The Rationale for Family Planning in the Former Soviet Union Evidence from Europe, Eurasia, and the US
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cyproterone Art. 31
Приложение I Списък на лекарствените продукти и форми 1 Държава членка Притежател на Наименование на INN/Активно Фармацевтична Начин на (ЕИП) разрешението за продукта вещество + форма приложение употреба Количество на активното вещество (в дозова единица) Австрия Bayer Austria Gmbh Androcur Depot Cyproterone Acetate Инжекционен Интрамускулно 300mg/3ml разтвор приложение Австрия Bayer Austria Gmbh Climen Cyproterone Acetate 1mg Обвита таблетка Перорално таблетка, Estradiol приложение Valerate 2mg таблетка| Estradiol Valerate 2mg таблетка Австрия Bayer Austria Gmbh Climen 28-Tage Cyproterone Acetate 1mg Обвита таблетка Перорално таблетка, Estradiol приложение Valerate 2mg таблетка| Estradiol Valerate 2mg таблетка Австрия Bayer Austria Gmbh Diane Mite Cyproterone Acetate 2mg Обвита таблетка Перорално таблетка, Ethinylestradiol приложение 35μg таблетка Австрия Bayer Austria Gmbh Minerva Cyproterone Acetate 2mg Обвита таблетка Перорално таблетка, Ethinylestradiol приложение 0,035mg таблетка Австрия Bayer Austria Gmbh Andro-Diane Cyproterone Acetate Таблетка Перорално 10mg таблетка приложение Австрия Bayer Austria Gmbh Androcur Cyproterone Acetate Таблетка Перорално 100mg таблетка приложение Австрия Bayer Austria Gmbh Androcur Cyproterone Acetate Таблетка Перорално 50mg таблетка приложение Австрия Gynial Gmbh Alisma Cyproterone Acetate 2mg Филмирана таблетка Перорално таблетка, Ethinylestradiol приложение 35μg таблетка 2 Държава членка Притежател на Наименование на INN/Активно Фармацевтична Начин на (ЕИП) разрешението за продукта вещество + -

CEE Bulletin on Sexual and Reproductive Health and Rights No
CEE Bulletin on Sexual and Reproductive Health and Rights No 07 (186) 2019 Table of contents: Burning Issue Regional Updates From ASTRA members Resources Upcoming events BURNING ISSUE World Health Organisation (WHO) launches a new set of guidelines on self-care interventions for sexual and reproductive health and rights Self-care consisting of self-testing, self- diagnosis, self-management, self-medication, self-monitoring and self-educating is said to be able to reshape global and national health systems. Understood as an opportunity to promote autonomous decisions of a patient and support for a person-centered approach, self-care interventions allow people across the world to protect their health without the need of visiting a medical professional when it is not necessary for providing oneself with successful treatment. The publication offers solutions and guidelines that will help meet the Sustainable Development Goals, while assuring access to proper medical care to everyone, including representatives of underprivileged groups, inhabitants of the Global South region and people that struggle to find a medical professional in their vicinity. The document is WHO’s first set of consolidated guidelines - it shifts its approach to healthcare to a more patient-focused. The first edition of guidelines tackles topics related to sexual and reproductive health, presenting evidence-based recommendations on interventions for maternal health, contraception, cervical cancer, fertility and STIs, including HIV and safe abortion. Full document can be accessed here. Source: WHO REGIONAL UPDATES Council of Europe Commissioner for Human Rights report on Poland Commissioner Dunja Mijatović and her team visited Poland from 11 to 15 March 2019. -

Aldosterone Enhances Renal Calcium Reabsorption by Two Types of Channels
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Kidney International, Vol. 66 (2004), pp. 242–250 Aldosterone enhances renal calcium reabsorption by two types of channels MARIE LECLERC,MICHELE` G. BRUNETTE, and DENIS COUCHOUREL Maisonneuve-Rosemont Hospital and University of Montreal, Canada Aldosterone enhances renal calcium reabsorption by two types transepithelial potential difference in the late segments of channels. of the nephron, reflecting a stimulation of the amiloride- Background. Aldosterone has been known for many years + + sensitive Na transport by the apical membranes. to increase sodium (Na ) reabsorption by the distal nephron. The present in vitro experiments investigated the effect of the In contrast to the abundant literature dealing with the + hormone on calcium (Ca2 ) transport by the luminal membrane antinatriuretic effect of aldosterone, data concerning its + of the rabbit nephron, independent of any systemic influence. action on Ca2 transport are relatively scarce. Clearance Methods. Proximal and distal tubules were incubated with studies showed either an increase in calciuria [2] or an + either aldosterone or the carrier. The luminal membranes of absence of significant change of Ca2 excretion [3, 4] af- these tubules were purified, vesiculated, and 45Ca uptake by these vesicles was subsequently measured. ter aldosterone administration. In a randomized study in Results. Treatment of the distal tubules with 10−8 mol/L al- male volunteers, Van Hamersvelt et al [5] compared the + + dosterone enhanced both 0.1 and 0.5 mmol/L Ca2 transport. effect of the Ca2 channel blocker felodipine, alone or The hormone action was abolished by tyrosine kinase inhibitors. -

Abortion Rates
MEASURE DHS assists countries worldwide in the collection and use of data to monitor and evaluate population, health, and nutrition programs. Funded by the U.S. Agency for International Development (USAID), MEASURE DHS is implemented by ORC Macro in Calverton, Maryland. The main objectives of the MEASURE DHS project are: 1) to provide decisionmakers in survey countries with information useful for informed policy choices, 2) to expand the international population and health database, 3) to advance survey methodology, and 4) to develop in participating countries the skills and resources necessary to conduct high-quality demographic and health surveys. Information about the MEASURE DHS project or the status of MEASURE DHS surveys is available on the Internet at http://www.measuredhs.com or by contacting: ORC Macro 11785 Beltsville Drive, Suite 300 Calverton, MD 20705 USA Telephone: 301-572-0200 Fax: 301-572-0999 E-mail: [email protected] DHS Analytical Studies No. 8 Recent Trends in Abortion and Contraception in 12 Countries Charles F. Westoff Office of Population Research Princeton University ORC Macro Calverton, Maryland, USA February 2005 This publication was made possible through support provided by the U.S. Agency for Interna- tional Development under the terms of Contract No. HRN-C-00-97-00019-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the U.S. Agency for International Development Suggested citation: Westoff, Charles F. 2005. Recent Trends in Abortion and Contraception -

Abortion and Modern Contraception Are Substitutes
IZA DP No. 9809 Population Policy: Abortion and Modern Contraception Are Substitutes Grant Miller Christine Valente March 2016 DISCUSSION PAPER SERIES Forschungsinstitut zur Zukunft der Arbeit Institute for the Study of Labor Population Policy: Abortion and Modern Contraception Are Substitutes Grant Miller Stanford University and NBER Christine Valente University of Bristol and IZA Discussion Paper No. 9809 March 2016 IZA P.O. Box 7240 53072 Bonn Germany Phone: +49-228-3894-0 Fax: +49-228-3894-180 E-mail: [email protected] Any opinions expressed here are those of the author(s) and not those of IZA. Research published in this series may include views on policy, but the institute itself takes no institutional policy positions. The IZA research network is committed to the IZA Guiding Principles of Research Integrity. The Institute for the Study of Labor (IZA) in Bonn is a local and virtual international research center and a place of communication between science, politics and business. IZA is an independent nonprofit organization supported by Deutsche Post Foundation. The center is associated with the University of Bonn and offers a stimulating research environment through its international network, workshops and conferences, data service, project support, research visits and doctoral program. IZA engages in (i) original and internationally competitive research in all fields of labor economics, (ii) development of policy concepts, and (iii) dissemination of research results and concepts to the interested public. IZA Discussion Papers often represent preliminary work and are circulated to encourage discussion. Citation of such a paper should account for its provisional character. A revised version may be available directly from the author. -
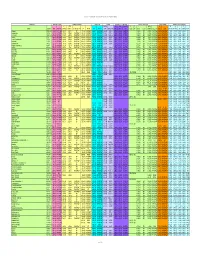
Chemical-Specific Parameters Supporting Table May 2016 Analyte
Regional Screening Level (RSL) Chemical-specific Parameters Supporting Table May 2016 Contaminant Molecular Weight Volatility Parameters Melting Point Density Diffusivity in Air and Water Partition Coefficients Water Solubility Tapwater Dermal Parameters H` (atm- Density Dia Diw Dia and Diw Kd Kd Koc log Kow S B τevent t* Kp 3 3 2 2 Analyte CAS No. MW MW Ref (unitless) m /mole) H` and HLC Ref VP VP Ref MP MP Ref (g/cm ) Density Ref (cm /s) (cm /s) Ref (L/kg) Ref (L/kg) Koc Ref (unitless) log Kow Ref (mg/L) S Ref (unitless) (hr/event) (hr) (cm/hr) K Ref Acephate 30560-19-1 1.8E+02 PHYSPRO 2.0E-11 5.0E-13 EPI 1.7E-06 PHYSPROP 8.8E+01 PHYSPROP 1.4E+00 CRC89 3.7E-02 8.0E-06 WATER9 1.0E+01 EPI -8.5E-01 PHYSPRO 8.2E+05 PHYSPROP 2.1E-04 1.1E+00 2.7E+00 4.0E-05 EPI Acetaldehyde 75-07-0 4.4E+01 PHYSPRO 2.7E-03 6.7E-05 PHYSPROP 9.0E+02 PHYSPROP -1.2E+02 PHYSPROP 7.8E-01 CRC89 1.3E-01 1.4E-05 WATER9 1.0E+00 EPI -3.4E-01 PHYSPRO 1.0E+06 PHYSPROP 1.3E-03 1.9E-01 4.5E-01 5.3E-04 EPI Acetochlor 34256-82-1 2.7E+02 PHYSPRO 9.1E-07 2.2E-08 PHYSPROP 2.8E-05 PHYSPROP 1.1E+01 PubChem 1.1E+00 PubChem 2.2E-02 5.6E-06 WATER9 3.0E+02 EPI 3.0E+00 PHYSPRO 2.2E+02 PHYSPROP 3.1E-02 3.4E+00 8.2E+00 5.0E-03 EPI Acetone 67-64-1 5.8E+01 PHYSPRO 1.4E-03 3.5E-05 PHYSPROP 2.3E+02 PHYSPROP -9.5E+01 PHYSPROP 7.8E-01 CRC89 1.1E-01 1.2E-05 WATER9 2.4E+00 EPI -2.4E-01 PHYSPRO 1.0E+06 PHYSPROP 1.5E-03 2.2E-01 5.3E-01 5.1E-04 EPI Acetone Cyanohydrin 75-86-5 8.5E+01 PHYSPRO 8.1E-08 2.0E-09 PHYSPROP 3.4E-01 PHYSPROP -1.9E+01 PHYSPROP 9.3E-01 CRC89 8.6E-02 1.0E-05 WATER9 1.0E+00 -
Environmental Health Criteria 206 Methyl Tertiary-Butyl Ether -J
INTERNATIONAL PROGRAMME ON CHEMICAL SAFETY Environmental Health Criteria 206 Methyl tertiary-Butyl Ether -J. l \r LNTER-ORGAN1ZATON PROGRAMME FOR THE SOUND MANAGEMENT OF CHEMICALS I JiVJ A cooperative agreement among UNEP, ILO, FAO, WHO, UNIDO, UNITAR and OECD THE ENVIRONMENTAL HEALTH CRITERIA SERIES Acetaldehyde (No. 167, 1995) Chiorofluorocarbons, partially halogenated Acetonitrile (No. 154, 1993) (ethane derivatives) (No. 139, 1992) Acrolein (No. 127, 1991) (methane derivatives) (No. 126, 1991) Acrylamide (No. 49, 1985) Chloroform (No. 163, 1994) Acrylic acid (No. 191, 1997) Chlorophenols (No. 93, 1989) Acrylonitrile (No. 28, 1983) Chlorothalonil (No. 183, 1996) Aged population, principles for evaluating Chromium (No. 61, 1988) the effects of chemicals (No. 144, 1992) Chrysotile asbestos (No. 203, 1998) Aldicarb (No. 121, 1991) Copper (No. 200, 1998) Aldrin and dieldrin (No. 91, 1989) Cresols (No. 168, 1995) Allethrins (No. 87, 1989) Cyhalothrin (No. 99, 1990) Aluminium (No. 194, 1997) Cypermethrin (No. 82, 1989) Amitrole (No. 158, 1994) Cypermethrin, alpha- (No. 142, 1992) Ammonia (No. 54, 1986) DOT and its derivatives (No. 9, 1979) Anticoagulant rodenticides (No. 175, 1995) DOT and its derivatives - Arsenic (No. 18, 1981) environmental aspects (No, 83, 1989) Asbestos and other natural mineral fibres Deltamethrjn (No. 97, 1990) (No. 53, 1986) Demeton-S-methyl (No. 197, 1997) Barium (No. 107, 1990) Diaminotoluenes (No. 74, 1987) Benomyl (No. 148, 1993) Diazinon (No. 198, 1997) Benzene (No. 150, 1993) 1,2-Dibromoethane (No. 177, 1996) Beryllium (No. 106, 1990) Oi-n-butyl phthalate (No. 189, 1997) Biomarkers and risk assessment: concepts 1 ,2-Dichloroethane and principles (No. 155, 1993) (No. 62, 1987, 1St edition) Blotoxins, aquatic (marine and freshwater) (No. -

Reasons for Women to Terminate a Pregnancy: a Qualitative Study
University of Pretoria etd – Badenhorst, R (2005) Reasons for Women to Terminate a Pregnancy: a Qualitative Study by Ronel Badenhorst Student Number: 9143998 Submitted in partial fulfillment of the requirements for the degree Magister Artium (Demography) In the Faculty of Humanities Department of Sociology University of Pretoria July 2005 Supervisor: Dr M de Waal University of Pretoria etd – Badenhorst, R (2005) TABLE OF CONTENT Page number CHAPTER 1: ORIENTATION AND BACKGROUND 1.1. Introduction 1 1.2. Abortion Legislation 2 1.3. The International Arena 4 1.4. South African Liberalisation 6 1.5. South African Legislation 7 1.6. Rationale for the study and Problem Statement 8 1.7. Aim of the study 10 1.8. Delimitations of the study 10 1.9. Limitations of the study 10 1.10. Assumptions 11 1.11. Research Methodology 12 1.12. Summary 13 1.13. Chapter Layout 13 CHAPTER 2: LITERATURE REVIEW 2.1. Introduction 15 2.2. Reasons for women choosing to terminate a pregnancy 15 2.2.1. Contraception 20 2.2.2. HIV/AIDS 21 2.3. Ethical Considerations 26 2.4. Feminist Framework 30 2.5. Historical Perspective 35 i University of Pretoria etd – Badenhorst, R (2005) Page number 2.6. Human rights and Reproductive rights 38 2.6.1. The World Population Conference, Bucharest, 1974 39 2.6.2. The International Conference on Population, Mexico City, 1984 39 2.6.3. The International Conference on Population and Development, Cairo, 40 1994 2.7. South African Population Policies 44 2.8. Abortion Legislation 48 2.8.1. -

Lessons Without Borders Increased Health Risks, but When the Procedure Is Performed in an Appro- by Susan A
Issues & Implications involved in making travel arrange- ments and gathering the necessary Envisioning Life Without Roe: funds beyond just the medical costs. Abortion later in pregnancy carries Lessons Without Borders increased health risks, but when the procedure is performed in an appro- By Susan A. Cohen priate setting by a trained medical professional, those risks are still low. And they pale in comparison to the risks millions of women in develop- Abortion has been legal nationwide professional to safely perform an ille- ing countries take every day in hav- in the United States for 30 years. gal procedure. In those states that ing an illegal abortion. Statistics as well as the personal permitted abortion under very nar- accounts of physicians and women row circumstances, some were able Of the 46 million abortions occur- who are now grandmothers tell the to persuade hospital authorities that ring worldwide each year, 20 million tale of hardship, injury and death they fit the criteria. New York legal- are illegal. As was the case with due to American women’s under- ized abortion, without a residency affluent U.S. women in the years ground recourse to illegal, septic requirement, in 1970, which imme- before Roe, a small proportion of procedures in an earlier time. These diately put New York City on the women living in urban areas in some provide an important context for the map as an option for those women developing countries may be able to current debate over the future of who could afford to travel. Before afford the services of a private physi- legal abortion in the United States— that, it was an open secret that afflu- cian who can perform a safe, if still but the fact remains that the coun- ent American women would travel to illegal, abortion. -

TOXICOLOGICAL PROFILE for METHYL Tert-BUTYL ETHER
TOXICOLOGICAL PROFILE FOR METHYL tert-BUTYL ETHER U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Agency for Toxic Substances and Disease Registry August 1996 METHYL tert-BUTYL ETHER ii DISCLAIMER The use of company or product name(s) is for identification only and does not imply endorsement by the Agency for Toxic Substances and Disease Registry. METHYL tert-BUTYL ETHER iii UPDATE STATEMENT Toxicological profiles are revised and republished as necessary, but no less than once every three years. For information regarding the update status of previously released profiles, contact ATSDR at: Agency for Toxic Substances and Disease Registry Division of Toxicology/Toxicology Information Branch 1600 Clifton Road NE, E-29 Atlanta, Georgia 30333 vi *Legislative Background The toxicological profiles are developed in response to the Superfund Amendments and Reauthorization Act (SARA) of 1986 (Public Law 99-499) which amended the Comprehensive Environmental Response, Compensation, and Liability Act of 1980 (CERCLA or Superfund). This public law directed ATSDR to prepare toxicological profiles for hazardous substances most commonly found at facilities on the CERCLA National Priorities List and that pose the most significant potential threat to human health, as determined by ATSDR and the EPA. The availability of the revised priority list of 275 hazardous substances was announced in the Federal Register on April 29, 1996 (61 FR 18744). For prior versions of the list of substances, see Federal Register notices dated April 17, 1987 (52 FR 12866); October 20, 1988 (53 FR 41280); October 26, 1989 (54 FR 43619); October 17, 1990 (55 FR 42067); October 17, 199l (56 FR 52166); October 28, 1992 (57 FR 48801); and February 28, 1994 (59 FR 9486). -

The Effect of Dosing Regimen on Outcomes of Vitamin D Supplementation Trials a Study of Current Literature
Faculty of Medicine The effect of dosing regimen on outcomes of vitamin D supplementation trials A study of current literature — Anette Uhlving Larsen Master thesis in Medicine (MED-3950) June 2019 Supervisor: Professor Rolf Jorde, Institute of Clinical Medicine Abstract Results from observational studies have indicated associations between vitamin D and extra- skeletal outcomes, including respiratory tract infections (RTI) and all-cause mortality. However, available trial-data have shown inconsistent results. The main objective of this thesis was to investigate whether a beneficial effect of daily supplementation of vitamin D on RTI and all-cause mortality could have been masked by the use of less frequent supplementation intervals. This thesis included data from double-blinded, randomized controlled trials (RCTs) published in the last 10 years. Eligible trials were identified through screening of the reference lists of systematic reviews of meta-analyses (MAs), and of reference lists of MAs on the selected outcomes included in these reviews. Also, additional searches were performed to ensure that also recently published RCTs, not identified in a previous step of the search strategy, were considered for inclusion. The search strategy was designed to promote selection of trials of adequate methodological quality. To be included the record had to be written in English and report results of a double-blinded placebo-controlled RCT with vitamin D supplementation in a human population. Studies including pregnant women or assessing the effect of prenatal supplementation were not included, nor were studies including populations with chronic kidney disease and/or other diseases known to affect the conversion of active metabolites of vitamin D. -

Abortion and Contraception in Georgia and Kazakhstan
ABORTION AND CONTRACEPTION IN GEORGIA AND KAZAKHSTAN Suzanne Olds Charles F. Westoff ACKNOWLEDGEMENTS This project was supported by the Open Society Institute—New York, in collaboration with Open Society Georgia Foundation. We would also like to thank the many individuals who provided information and insights. (Their names are cited in Appendix A.) 2 TABLE OF CONTENTS Executive Summary 4 Introduction 7 Georgia 8 Kazakhstan 28 Comparison Findings: 1995 to1999 35 Appendix A: List of Individuals Interviewed and Documents Reviewed 40 Appendix B: Supply Side Data Collection Framework 46 3 EXECUTIVE SUMMARY The 1999 “Reproductive Health Survey, Georgia” indicates that Georgia has a very high rate of legal abortion and low use of modern contraception. (A second survey will be conducted in 2005.) To explore contributing causes and factors and to develop critical recommendations for the Government of Georgia and health and population donor organizations, the Open Society Institute’s Network Public Health Programs sponsored, in collaboration with the Open Society Georgia Foundation, a report on Abortion and Contraception in Georgia and Kazakhstan in 2004. Key Findings While half of all Georgian women consider abortion a health risk, nearly 80 percent feel women should have the right to decide about her pregnancy, including the option of abortion. Some reasons for the high abortion rate in Georgia are: • A long reliance on abortion as birth control in the Soviet Union due to isolation from the development of modern, safe, and effective contraception elsewhere in the world; • An inadequate supply of government funded contraceptives due to high costs; • Attitudes and practices of the medical profession that favor abortion; • A health-care system that favors curative, high-level institutional care and procedures over a preventive health approach that includes family planning at the primary care level.