 12.00 13.00 14.00 15.00 16.00 17.00 18.00 device or card. -

Glasgow City Health and Social Care Partnership Health Contacts
Glasgow City Health and Social Care Partnership Health Contacts January 2017 Contents Glasgow City Community Health and Care Centre page 1 North East Locality 2 North West Locality 3 South Locality 4 Adult Protection 5 Child Protection 5 Emergency and Out-of-Hours care 5 Addictions 6 Asylum Seekers 9 Breast Screening 9 Breastfeeding 9 Carers 10 Children and Families 12 Continence Services 15 Dental and Oral Health 16 Dementia 18 Diabetes 19 Dietetics 20 Domestic Abuse 21 Employability 22 Equality 23 Health Improvement 23 Health Centres 25 Hospitals 29 Housing and Homelessness 33 Learning Disabilities 36 Maternity - Family Nurse Partnership 38 Mental Health 39 Psychotherapy 47 NHS Greater Glasgow and Clyde Psychological Trauma Service 47 Money Advice 49 Nursing 50 Older People 52 Occupational Therapy 52 Physiotherapy 53 Podiatry 54 Rehabilitation Services 54 Respiratory Team 55 Sexual Health 56 Rape and Sexual Assault 56 Stop Smoking 57 Volunteering 57 Young People 58 Public Partnership Forum 60 Comments and Complaints 61 Glasgow City Community Health & Care Partnership Glasgow Health and Social Care Partnership (GCHSCP), Commonwealth House, 32 Albion St, Glasgow G1 1LH. Tel: 0141 287 0499 The Management Team Chief Officer David Williams Chief Officer Finances and Resources Sharon Wearing Chief Officer Planning & Strategy & Chief Social Work Officer Susanne Miller Chief Officer Operations Alex MacKenzie Clincial Director Dr Richard Groden Nurse Director Mari Brannigan Lead Associate Medical Director (Mental Health Services) Dr Michael Smith -

Mental Health Bed Census
Scottish Government One Day Audit of Inpatient Bed Use Definitions for Data Recording VERSION 2.4 – 10.11.14 Data Collection Documentation Document Type: Guidance Notes Collections: 1. Mental Health and Learning Disability Bed Census: One Day Audit 2. Mental Health and Learning Disability Patients: Out of Scotland and Out of NHS Placements SG deadline: 30th November 2014 Coverage: Census date: Midnight, 29th Oct 2014 Page 1 – 10 Nov 2014 Scottish Government One Day Audit of Inpatient Bed Use Definitions for Data Recording VERSION 2.4 – 10.11.14 Document Details Issue History Version Status Authors Issue Date Issued To Comments / changes 1.0 Draft Moira Connolly, NHS Boards Beth Hamilton, Claire Gordon, Ellen Lynch 1.14 Draft Beth Hamilton, Ellen Lynch, John Mitchell, Moira Connolly, Claire Gordon, 2.0 Final Beth Hamilton, 19th Sept 2014 NHS Boards, Ellen Lynch, Scottish John Mitchell, Government Moira Connolly, website Claire Gordon, 2.1 Final Ellen Lynch 9th Oct 2014 NHS Boards, Further clarification included for the following data items:: Scottish Government Patient names (applicable for both censuses) website ProcXed.Net will convert to BLOCK CAPITALS, NHS Boards do not have to do this in advance. Other diagnosis (applicable for both censuses) If free text is being used then separate each health condition with a comma. Mental Health and Learning Disability Bed Census o Data item: Mental Health/Learning Disability diagnosis on admission Can use full description option or ICD10 code only option. o Data item: Last known Mental Health/Learning Disability diagnosis Can use full description option or ICD10 code only option. -
Campus Travel Guide Final 08092016 PRINT READY
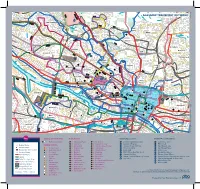
Lochfauld V Farm ersion 1.1 27 Forth and 44 Switchback Road Maryhill F C Road 6 Clyde Canal Road Balmore 1 0 GLASGOW TRANSPORT NETWORK 5 , 6 F 61 Acre0 A d Old Blairdardie oa R Drumchapel Summerston ch lo 20 til 23 High Knightswood B irkin e K F 6 a /6A r s de F 15 n R F 8 o Netherton a High d 39 43 Dawsholm 31 Possil Forth and Clyde Canal Milton Cadder Temple Gilshochill a 38 Maryhill 4 / 4 n F e d a s d /4 r a 4 a o F e River Lambhill R B d Kelvin F a Anniesland o 18 F 9 0 R 6 n /6A 1 40 r 6 u F M 30 a b g Springburn ry n h 20 i ill r R Ruchill p Kelvindale S Scotstounhill o a Balornock 41 d Possil G Jordanhill re Park C at 19 15 W es 14 te rn R 17 37 oa Old Balornock 2 d Forth and D um Kelvinside 16 Clyde b North art 11 Canal on Kelvin t Ro Firhill ad 36 ee 5 tr 1 42 Scotstoun Hamiltonhill S Cowlairs Hyndland 0 F F n e 9 Broomhill 6 F ac 0 r Maryhill Road V , a ic 6 S Pa tor Dowanhill d r ia a k D 0 F o S riv A 8 21 Petershill o e R uth 8 F 6 n F /6 G r A a u C 15 rs b R g c o u n Whiteinch a i b r 7 d e Partickhill F 4 p /4 S F a River Kelvin F 9 7 Hillhead 9 0 7 River 18 Craighall Road Port Sighthill Clyde Partick Woodside Forth and F 15 Dundas Clyde 7 Germiston 7 Woodlands Renfrew Road 10 Dob Canal F bie' 1 14 s Loa 16 n 5 River Kelvin 17 1 5 F H il 7 Pointhouse Road li 18 5 R n 1 o g 25A a t o Shieldhall F 77 Garnethill d M 15 n 1 14 M 21, 23 10 M 17 9 6 F 90 15 13 Alexandra Parade 12 0 26 Townhead 9 8 Linthouse 6 3 F Govan 33 16 29 Blyt3hswood New Town F 34, 34a Anderston © The University of Glasgo North Stobcross Street Cardonald -

New Stobhill Hospital the New Stobhill Ambulatory Care Hospital Belmont (ACH) Is Set in the Stobhill Campus
To Bishopbriggs FIF New Stobhill station E WAY New Stobhill Hospital The New Stobhill Ambulatory Care Hospital Belmont (ACH) is set in the Stobhill campus. The campus Hospital D Centre A O houses the hospital, a minor injuries unit, a R L L Marie Curie number of general and specialist mental health Walking and cycling guide 2021 HI Hospice Y facilities, and a brand new purpose-built Marie RA G Curie Cancer Care hospice. L BA A LORNOCK ROAD B The ACH provides outpatient clinics, day surgery and diagnostic services. There are hospital beds available to medics to extend the range of short B ALORNOCK ROAD stay surgical procedures offered to patients. B A L Skye House O At the main entrance there is a staffed help desk R N O and patient information points which provide C K R travel information, health promotion and other O A D advice. BELMONT ROAD Stobhill Hospital 2 new mental health wards are now on the campus. The two wards – Elgin and Appin – have space for up to 40 inpatients, with Elgin To Springburn dedicated to adult acute mental health inpatient station care and Appin focusing on older adults with functional mental health issues. Cycle Parking Entrance Rowanbank Bus stop Clinic BALORNOCK ROAD Active Travel Cycling to Work NHS Greater Glasgow & Clyde recognise that New Stobhill Hospital is well served by public transport The Cycle to Work scheme is a salary sacrifice scheme physical activity is essential for good health covering bus travel within the immediate area and available to NHS Greater Glasgow & Clyde staff*. -

Well Positioned Plots of Land with Planning Permission
Plot 2 WELL POSITIONED PLOTS OF LAND WITH PLANNING PERMISSION craigmore crag, carbeth g63 9at Description WELL POSITIONED PLOTS Plot 1 – Planning permission granted for detached home – Stirling OF LAND WITH PLANNING Council – 14/00124/FUL Plot 2 – Planning permission granted in principle for detached home – PERMISSION Stirling Council – 14/00602/PPP The images in this brochure are computer generated, based on the Architect's drawings & reflect the approved planning permissions. craigmore crag, carbeth g63 9at The boundary plan was created for identification purposes only and its accuracy is not guaranteed and is subject to change. Servitude rights, burdens and wayleaves Glasgow – 13 miles The property is sold subject to and with the benefit of all servitude Glasgow Airport – 16 miles rights, burdens, reservations and wayleaves, including rights of access Stirling – 27 miles and rights of way, whether public or private, light, support, drainage, water and wayleaves for masts, pylons, stays, cable, drains and Travel directions water, gas and other pipes, whether contained in the Title Deeds or From Glasgow and Bearsden Cross, take the A809 north, signed for informally constituted and whether referred to in the General Remarks Plot 1 Drymen. Stay on the A809 passing Hilton Park Golf Club on the right and Stipulations or not. The Purchaser(s) will be held to have satisfied hand side. Immediately after the Carbeth Inn, turn right onto the B821 himself as to the nature of all such servitude rights and others. (Cuilts Road) , follow the B821 and the plots are the third entrance on the right hand side. Possession Vacant possession and entry will be given on completion. -
Self Guided View Trip Dates the West Highland Way Book Now
Self Guided View Trip Dates The West Highland Way Book Now Trip Grade: Blue 6 Point to Point The West Highland Way The West Highland Way is a classic long distance walk, covering 152 kilometres (95 miles) from Milngavie on the outskirts of Glasgow, to Fort William in the Highlands. The route travels past the bonnie banks of Loch Lomond, across the atmospheric Rannoch Moor, past dramatic Glencoe and onwards to finish at the foot of Ben Nevis, Britain’s highest mountain. The West Highland Way is one of the classic treks of the world and is undertaken by many people of all ages from across the world, making it a fun and social trek. On this self- guided walk we arrange your accommodation each evening and baggage transfer, as well as providing you with detailed route notes and maps so that you get the most out of this wonderful trek. Highlights • Take on the challenge of Scotland’s most famous and one of the world’s greatest long distance trails - the West Highland Way. • Immerse yourself in the spectacular scenery as you walk through the beautiful landscapes of Loch Lomond, Rannoch Moor and Glencoe. • We will arrange all accommodation, luggage transfer and provide you with maps and comprehensive route notes. Book with confidence • You pick the dates that suit you – we make all the arrangements required. PLEASE NOTE – The itinerary may be subject to change at the discretion of the Wilderness Scotland Guide with regard to weather conditions and other factors. Planned Itinerary Day 1 | Arrive in Milngavie Day 2 | Milngavie to Drymen Day 3 | Drymen to Rowardennan Day 4 | Rowardennan to Inverarnan Day 5 | Inverarnan to Tyndrum Day 6 | Tyndrum to Glencoe* Day 7 | Glencoe to Kinlochleven Day 8 | Kinlochleven to Fort William Day 9 | Fort William and Depart Arrival Info Make your own transport arrangements to Milngavie and your first nights accommodation Departure Info From Fort William depart for home or onward travel after breakfast the day after completing the hike. -

Housing Officers
p30.qxp_Layout 1 08/12/2020 10:48 Page 1 HELPFUL INFORMATION Housing Officers Multi-Storey Flats Housing Manager: Karen Johnson Karen JohnsonBola Akintoye Catherine Mather Pamela Hutchison Terri McChesney Yvonne Kinnear Liz MacMillan Anne Sheeran For Rent Enquiries: Carron Street For Housing Elmvale Street Carbisdale Street Horne Street Bola Akintoye Enquiries: Eccles Street Memel Street Carron Crescent Terri McChesney Carbisdale Street Carron Street 1292-1330 Springburn Road 1292-1330 Springburn Road Fernbank Street Carbisdale Street Balgrayhill Road Balgrayhill Road Hickory Street Eccles Street Stobhill Road Stobhill Road Carron Place Carbisdale Street Viewpoint Gate, Place & Road Viewpoint Gate, Place & Road Fernbank Street Pamela Hutchison Catherine Mather Yvonne Kinnear Hickory Street Lenzie Terrace Galloway Street Galloway Street Carron Place Broomknowes Road 771-783 Springburn Road Lenzie Terrace Croftbank Street Anne Sheeran Blackthorn Street Carron Crescent Edgefauld Road Broomknowes Road Elmvale Street Liz MacMillan 623-700 Hawthorn Street Croftbank Street Horne Street 771-783 Springburn Road Edgefauld Road Memel Street Blackthorn Street 623-700 Hawthorn Street Possilpark Housing Manager: Sharon Hazlett Sharon HazlettAndrea Campbell Danielle Quinn Susan McAllister Alison McLean Lynn Bennett Gail Hamilton Gordon McFarlane Ashleigh McIntyre For Rent Enquiries: 313-483 Hawthorn Street For Housing Gail Hamilton Hawthorn Quadrant 8, 16, 24 Balmore Road Andrea Campbell Enquiries: Mansion Street 40, 46, 52 Balmore Road 67-101 Allander -

NBG Report for KCC Meeting 19 Apr 2017
NBG Report for KCC Meeting 19 Apr 2017 Further progress! The new fibre cabinet at the Killearn exchange is now live, accepting orders, and some residents have already got the service installed and working. Speeds are reported to be as expected at 30Mbps or more. So if you live in “The Trees”, nearby, or in the centre of the village, you should be able to get “super-fast broadband! About 50% of postcodes in the village are now connected to one of the fibre cabinets. Status of your individual connectivity can be checked on either of the WhereandWhen pages of the BT Openreach or Digital Scotland websites or in the tables at the end of this report. This site is also showing a download of the exchange roll-out list, but as this is only at exchange level, it doesn’t help very much. NOTE: Remember the Digital Scotland “Better Broadband Scheme” provides a subsidy to establish a better connection using either satellite or wireless for those currently getting download speeds of less than 2Mbps. See the KCC website for specific links. Balfron has also got more cabinets with 85% of the village now showing as “Accepting Orders”. Strathblane/Blanefield is in a similar position with slightly over 85% of the village covered. Buchlyvie has nearly 90% showing as connected while Croftamie/Drymen is showing nearly 60% Accepting Orders. All this does have to be qualified though as many premises are on long lines, and whilst they will see a significant benefit in speed (double or better), they will not achieve “super-fast” speeds.