African Programme for Onchocerciasis Control (Apoc)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Credit and Agricultural Productivity Among Farmers in Gwarzo Local Government Area of Kano State, Nigeria
CREDIT AND AGRICULTURAL PRODUCTIVITY AMONG FARMERS IN GWARZO LOCAL GOVERNMENT AREA OF KANO STATE, NIGERIA BY HAMIDAN BELLO HARRIS MEC 1165-05306-09786 A RESEARCH SUBMITITED TO THE COLLEGE OF ECONOMICS AND MANAGEMENT IN PARTIAL FULFILMENT OF THE RECUIRETMENTS FOR THE AWARD OF MASTER OF ARTS DEGREE IN ECONOMICS OF THE KAMPALA INTERNATIONAL UNIVERSITY, KAMPALA, UGANDA. JUNE, 2019 i DECLARATION I hereby declare that this thesis is my original work and the topic has never been submitted to any university or institution of higher learning for an academic award. Signature………………………… Date …………………………. HAMIDAN BELLO HARRIS i APPROVAL This research report has been submitted for examination with my supervisors consent Dr Byamukama E ………………………… ………………………… Signed Date ii DEDICATION I dedicated this work to Almighty Allah for giving me the opportunity to proceed with my academic activities up to this stage of learning. I believe many are willing to attain but could not make it because of one reason or the other. ALHAMDULILLAH ALA KULLI –HAL iii ACKNOWLEDGMENTS I wish to express my profound gratitude and happiness to Allah (SWA) for giving me the strength and wisdom to withstand the challenges of studying away from my home. Despite all the challenges, I finally made it. I wish to thank my entire family members for their courage in confronting the challenges of life during my leave of study. I wish to thank my supervisor, Dr Byamukama Eliab, for his tireless effort in ensuring that this work has become successful. Also not forgetting the tremendous effort imputed by my able lecturer, Dr Muhammad kibuuka, Prof. Emenike O. -

Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No
LICENSED MICROFINANCE BANKS (MFBs) IN NIGERIA AS AT FEBRUARY 13, 2019 S/N Name Category Address State Description 1 AACB Microfinance Bank Limited State Nnewi/ Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No. 9 Oba Akran Avenue, Ikeja Lagos State. LAGOS 3 ABC Microfinance Bank Limited Unit Mission Road, Okada, Edo State EDO 4 Abestone Microfinance Bank Ltd Unit Commerce House, Beside Government House, Oke Igbein, Abeokuta, Ogun State OGUN 5 Abia State University Microfinance Bank Limited Unit Uturu, Isuikwuato LGA, Abia State ABIA 6 Abigi Microfinance Bank Limited Unit 28, Moborode Odofin Street, Ijebu Waterside, Ogun State OGUN 7 Above Only Microfinance Bank Ltd Unit Benson Idahosa University Campus, Ugbor GRA, Benin EDO Abubakar Tafawa Balewa University Microfinance Bank 8 Limited Unit Abubakar Tafawa Balewa University (ATBU), Yelwa Road, Bauchi BAUCHI 9 Abucoop Microfinance Bank Limited State Plot 251, Millenium Builder's Plaza, Hebert Macaulay Way, Central Business District, Garki, Abuja ABUJA 10 Accion Microfinance Bank Limited National 4th Floor, Elizade Plaza, 322A, Ikorodu Road, Beside LASU Mini Campus, Anthony, Lagos LAGOS 11 ACE Microfinance Bank Limited Unit 3, Daniel Aliyu Street, Kwali, Abuja ABUJA 12 Achina Microfinance Bank Limited Unit Achina Aguata LGA, Anambra State ANAMBRA 13 Active Point Microfinance Bank Limited State 18A Nkemba Street, Uyo, Akwa Ibom State AKWA IBOM 14 Ada Microfinance Bank Limited Unit Agwada Town, Kokona Local Govt. Area, Nasarawa State NASSARAWA 15 Adazi-Enu Microfinance Bank Limited Unit Nkwor Market Square, Adazi- Enu, Anaocha Local Govt, Anambra State. ANAMBRA 16 Adazi-Nnukwu Microfinance Bank Limited Unit Near Eke Market, Adazi Nnukwu, Adazi, Anambra State ANAMBRA 17 Addosser Microfinance Bank Limited State 32, Lewis Street, Lagos Island, Lagos State LAGOS 18 Adeyemi College Staff Microfinance Bank Ltd Unit Adeyemi College of Education Staff Ni 1, CMS Ltd Secretariat, Adeyemi College of Education, Ondo ONDO 19 Afekhafe Microfinance Bank Ltd Unit No. -

Fertility Assessment of Soils Under Rice Cultivation in Kadawa, Garun Mallam Local Government Kano State
ISSN-L: 2223-9553, ISSN: 2223-9944 Part-I :Natural and Applied Sciences Vol. 5 No. 1 January 2014 FERTILITY ASSESSMENT OF SOILS UNDER RICE CULTIVATION IN KADAWA, GARUN MALLAM LOCAL GOVERNMENT KANO STATE G. K. Adamu 1, A. K. Aliyu 2, A. M. Jabbi 3 1 Department of Geography and Regional planning, 3 Department of Biological Sciences, Federal University Dutsinma, Katsina, NIGERIA. 1 [email protected] ABSTRACT This research was conducted in Kadawa, Garun Mallam local government of Kano State with aim of assessing the fertility of soils under rice cultivation in the area. Ten (10) composite samples were randomly collected from the top (0-20cm) in the sites. The samples were analyzed for some soil fertility index parameters using standard routine laboratory tests. In addition, Mean values of soil parameter determined were computed so as to compare the results with the critical limits for interpreting levels of soil fertility. The findings indicated that the soil texture was generally sandy loam with brown colour. The soil was moderately acidic with mean pH values of 6.07 and 5.95 in water and CaCl 2 respectively. The electrical conductivity (ECE) ranged from 0.027 to 0.2 dS/m with a mean of 0.097 dS/m. The total nitrogen (TN) ranged from 0.035 to 0.053% with a mean of 0.05%. The organic matter content (OM) ranged from 0.79 to 1.87% with a mean of 2.61%. The Available phosphorus (AP) ranged from 9.63 to 87.50ppm with a mean of 54.87ppm. Furthermore, The Exchangeable K ranged from 0.11 to 0.87Cmol/kg with a mean value of 0.24Cmol/kg and Cation Exchange Capacity (CEC) ranged from 5.0 to 11.0Cmol/kg with a mean of 7.57. -

Analysis of Human Capital Development Index in Kano State
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by International Institute for Science, Technology and Education (IISTE): E-Journals Developing Country Studies www.iiste.org ISSN 2224-607X (Paper) ISSN 2225-0565 (Online) Vol.7, No.5, 2017 Analysis of Human Capital Development Index in Kano State Dr. Nazifi Abdullahi Darma 1 Aigbedion I. Marvelous 1 Nafiu Bashir 2 Umar Abubakar kari 3 1.Department of Economics, University of Abuja 2.Department of Economics, Bayaro University Kano (BUK) 3.Department of Sociology, University of Abuja Abstract The study focuses on the analysis of human capital development index domesticated in Kano state, Nigeria. The main objective of this study is design human capital index and explores the contributors and inhibitors to the development and deployment of a healthy, educated and productive labour force in the state. The study covers the 44 local government areas and 122 wards of the State. Four key indicators were used for the design of human capital index in Kano State which are; level of education, health and wellness, workforce and employment and enabling environment. These indicators were analyzed using standardization method of ranking. From the index, some regions of the states have impressive and fair human capital index which are Northern Central, Eastern and North Western regions while some regions have poor ranking of human capital index in the State especially Far South, Western and Southern regions were most of the index were negative as per the defined indicators as captured by the level of education, health and wellness, workforce and employment and enabling environment. -

Preliminary Results from Direct-To-Facility Vaccine Deliveries in Kano, Nigeria
Preliminary results from direct-to-facility vaccine deliveries in Kano, Nigeria Muyi Aina Uchenna Igbokwe Solina Center for International Development and Research Rabiu Fagge Kano State Primary Health Care Management Board Presentation at the Health and Humanitarian Logistics Conference, Copenhagen June 8, 2017 CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of Solina Health is strictly prohibited Content Background Methods Results Learnings Conclusion 2 General information on Kano state, Nigeria Kano at a glance Kano State has 44 LGAs ▪ 11 Million (2011) Population1 Makoda Kunchi Dambatta GDP per ▪ $1,288 USD Tsanyawa Bichi 2 Minjibir Gabasawa capita Dawakin Tofa Bagwai Ungogo Tofa Dala Gezawa Shanono Rimin Gado Tarauni Ajingi KumbotsoWarawa ▪ 0.44 Million Gwarzo Kabo No. of Madobi Dawakin Kudu Kura Gaya children <1 Wudil Karaye Bumkure Albasu Kiru Garun Mallam Garko Rogo Bebeji Rano ▪ 50 deaths per 1,000 Kibiya Takai Infant mortality rate3 children Tudun Wada Sumaila ▪ BCG: 27.5% Immun. ▪ DPT3: 18.9% coverage rate4 Doguwa ▪ Fully immunised: 13.2% ▪ 1,300 PHCs;, 1,142 0 50 100 Km Healthcare facilities providing RI services SOURCE: 1. City population statistics; 2. Canback Dangtel C-GIDD, 3. MDG 2014; 4. Nigeria Demographic and Health Survey, 2013 3 Historically, a weak vaccine supply chain system significantly contributed to poor immunization coverage rates in Kano Key supply chain bottlenecks resulted in …and contributed to the poor vaccination inadequate supply of vaccine for RI sessions… coverage in Kano and other northern states DPT3 coverage by state (NDHS 2013) 1 Inadequate cold chain and poor maintenance limiting vaccine availability at service points 2 Complex and ineffective distribution architecture causing frequent stock outs 3 Inadequate and ad-hoc funding for vaccine transportation across all levels 4 Faulty vaccine forecasting and allocation which did not adequately reflect demand 5 Weak data management systems resulting in ineffective management decision making 6 Lack of proper supportive supervision due to 1. -

State Kano Code: 19 Lga: Ajingi Code: 01 Name of Registration Name of Reg
INDEPENDENT NATIONAL ELECTORAL COMMISSION (INEC) STATE KANO CODE: 19 LGA: AJINGI CODE: 01 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 AJINGI 01 AJINGI SPE. PRI. AJINGI SPE. PRI. 2 BALARE 02 BALARE PRI. SCH. BALARE PRI. SCH. 3 CHULA 03 CHULA PRI. SCH. CHULA PRI. SCH. 4 DABIN-KANAWA 04 DABIN-KANAWA PRI. SCH. DABIN-KANAWA PRI. SCH. 5 DUN-DUN 05 DUNDU PRI. SCH. DUNDU PRI. SCH. 6 GAFASA 06 TSIKO PRI. SCH. TSIKO PRI. SCH. 7 GURDUBA 07 GURDUBA PRI. SCH. GURDUBA PRI. SCH. 8 KUNKURAWA 08 KUNKURAWA PRI. SCH. KUNKURAWA PRI. SCH. 9 TORANKE 09 TORANKE PRI. SCH. TORANKE PRI. SCH. 10 UNGWA BAI 10 UNGWA BAI PRI. SCH. UNGWA BAI PRI. SCH. TOTAL LGA: ALBASU CODE: 02 NAME OF REGISTRATION NAME OF REG. AREA COLLATION NAME OF REG. AREA CENTRE S/N CODE AREA (RA) CENTRE (RACC) (RAC) 1 ALBASU CENTRAL 01 ALBASU C. PRIMARY SCHOOL ALBASU C. PRIMARY SCHOOL 2 BATAIYA 02 BATAIYA C. PRIMARY SCHOOL BATAIYA C. PRIMARY SCHOOL 3 CHAMARANA 03 DUJA C. PRIMARY SCHOOL DUJA C. PRIMARY SCHOOL 4 DAHO 04 DAHO C. PRIMARY SCHOOL DAHO C. PRIMARY SCHOOL 5 FANDA 05 FANDA C. PRIMARY SCHOOL FANDA C. PRIMARY SCHOOL 6 FARAGAI 06 FARAGAI C. PRIMARY SCHOOL FARAGAI C. PRIMARY SCHOOL 7 GAGARAME 07 S/KASUWA C. PRIMARY SCHOOL S/KASUWA C. PRIMARY SCHOOL 8 HUNGU 08 Z/GALA C. PRIMARY SCHOOL Z/GALA C. PRIMARY SCHOOL 9 SAYA-SAYA 09 SAYA-SAYA C. PRIMARY SCHOOL SAYA-SAYA C. -

RJOAS, 6(114), June 2021
RJOAS, 6(114), June 2021 DOI 10.18551/rjoas.2021-06.03 EFFORTS OF DRY-LAND FARMERS OF KANO-NIGERIA IN THE CONDITIONS OF COVID-19 PANDEMIC THAT HITS GLOBAL FOOD SECURITY Salami Azeez Oyeniyi Shelterbelt Research Station, Forestry Research Institute of Nigeria, Kano, Nigeria E-mail: [email protected] ORCID: 0000 0002 8250 0898 ABSTRACT A survey was conducted in Kano State-Nigeria aimed at exploring the travails of the dry-land farmers of the state amidst Covid-19 pandemic lockdown. The exercise was carried out in 8 Local Government Areas marked out in two sampling units within the metropolis and outside the metropolis. Within the Kano metropolis were Nassarawa, Ungogo, Tarauni and Dala; while Madobi, Minjiibir, Garun Mallam and Dambatta were outside the metropolitan. The enumeration thus pointed to the complete halt of all activities in the state during the ill-fated lockdown which was coupled with hunger, starvation, alongside stringent survival strategies; difficult access to agricultural imputes aids; and the effects on farming activities, among others. Structured interview was employed with a total of 120 respondents, using Availability Sampling Technique. However, food insecurity and malnutrition in Nigeria is as a result of the non implementation of the national and conventional food policy and agricultural programs. Nonetheless, in this critical time of economic pressure and the insurgence of Covid-19 pandemic, it is very important therefore to improve the budget allocation to the agricultural sector, as well as sustainable agricultural policy improvement programs by giving very compelling priority for nutrition on the agenda of the government, and enforcing a vibrant policy at aiding these dry-land farmers from whom the bulk of the global food production emanates. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -
Technical Cooperation for Development Planning on the One
The Federal Republic of Nigeria Small and Medium Enterprises Development Agency of Nigeria (SMEDAN) Technical Cooperation for Development Planning on the One Local Government One Product Programme for Revitalising the Rural Economy in the Federal Republic of Nigeria FINAL REPORT December 2011 Japan International Cooperation Agency (JICA) IC Net Limited Overseas Merchandise Inspection Co., Ltd. Yachiyo Engineering Co., Ltd. A2 Kano State Katsina State A9 Jigawa State Kunchi MakodaDambatta A9 Tsanyawa A9 Nigeria all area Bichi Minjibir Gabasawa Bagwai DawakinT Ungogo Shanono A2 Gezawa Tofa Dala RiminGad Ajingi Lake Chad Gwarzo Kumbotso Warawa Sokoto Lake Chad Kabo A2 Madobi DawakinKK a n o S t a t e Karaye Kura Gaya Kano NdjamenaNdjamena Wudil Maiduguri Garum Mallam Bunkure A2 Albasu Kiru Garko Kaduna Rogo Bebeji Kaduna Rano Kibiya Takai A2 AbujaAbuja A2 Sumaila Tundun Wada Ilorin A126 IbadanIbadan A2 LagosLagos A236 Enugu PortoPorto NovoNovo Benin City Doguwa A11 ¯ A11 Port Harcourt Yaounde A11 A11 Douala 0Malabo75 150 300 450 600 750 Kaduna State A11 Km A236 A235 0 10 20 40 60 80 100 A236 Km A126 A1 Zamfara State Kebbi State Kebbi State Rijau A1 A2 Agwara A1 Kaduna State A125 Mariga Kaduna State A125 Niger State A235 A125 Magama Kontogur A2 Borgu A125 A2 Rafi A125 Shiroro Niger State Niger State Mashegu Legend A1 Muya Wushishi p Airports Chanchaga A7 Bosso Primary road A2 Paikoro Local road Lavun A124 A2A124 Katcha Gurara Urban Areas Mokwa Gbako Tafa A124 Suleja A234 Intermittent stream A7 Bida A124 Perennial stream A7 Kwara State Edati Agaie Water bodies: Intermittent A1 Lavun A2 Water bodies: Perennial A1 A7 Lapai National Boundary O y o S t a t e A1 State Boundary A123 A1 Niger and Kano State Nassarawa State 0 10 20 40 60 80 A123100 Km A123 LGA Boundary K o g i S t a t e Source: ESRI Japan; Study Team Map of Nigeria iii Table of contents Abbreviations and acronyms ............................................................................................................... -
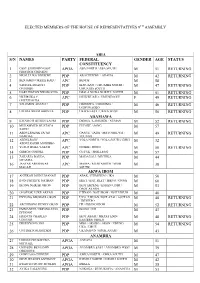
List of the Elected House of Representatives Members for the 9Th Assembly
ELECTED MEMBERS OF THE HOUSE OF REPRESENTATIVES 9TH ASSEMBLY ABIA S/N NAMES PARTY FEDERAL GENDER AGE STATUS CONSTITUENCY 1 OSSY EHIRIODO OSSY APGA ABA NORTH / ABA SOUTH M 51 RETURNING PRESTIGE CHINEDU 2 NKOLE UKO NDUKWE PDP AROCHUKWU / OHAFIA M 42 RETURNING 3 BENJAMIN OKEZIE KALU APC BENDE M 58 4 SAMUEL IFEANYI PDP IKWUANO / UMUAHIA NORTH / M 47 RETURNING ONUIGBO UMUAHIA SOUTH 5 DARLINGTON NWOKOCHA PDP ISIALA NGWA NORTH / SOUTH M 51 RETURNING 6 NKEIRUKA C. APC ISUIKWUATO / UMUNEOCHI F 49 RETURNING ONYEJEOCHA 7 SOLOMON ADAELU PDP OBINGWA / OSISIOMA / M 46 RETURNING UGWUNAGBO 8 UZOMA NKEM ABONTA PDP UKWA EAST / UKWA WEST M 56 RETURNING ADAMAWA 9 KWAMOTI BITRUS LAORI PDP DEMSA / LAMURDE / NUMAN M 52 RETURNING 10 MUHAMMED MUSTAFA PDP FUFORE / SONG M 57 SAIDU 11 ABDULRAZAK SA’AD APC GANYE / JADA / MAYO BELWA / M 49 RETURNING NAMDAS TOUNGO 12 ABDULRAUF APC YOLA NORTH / YOLA SOUTH/ GIREI M 32 ABDULKADIR MODIBBO 13 YUSUF BUBA YAKUB APC GOMBI / HONG M 50 RETURNING 14 GIBEON GOROKI PDP GUYUK / SHELLENG M 57 15 ZAKARIA DAUDA PDP MADAGALI / MICHIKA M 44 NYAMPA 16 JAAFAR ABUBAKAR APC MAIHA / MUBI NORTH / MUBI M 38 MAGAJI SOUTH AKWA IBOM 17 ANIEKAN JOHN UMANAH PDP ABAK / ETIM EKPO / IKA M 50 18 IFON PATRICK NATHAN PDP EKET / ESIT EKET / IBENO / ONNA M 60 19 IKONG NSIKAK OKON PDP IKOT EKPENE / ESSIEN UDIM / M 53 OBOT AKARA 20 ONOFIOK LUKE AKPAN PDP ETINAN / NSIT IBOM / NSIT UBIUM M 40 21 ENYONG MICHAEL OKON PDP UYO / URUAN /NSIT ATAI / ASUTAN M 48 RETURNING / IBESIKPO 22 ARCHIBONG HENRY OKON PDP ITU /IBIONO IBOM M 52 RETURNING 23 EMMANUEL UKPONG-UDO -

Press Release | May 12, 2020 Media Relations Office Mr
Press Release | May 12, 2020 Media Relations Office Mr. Moses Duku Mobile: +234 805 222 5465 Phone: +234 803 906 7000 | ext. 4635 Email: moses.duku@julius- berger.com Kaduna State and Kano State Communities Receive Julius Berger Aid Over the weekend of May 9, 2020, Julius Berger Nigeria Plc’s (Julius Berger) Covid-19 response efforts pushed further North, bringing its Food for our Communities campaign to Kaduna State and Kano State where the Company delivered 36,000 kilograms of food supplies to communities in need. In Kaduna State, the Kawo District, Rigachukun District and Zaria District received food relief packages, containing rice, cooking oil and other kitchen essentials. The same food relief packages were distributed to the Bebeji, Kura and Garun Mallam Districts in Kano State. Since the launch of its Food for our Communities campaign, Julius Berger has donated over 100,000 Kilograms of food supplies to communities. The Company remains dedicated to supporting the fight to curb the Covid-19 pandemic in Nigeria and minimize its impact on citizens. In addition to supplementing communities’ access to staple food supplies, Julius Berger has donated needed resources such as beds and personal protective equipment to hospitals and healthcare facilities, as well as supporting Federal and State efforts towards sanitation and safety. About Julius Berger Julius Berger Nigeria Plc is a Nigerian company offering integrated construction solutions. The company has been operating in Nigeria since 1965 and its scope covers all areas of construction. Julius Berger is dedicated to utilization of cutting-edge technologies, the continuous investment in staff training and strong partnership with clients. -
How to Set up and Manage a Community Journalism Network
HOW TO SET UP AND MANAGE A COMMUNITY JOURNALISM NETWORK Implemented by Adam Smith International 1 How to Set Up and Manage a Community Journalism Network Preface Nigeria is blessed with numerous media organisations (though analysts are still asking for more), from the print – newspapers, magazines and other periodicals to broadcast – radio, television, satellite stations and online media. As of November 2016, there were over three hundred radio stations, one hundred television stations, thirty Internet radio stations, six international broadcasters across Nigeria and still counting. There were also sixty-six newspapers and magazines across the country during the same period1 Nigeria also enjoys relative freedom of the press when compared with some other African, Asian, Caribbean or even European countries. However, ninety per cent of Nigeria’s media spread are in the urban centres, leaving the remaining ten per cent to the semi urban fringes, with virtually no newspaper, radio or television station located in any remote, rural village. The implication of this, is that news coverage, programme focus, analyses and general perspectives on issues centre on the urban and semi urban areas, leaving the rural settlers, who contributed a chunk of Nigeria’s population with neither a voice nor fair representation in the media. This is what led to the community journalism initiative. Enhancing Nigeria’s Advocacy for Better Business Environment Phase 2 (ENABLE2), as part of its intervention to improve the professional competence of the Nigerian media in the coverage of small business women and men 1 See list of Nigerian media organisations in appendix 1 How to Set Up and Manage a Community Journalism Network 2 and the smallholder farmers in the rural communities, embarked on this initiative.