Urine Blockage in Newborns
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hydronephrosis
Hydronephrosis Natasha Brownrigg RN(EC), MN, NP-Pediatrics Assistant Clinical Professor, McMaster School of Nursing Nurse Practitioner, Pediatric Urology, McMaster Children’s Hospital, Hamilton, ON, Canada Dr. Jorge DeMaria Pediatric Urologist, McMaster Children’s Hospital Professor Department of Surgery/Urology, McMaster University, Hamilton, ON, Canada Dr. Luis H.P. Braga Pediatric Urologist, McMaster Children’s Hospital. Associate professor Department of Surgery/Urology, McMaster University, Hamilton, ON, Canada What is hydronephrosis? Hydro Nephrosis Hydronephrosis += Refers to water Refers to the kidney A build up of fluid or fluid (urine) in the kidney Hydronephrosis is the medical term for a build-up of urine in the kidney. As the urine builds up, it stretches or dilates the inside of the kidney, known as the collecting system. If an unborn baby has hydronephrosis, an ultrasound scan will show a build-up of urine in the kidney. This is called “antenatal hydronephrosis.” Hydronephrosis is found in as many as five out of 100 pregnancies. Hydronephrosis may also be found after birth. For example, if a baby has a urinary tract infection, an ultrasound of the baby’s kidneys and bladder may detect hydronephrosis. Key points to remember if your baby has hydronephrosis • Your baby can grow and develop normally with hydronephrosis. • Hydronephrosis may affect one kidney or both. • Hydronephrosis is a finding, not a disease. • Further tests are needed to find the cause of hydronephrosis. • If the cause is known, a pediatric urologist will discuss the possible treatment. Surgery is sometimes required to correct the cause of the hydronephrosis. Hydronephrosis is often transient and improves without any intervention. -
Acute Phosphate Nephropathy Alexander K
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector http://www.kidney-international.org the renal consult & 2009 International Society of Nephrology Acute phosphate nephropathy Alexander K. Rocuts1, Sushrut S. Waikar1, Mariam P. Alexander1,2, Helmut G. Rennke2 and Ajay K. Singh1 1Renal Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA and 2Department of Pathology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA minute. The rest of the examination was unremarkable. CASE PRESENTATION HerlaboratorydataissummarizedinTable1. A 60-year-old white Latino female with a clinical diagnosis A postoperative kidney ultrasound showed no of diabetes mellitus (diagnosed in 1993) and hypertension hydronephrosis. was referred to the chronic kidney disease clinic at The etiology of the acute kidney injury was unclear. Brigham and Women’s Hospital for the evaluation of acute Progressive diabetic nephropathy exacerbated by other kidney injury; serum creatinine had increased from a contributory factors, such as exposure to lisinopril, baseline of 0.9 to 1.5 mg/dl in a 11-week period. She was acetylsalicylic acid, or naproxen, was regarded as the most asymptomatic at the time of presentation. Her past plausible explanation. Despite discontinuation of these medical history included a total abdominal hysterectomy medications, kidney function did not improve; it worsened with bilateral salpingo oophorectomy and upper in a 4-week period after presentation. Hence, a kidney vaginectomy for high-grade squamous intraepithelial biopsy was performed. lesion of the cervix, 11 weeks prior to presentation. Three weeks prior to presentation (8 weeks after surgery) and within a week of each other, she was evaluated for two consecutive episodes of acute onset of chest pain with pulmonary edema in the setting of severe hypertension. -

The Reproductive System
27 The Reproductive System PowerPoint® Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska © 2012 Pearson Education, Inc. Introduction • The reproductive system is designed to perpetuate the species • The male produces gametes called sperm cells • The female produces gametes called ova • The joining of a sperm cell and an ovum is fertilization • Fertilization results in the formation of a zygote © 2012 Pearson Education, Inc. Anatomy of the Male Reproductive System • Overview of the Male Reproductive System • Testis • Epididymis • Ductus deferens • Ejaculatory duct • Spongy urethra (penile urethra) • Seminal gland • Prostate gland • Bulbo-urethral gland © 2012 Pearson Education, Inc. Figure 27.1 The Male Reproductive System, Part I Pubic symphysis Ureter Urinary bladder Prostatic urethra Seminal gland Membranous urethra Rectum Corpus cavernosum Prostate gland Corpus spongiosum Spongy urethra Ejaculatory duct Ductus deferens Penis Bulbo-urethral gland Epididymis Anus Testis External urethral orifice Scrotum Sigmoid colon (cut) Rectum Internal urethral orifice Rectus abdominis Prostatic urethra Urinary bladder Prostate gland Pubic symphysis Bristle within ejaculatory duct Membranous urethra Penis Spongy urethra Spongy urethra within corpus spongiosum Bulbospongiosus muscle Corpus cavernosum Ductus deferens Epididymis Scrotum Testis © 2012 Pearson Education, Inc. Anatomy of the Male Reproductive System • The Testes • Testes hang inside a pouch called the scrotum, which is on the outside of the body -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Impact of Urolithiasis and Hydronephrosis on Acute Kidney Injury in Patients with Urinary Tract Infection
bioRxiv preprint doi: https://doi.org/10.1101/2020.07.13.200337; this version posted July 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Impact of urolithiasis and hydronephrosis on acute kidney injury in patients with urinary tract infection Short title: Impact of urolithiasis and hydronephrosis on AKI in UTI Chih-Yen Hsiao1,2, Tsung-Hsien Chen1, Yi-Chien Lee3,4, Ming-Cheng Wang5,* 1Division of Nephrology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi, Taiwan 2Department of Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, Taiwan 3Department of Internal Medicine, Fu Jen Catholic University Hospital, Fu Jen Catholic University, New Taipei, Taiwan 4School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei, Taiwan 5Division of Nephrology, Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan *[email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.07.13.200337; this version posted July 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Abstract Background: Urolithiasis is a common cause of urinary tract obstruction and urinary tract infection (UTI). This study aimed to identify whether urolithiasis with or without hydronephrosis has an impact on acute kidney injury (AKI) in patients with UTI. -

Urology & Incontinence
Urology & Incontinence - Glossary of Terms Anti-reflux Refers to a tube or collapsible material within a urine collection device to help prevent urine from reentering the tubing. Applicator collar Found on some Hollister male external catheters, a plastic guide with notches for the thumb and forefinger to assist proper placement against the tip of the penis. Aseptic intermittent catheterization The process of performing intermittent catheterization using sterile equipment and inserting the catheter in a sterile way. This would include a sterile ready-to-use product that can be inserted with gloves using a no-touch technique (e.g., the Advance Plus intermittent catheter or a VaPro hydrophilic catheter). Benzalkonium chloride (BZK) An antimicrobial solution used for cleansing the urethral opening prior to inserting an intermittent catheter. Does not stain skin or clothing. Bladder A collapsible balloon-like muscular organ that lies in the pelvis and functions to store and expel urine. Bladder catheterization A procedure in which a catheter is passed through the urethra or stoma into the bladder, usually for the purpose of draining urine. Bladder control The ability to control urination. Bladder diary A printed or electronic form to keep track of when one urinates or leaks urine. Catheter (urinary) A special type of hollow tube inserted through the urethra or a stoma to the bladder to withdraw urine or instill medication. Catheterization The process of inserting a tube into the bladder to drain urine. Clean intermittent catheterization The process of emptying the bladder using a clean intermittent catheter. It involves inserting and removing a catheter, typically several times a day. -
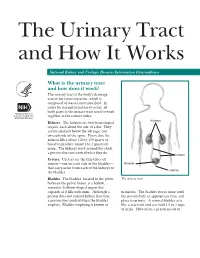
The Urinary Tract and How It Works
The Urinary Tract and How It Works National Kidney and Urologic Diseases Information Clearinghouse What is the urinary tract and how does it work? The urinary tract is the body’s drainage system for removing urine, which is composed of wastes and extra fluid. In order for normal urination to occur, all body parts in the urinary tract need to work together in the correct order. Kidneys Kidneys. The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the spine. Every day, the kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine. The kidneys work around the clock; a person does not control what they do. Ureters Ureters. Ureters are the thin tubes of muscle—one on each side of the bladder— Bladder that carry urine from each of the kidneys to Urethra the bladder. Bladder. The bladder, located in the pelvis The urinary tract between the pelvic bones, is a hollow, muscular, balloon-shaped organ that expands as it fills with urine. Although a urination. The bladder stores urine until person does not control kidney function, the person finds an appropriate time and a person does control when the bladder place to urinate. A normal bladder acts empties. Bladder emptying is known as like a reservoir and can hold 1.5 to 2 cups of urine. How often a person needs to urinate depends on how quickly the kidneys Why is the urinary tract produce the urine that fills the bladder. -

Renal Tubular Acidosis in Children: State of the Art, Diagnosis and Treatment
www.medigraphic.org.mx Bol Med Hosp Infant Mex 2013;70(3):178-193 REVIEW ARTICLE Renal tubular acidosis in children: state of the art, diagnosis and treatment Ricardo Muñoz-Arizpe,1 Laura Escobar,2 Mara Medeiros3 ABSTRACT Overdiagnosis of renal tubular acidosis (RTA) has been recently detected in Mexican children, perhaps due to diagnostic errors as well as due to a lack of knowledge regarding the pathophysiology and molecular biochemistry involved in this illness. The objective of the present study is to facilitate the knowledge and diagnosis of RTA, a clinical condition infrequently seen worldwide. RTA is an alteration of the acid-base equilibrium due to a bicarbonate wasting in the proximal renal tubules [proximal RTA, (pRTA) or type 2 RTA] or due to a distal nephron hy- drogen ion excretion defect [distal RTA (dRTA) or type 1 RTA]. Hyperkalemic, or type 4 RTA, is due to alterations in aldosterone metabolism. RTA may be primary, secondary, acquired or hereditary and frequently presents secondary to an array of systemic diseases, usually accom- panied by multiple renal tubular defects. The main defect occurs in the transmembrane transporters such as carbonic anhydrase (CA I and + - - + - II), H -ATPase, HCO3 /Cl (AE1) exchanger and Na /HCO3 (NBCe1) cotransporter. Diagnosis should include the presence of hyperchloremic metabolic acidosis with normal serum anion gap (done in an arterial or arterialized blood sample), lack of appetite, polyuria, thirst, growth failure, and rickets; nephrocalcinosis and renal stones (in dRTA); abnormal urine anion gap and abnormal urine/serum pCO2 gradient. Diagnosis of a primary systemic disease must be made in cases of secondary RTA. -

Silent Hydronephrosis, a Hazard Revisited
SILENT HYDRONEPHROSIS, A HAZARD REVISITED By JOEL S. ROSEN, M.D., JOHN B. NANNINGA, M.D. and VINCENT J. O'CONOR, M.D. Midwest Regional Spinal Cord Injury Care System, Chicago, Illinois, U.S.A. Abstract. Six patients with neurogenic bladder secondary to spinal cord injury were seen in our Centre for routine follow-up. All of these individuals had attained the catheter-free state by various means and were, by their standards, functioning very well. They had gone from 6 months to 2t years without genito-urinary re-evaluations. One individual had a normal urogram I year after catheter removal and then 2 years later was noted to have bilateral hydronephrosis. Development of silent hydronephrosis in the catheter-free state, its treatment, and a regimen for following patients are discussed. THE recognition of hydronephrosis following spinal cord injury has been docu mented in the past by several authorities (Talbot & Bunts, 1940; Hutch & Bunts, 1951; Damanski & Gibbon, 1956). Damanski and Gibbon stated that hydro nephrosis occurred in one.;.third of a group of patients suffering from spinal cord injury. The changes have been reported to occur as early as 2 months after injury to as long as 8 years later. Ross (1963) has found hydronephrosis to be associated with the neural damage, urinary infection and back pressure; the importance of each factor varying considerably with the individual, Ascoli and Franch (1970) noted hydronephrosis most frequently in patients more than 4 years post trauma. Warning signs of impending hydronephrosis include the onset of urinary tract infection, deterioration of bladder function, increasing residual urine, bladder hypertonia and the appearance of bladder diverticula and reflux. -

15-1040-Junu Oh-Neuronal.Key
Neuronal Control of the Bladder Seung-June Oh, MD Department of urology, Seoul National University Hospital Seoul National University College of Medicine Contents Relevant end organs and nervous system Reflex pathways Implication in the sacral neuromodulation Urinary bladder ! body: detrusor ! trigone and bladder neck Urethral sphincters B Preprostatic S Smooth M. Sphincter Passive Prostatic S Skeletal M. Sphincter P Prostatic SS P-M Striated Sphincter Membraneous SS Periurethral Striated M. Pubococcygeous Spinal cord ! S2–S4 spinal cord ! primary parasympathetic micturition center ! bladder and distal urethral sphincter ! T11-L2 spinal cord ! sympathetic outflow ! bladder and proximal urethral sphincter Peripheral innervation ! The lower urinary tract is innervated by 3 principal sets of peripheral nerves: ! parasympathetic -pelvic n. ! sympathetic-hypogastric n. ! somatic nervous systems –pudendal n. ! Parasympathetic and sympathetic nervous systems form pelvic plexus at the lateral side of the rectum before reaching bladder and sphincter Sympathetic & parasympathetic systems ! Sympathetic pathways ! originate from the T11-L2 (sympathetic nucleus; intermediolateral column of gray matter) ! inhibiting the bladder body and excite the bladder base and proximal urethral sphincter ! Parasympathetic nerves ! emerge from the S2-4 (parasympathetic nucleus; intermediolateral column of gray matter) ! exciting the bladder and relax the urethra Sacral somatic system !emerge from the S2-4 (Onuf’s nucleus; ventral horn) !form pudendal nerve, providing -

The Digestive System
69 chapter four THE DIGESTIVE SYSTEM THE DIGESTIVE SYSTEM The digestive system is structurally divided into two main parts: a long, winding tube that carries food through its length, and a series of supportive organs outside of the tube. The long tube is called the gastrointestinal (GI) tract. The GI tract extends from the mouth to the anus, and consists of the mouth, or oral cavity, the pharynx, the esophagus, the stomach, the small intestine, and the large intes- tine. It is here that the functions of mechanical digestion, chemical digestion, absorption of nutrients and water, and release of solid waste material take place. The supportive organs that lie outside the GI tract are known as accessory organs, and include the teeth, salivary glands, liver, gallbladder, and pancreas. Because most organs of the digestive system lie within body cavities, you will perform a dissection procedure that exposes the cavities before you begin identifying individual organs. You will also observe the cavities and their associated membranes before proceeding with your study of the digestive system. EXPOSING THE BODY CAVITIES should feel like the wall of a stretched balloon. With your skinned cat on its dorsal side, examine the cutting lines shown in Figure 4.1 and plan 2. Extend the cut laterally in both direc- out your dissection. Note that the numbers tions, roughly 4 inches, still working with indicate the sequence of the cutting procedure. your scissors. Cut in a curved pattern as Palpate the long, bony sternum and the softer, shown in Figure 4.1, which follows the cartilaginous xiphoid process to find the ventral contour of the diaphragm. -

The Urinary System Dr
The urinary System Dr. Ali Ebneshahidi Functions of the Urinary System • Excretion – removal of waste material from the blood plasma and the disposal of this waste in the urine. • Elimination – removal of waste from other organ systems - from digestive system – undigested food, water, salt, ions, and drugs. + - from respiratory system – CO2,H , water, toxins. - from skin – water, NaCl, nitrogenous wastes (urea , uric acid, ammonia, creatinine). • Water balance -- kidney tubules regulate water reabsorption and urine concentration. • regulation of PH, volume, and composition of body fluids. • production of Erythropoietin for hematopoieseis, and renin for blood pressure regulation. Anatomy of the Urinary System Gross anatomy: • kidneys – a pair of bean – shaped organs located retroperitoneally, responsible for blood filtering and urine formation. • Renal capsule – a layer of fibrous connective tissue covering the kidneys. • Renal cortex – outer region of the kidneys where most nephrons is located. • Renal medulla – inner region of the kidneys where some nephrons is located, also where urine is collected to be excreted outward. • Renal calyx – duct – like sections of renal medulla for collecting urine from nephrons and direct urine into renal pelvis. • Renal pyramid – connective tissues in the renal medulla binding various structures together. • Renal pelvis – central urine collecting area of renal medulla. • Hilum (or hilus) – concave notch of kidneys where renal artery, renal vein, urethra, nerves, and lymphatic vessels converge. • Ureter – a tubule that transport urine (mainly by peristalsis) from the kidney to the urinary bladder. • Urinary bladder – a spherical storage organ that contains up to 400 ml of urine. • Urethra – a tubule that excretes urine out of the urinary bladder to the outside, through the urethral orifice.