Review of an Initial Experience with an Experimental Spectral Photon-Counting Computed Tomography System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SI Traceable Solar Spectral Irradiance Measurement Based on a Quantum Benchmark: a Prototype Design
remote sensing Article SI Traceable Solar Spectral Irradiance Measurement Based on a Quantum Benchmark: A Prototype Design Xiaobing Zheng *, Maopeng Xia, Wenchao Zhai, Youbo Hu, Jianjun Li, Yinlin Yuan and Weiwei Pang Key Laboratory of Optical Calibration and Characterization, Anhui Institute of Optics and Fine Mechanics, Chinese Academy of Sciences, Hefei, Anhui 230031, China; [email protected] (M.X.); [email protected] (W.Z.); [email protected] (Y.H.); [email protected] (J.L.); [email protected] (Y.Y.); [email protected] (W.P.) * Correspondence: [email protected] Received: 1 March 2020; Accepted: 29 April 2020; Published: 4 May 2020 Abstract: We propose a space benchmark sensor with onboard SI (Système International) traceability by means of quantum optical radiometry. Correlated photon pairs generated by spontaneous parametric down-conversion (SPDC) in nonlinear crystals are used to calibrate the absolute responsivity of a solar observing radiometer. The calibration is systematic, insensitive to degradation and independent of external radiometric standards. Solar spectral irradiance at 380–2500 nm is traceable to the photon rate and Planck’s constant with an expected uncertainty of about 0.35%. The principle of SPDC calibration and a prototype design of the solar radiometer are introduced. The uncertainty budget is analyzed in consideration of errors arising from calibration and observation modes. Keywords: radiometric benchmark; spontaneous parametric down-conversion; correlated photons; detector calibration; solar irradiance 1. Introduction Space radiometric benchmarks were proposed in recent years to reveal the trend of climate change and evaluate the energy budget of the Earth system with high confidence [1–4]. -

B2,3,8,X26093 Page 1 of 9 IAC-14-B2,3,8,X26093 IMPLICATIONS of SKY RADIANCE on DEEP-SPACE OPTICAL COMMUNICATION LINKS Ke
65th International Astronautical Congress, Toronto, Canada. Copyright ©2014 by the International Astronautical Federation. All rights reserved. IAC-14-B2,3,8,x26093 IMPLICATIONS OF SKY RADIANCE ON DEEP-SPACE OPTICAL COMMUNICATION LINKS Kevin Shortt German Aerospace Center, Germany, [email protected] Dirk Giggenbach German Aerospace Center, Germany, [email protected] Thomas Dreischer RUAG Schweiz AG, Switzerland, [email protected] Carlos Rivera ISDEFE, Spain, [email protected] Robert Daddato, Andrea Di Mira, Igor Zayer European Space Agency, Germany [email protected], [email protected], [email protected] As the number of deep-space missions that are turning to optical communications to support science operations increases, system designers are taking a more in depth look at the link budgets that govern such links. Noise sources, such as the radiance arising from scattering in the Earth’s atmosphere and light reflected from planetary bodies in close visual proximity to spacecraft, become particularly critical given the photon-starved channels normally associated with deep-space links. In the case of the Earth’s atmosphere, sky radiance becomes a significant factor when considering daytime operations especially when operators need to support spacecraft contacts close to the Sun. This paper encapsulates the implications of sky radiance on deep-space optical communication scenarios and provides an overview of the current efforts underway in Europe to further quantify its impact on future mission operations. I. INTRODUCTION In the European context, this research is particularly timely given that the European Space Agency, as well Photons received as a result of sky radiance have a as other European players, have set their sights on a major impact on optical communication links to deep- number of deep-space missions in the coming years. -

TOPICAL REVIEW Quantum Radiometry Sergey V
Journal of Modern Optics Vol. 56, No. 9, 20 May 2009, 1045–1052 TOPICAL REVIEW Quantum radiometry Sergey V. Polyakova,b and Alan L. Migdalla,b* aOptical Technology Division, National Institute of Standards and Technology, 100 Bureau Drive, Gaithersburg, MD 20899-8441, USA; bJoint Quantum Institute, University of Maryland, College Park, MD 20742, USA (Received 1 March 2009; final version received 21 March 2009) We review radiometric techniques that take advantage of photon counting and stem from the quantum laws of nature. We present a brief history of metrological experiments and review the current state of experimental quantum radiometry. Keywords: single photon detector; metrology; high accuracy measurement; parametric downconversion Conventionally defined, radiometry is the field that photon-pair sources and single-photon or photon- studies the measurement of electromagnetic radiation number-resolving photodetectors. As such, these mea- in terms of its power, spectral characteristics, and other surements are based on quantum mechanical laws parameters. The term applies to electromagnetic radi- that guarantee certain properties of photon statistics ation characterization in a wavelength range from and rely on our ability to reliably detect single photons. nanometers to tens of microns and at all optical power Ideally, the accuracy of measurements based on levels. Because radiometry is defined so broadly, a wide photon counting scales as 1=N1=2, where N is the variety of measurement devices, or radiometers, with number of detected photons. Therefore, to match the a variety of physical characteristics are used. It is state-of-the-art accuracy of conventional radiometry therefore necessary to maintain a common scale for one needs to collect 4108 single photon detections. -

Scintillator Based Color X-Ray Photon Counting Imager Stijn Vandewiele1,4, Bart Dierickx1,2, Benoit Dupont1,3, Arnaud Defernez1, Dirk Uwaerts1
Scintillator based color X-ray photon counting imager Stijn Vandewiele1,4, Bart Dierickx1,2, Benoit Dupont1,3, Arnaud Defernez1, Dirk Uwaerts1 1Caeleste, Antwerp, Belgium, 2V.U.B., Brussels, Belgium, 3Université Paris XIII, France, 4University of Ghent, Belgium With the ubiquitus usage of radiography in many medical diagnosis, the urge to achieve the lowest possible radiation dose is a driving force for the X-ray image sensor community. The ultimate signal to noise ratio that one can theoretically achieve is the quantum limit, where each and every photon reaching the imager is counted. Additionally, photon counting comes with abenefit: the possibility to sort incoming X-ray photons based on their energy, thus achieving “color X-ray”, a real added value for the diagnostician. As shown in [1], from electronics standpoint state-of-the-art photon counting pixels [2,3,4] use direct detection, whereby the X-ray to charge conversion happens by the photo- electric effect in a high-Z semiconductor photoconductor or photodiode. From X-ray source From X-ray source Heavy element Heavy element scintillator photodiode or Visible photoresistor light Bump bonds Optical glue flash ROIC ROIC wafer wafer thickness 5000...20000 e- 100…500 e- charge packet charge packet Figure 1 Direct (left) vs indirect (center) X-photon detection technics, detector prototype(right) In direct detection material, an X-ray photon with a typical energy for medical imaging produces about 5000 to 20000 electrons. Photon counting imagers based on direct detection materials have been used in scientific and medical imagers. However manufacturing of such detector in large scale, compatible with applications such as Chest Xray or Mammography faces several challenges. -

Photomultiplier Tubes
CHAPTER 6 PHOTON COUNTING 1) 2) 4) - 12) Photon counting is an effective technique used to detect very-low- level-light such as Raman spectroscopy, fluorescence analysis, and chemical or biological luminescence analysis where the absolute mag- nitude of the light is extremely low. This section describes the prin- ciples of photon counting, its operating methods, detection capabili- ties, and advantages as welll as typical characteristics of photomulti- plier tubes designed for photon counting. © 2007 HAMAMATSU PHOTONICS K. K. 126 CHAPTER 6 PHOTON COUNTING 6.1 Analog and Digital (Photon Counting) Modes The methods of processing the output signal of a photomultiplier tube can be broadly divided into analog and digital modes, depending on the incident light intensity and the bandwidth of the output processing cir- cuit. As Figure 6-1 shows, when light strikes the photocathode of a photomultiplier tube, photoelectrons are emitted. These photoelectrons are multiplied by the cascade process of secondary emission through the dyn- odes (normally 106 to 107 times) and finally reach the anode connected to an output processing circuit. PHOTO- CATHODE FIRST DYNODE ANODE P PULSE HEIGHT SINGLE PHOTON Dy1 Dy2 Dy-1 Dyn ELECTRON GROUP THBV3_0601 Figure 6-1: Photomultiplier tube operation in photon counting mode When observing the output signal of a photomultiplier tube with an oscilloscope while varying the incident light level, output pulses like those shown in Figure 6-2 are seen. At higher light levels, the output pulse intervals are narrow so that they overlap each other, producing an analog waveform (similar to (a) and (b) of Figure 6-2). -

Photon Counting X-Ray Detector Systems
Thesis for the degree of Licentiate Sundsvall 2005 Photon Counting X-ray Detector Systems Börje Norlin Supervisors: Docent Christer Fröjdh Professor Hans-Erik Nilsson Electronics Design Division, in the Department of Information Technology and Media Mid Sweden University, SE-851 70 Sundsvall, Sweden ISSN 1652-8948 Mid Sweden University Licentiate Thesis 2 ISBN 91-85317-01-2 Akademisk avhandling som med tillstånd av Mittuniversitetet i Sundsvall framläggs till offentlig granskning för avläggande av licentiatexamen i elektronik fredagen den 11 februari 2005, klockan 10.15 i sal M102, Mittuniversitetet Sundsvall. Seminariet kommer att hållas på engelska. Photon Counting X-ray Detector Systems Börje Norlin © Börje Norlin, 2005 Electronics Design Division, in the Department of Information Technology and Media Mid Sweden University, SE-851 70 Sundsvall Sweden Telephone: +46 (0)60 148594 Printed by Kopieringen Mittuniversitetet, Sundsvall, Sweden, 2005 To my wife Monica! …my rose from Mid Sweden. ABSTRACT This licentiate thesis concerns the development and characterisation of X-ray imaging detector systems. “Colour” X-ray imaging opens up new perspectives within the fields of medical X-ray diagnosis and also in industrial X-ray quality control. The difference in absorption for different “colours” can be used to discern materials in the object. For instance, this information might be used to identify diseases such as brittle-bone disease. The “colour” of the X-rays can be identified if the detector system can process each X-ray photon individually. Such a detector system is called a “single photon processing” system or, less precise, a “photon counting system”. With modern technology it is possible to construct photon counting detector systems that can resolve details to a level of approximately 50 µm. -
Radiometry from Watts to Single-Photons
Bridging the Gap: Radiometry from Watts to Single-Photons A. Migdall B. Calkins D. Livigni C. Cromer R. P. Mirin M. Dowell S. W. Nam J. Fan S. V. Polyakov T. Gerrits M. Stevens J. Lehman N. Tomlin A. Lita I. Vayshenker NIST, Boulder & Gaithersburg NEWRAD Maui, HI Sept. 22, 2011 Outline • Existing Radiometry and The Gap (What this talk is and is not about) • Bridging the Gap efforts (review) • Hope: Single-Photon Tools • Issues and concerns Bridging the Gap Absolute Radiometric Standards Sources Detectors Blackbody Trap: Radiometer T Electrical Substitution Temperature Radiance Radiant power Synchrotron e- Trap: B-field Semiconductor Radiant power (transfer standard) B-field, current, energy Radiance Radiometry Electrical Substitution Radiometry High-Accuracy Laser Cryogenic Optimized Radiometer Cryogenic (HACR) 1980s Radiometer (LOCR) 1990s From NIST Technical Note 1421, A. Parr Optical Power = Electrical Power Bridging the Gap Present Limits: • “World’s best” cryogenic radiometry is U = 0.01% • Primary standards (cryogenic radiometers) operate over limited range and relatively “high” powers • Typical operation is ~100 uW to ~1 mW • Dissemination to customers degrades due to transfer standard limits ~1% • Optical power traceability has the poorest uncertainty of major measurands • Difficult to link the lower range of optical powers to primary standards No formal connection between classical methods to measure optical power and new methods to measure single photons Bridging the Gap The gap 15 order-of-magnitude gap between cryogenic radiometry -
PHOTON COUNTING Using Photomultiplier Tubes INTRODUCTION
TECHNICAL INFORMATION MAY. 1998 PHOTON COUNTING Using Photomultiplier Tubes INTRODUCTION Recently, non-destructive and non-invasive measurement using light is becoming more and more popular in diverse fields including biological, chemical, medical, material analysis, industrial instruments and home appliances. Technologies for detecting low level light are receiving par- ticular attention since they are effective in allowing high precision and high sensitivity measurements without changing the properties of the objects. Biological and biochemical examinations, for example, use low-light-level measurement for cell qualitative and quanlitative by detecting fluorescence emitted from cells labeled with a fluorescent dye. In clinical testing and medi- cal diagnosis, techniques such as in-vitro assay and im- munoassay have become essential for blood analysis, blood cell counting, hormone inspection and diagnosis of cancer and various infectious diseases. These techniques also involve low-light-level measurement such as colorim- etry, absorption spectroscopy, fluorescence photometry, and detection of light scattering or Iuminescence measure- ment. In RIA (radioimmunoassay) which has been used in immunological examinations using radioisotopes, radia- tion emitted from a sample is converted into low level light which must be measured with high sensitivity. In addition, fluorescence and Iuminescence measurements are used for rapid hygienic testing and monitoring processes in in- spections for bacteria contamination in water or in food processing. -
Few-Photon Computed X-Ray Imaging
Few-photon computed x-ray imaging 1* 1 ZHEYUAN ZHU, SHUO PANG 1CREOL, The College of Optics and Photonics, University of Central Florida, 4304 Scorpius St, Orlando, FL, 32816, USA * [email protected] Abstract: X-ray is a ubiquitous imaging modality in clinical diagnostics and industrial inspections, thanks to its high penetration power. Conventional x-ray imaging system, equipped with energy-integrating detectors, collects approximately 103 – 104 counts per pixel to ensure sufficient signal to noise ratio (SNR). The recent development of energy sensitive photon counting detectors opens new possibilities for x-ray imaging at low photon flux. In this paper, we report a novel photon-counting scheme that records the time stamp of individual photons, which follows a negative binomial distribution, and demonstrate the reconstruction based on the few-photon statistics. The projection and tomography reconstruction from measurements of ~ 16 photons show the potential of using photon counting detectors for dose-efficient x-ray imaging systems. © 2018 Optical Society of America under the terms of the OSA Open Access Publishing Agreement 1. Introduction Due to its high penetrating power, x-ray imaging is extensively used as a non-invasive imaging method in medical diagnosis and industrial inspections. Among many x-ray contrast mechanisms, such as phase contrast [1] and coherent scattering [2] etc., x-ray imaging modalities based on attenuation, such as radiography (projection) and computed tomography (CT), remain the most common ones. Conventional x-ray imaging systems count 103-104 photons per pixel in a fixed period. To ensure the signal to noise ratio (SNR), high radiation dose is administrated to the sample [3], prohibiting the imaging of objects that are susceptible to radiation damage. -

A Photon-Counting Detector for Exoplanet Missions*
A photon-counting detector for exoplanet missions* D. F. Figer†a, J. Leea, B. J. Hanolda, B. F. Aullb, J. A. Gregoryb, D. R. Schuetteb aCenter for Detectors, Rochester Institute of Technology, 74 Lomb Memorial Drive, Rochester, NY 14623; bLincoln Laboratory, Massachusetts Institute of Technology, 244 Wood St, Lexington, MA 02420 ABSTRACT This paper summarizes progress of a project to develop and advance the maturity of photon-counting detectors for NASA exoplanet missions. The project, funded by NASA ROSES TDEM program, uses a 256×256 pixel silicon Geiger- mode avalanche photodiode (GM-APD) array, bump-bonded to a silicon readout circuit. Each pixel independently registers the arrival of a photon and can be reset and ready for another photon within 100 ns. The pixel has built-in circuitry for counting photo-generated events. The readout circuit is multiplexed to read out the photon arrival events. The signal chain is inherently digital, allowing for noiseless transmission over long distances. The detector always operates in photon counting mode and is thus not susceptible to excess noise factor that afflicts other technologies. The architecture should be able to operate with shot-noise-limited performance up to extremely high flux levels, >106 photons/second/pixel, and deliver maximum signal-to-noise ratios on the order of thousands for higher fluxes. Its performance is expected to be maintained at a high level throughout mission lifetime in the presence of the expected radiation dose. Keywords: detector, read noise, avalanche photodiode, array, exoplanet 1. INTRODUCTION NASA’s ultimate goal in exploring extrasolar planets (exoplanets) is to identify bodies like Earth that can support life. -
Questionnaire on Activities in Radiometry and Photometry
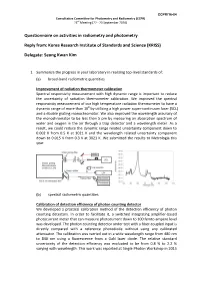
CCPR/16-04 Consultative Committee for Photometry and Radiometry (CCPR) 23rd Meeting (22 - 23 September 2016) Questionnaire on activities in radiometry and photometry Reply from: Korea Research Institute of Standards and Science (KRISS) Delegate: Seung Kwan Kim 1. Summarize the progress in your laboratory in realizing top-level standards of: (a) broad-band radiometric quantities Improvement of radiation thermometer calibration Spectral responsivity measurement with high dynamic range is important to reduce the uncertainty of radiation thermometer calibration. We improved the spectral responsivity measurement of our high temperature radiation thermometer to have a dynamic range of more than 108 by utilizing a high power super-continuum laser (SCL) and a double grating monochromator. We also improved the wavelength accuracy of the monochromator to be less than 5 pm by measuring an absorption spectrum of water and oxygen in the air through a trap detector and a wavelength meter. As a result, we could reduce the dynamic range related uncertainty component down to 0.002 K from 0.5 K at 3021 K and the wavelength related uncertainty component down to 0.015 K from 0.3 K at 3021 K. We submitted the results to Metrologia this year. (b) spectral radiometric quantities Calibration of detection efficiency of photon counting detector We developed a practical calibration method of the detection efficiency of photon counting detectors. In order to facilitate it, a switched integrating amplifier-based photocurrent meter that can measure photocurrent down to 100 femto ampere level was developed. The photon counting detector under test with a fiber-coupled input is directly compared with a reference photodiode without using any calibrated attenuator. -

Investigation of Photon Counting Pixel Detectors for X-Ray Spectroscopy and Imaging
Investigation of photon counting pixel detectors for X-ray spectroscopy and imaging Der Naturwissenschaftlichen Fakult¨at der Friedrich-Alexander-Universit¨at Erlangen-Nurnberg¨ zur Erlangung des Doktorgrades Dr.rer.nat. vorgelegt von Patrick Takoukam Talla aus Yaounde/Kamerun Als Dissertation genehmigt von der Naturwissen- schaftlichen Fakult¨at der Universit¨at Erlangen-Nurnberg¨ Tag der mundlichen¨ Prufung:¨ 07. April 2011 Vorsitzender der Promotionskommission: Prof. Dr. Rainer Fink Erstberichterstatter: Prof. Dr. Gisela Anton Zweitberichterstatter: Prof. Dr. Valeria Rosso Dedication To my wife Sandrine Takoukam Talla To my parents Jean Baptiste Talla and Monique Talla To my late brother Guy Bertrand Wafeu Talla i Contents 1 Introduction 1 2 Interaction of X-rays with Matter 3 2.1 PhotoelectricEffect. .. .. .. .. .. .. .. .. .. .. 3 2.2 ComptonScattering .............................. 4 2.3 RayleighScattering. .. .. .. .. .. .. .. .. .. .. 5 2.4 PairProduction ................................ 5 2.5 Interaction of Electrons with Matter . ..... 6 2.6 Conclusion ................................... 7 3 The Medipix2 Detector 9 3.1 Description and operating Modes . ... 9 3.2 CountingPrinciple ............................... 11 3.3 ChargeSharing................................. 12 3.4 Conclusion ................................... 15 4 The Medipix3 Detector 17 4.1 Motivation ................................... 17 4.2 Description ................................... 18 4.3 Functionalities and operating Modes . ..... 20 4.4 ChargeSummingMode ...........................