Diseases of the Musculoskeletal System and Connective Tissue
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

19-0603 ) Issued: January 28, 2020 DEPARTMENT of the TREASURY, ) INTERNAL REVENUE SERVICE, ) Holtsville, NY, Employer ) ______)
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) S.L., Appellant ) ) and ) Docket No. 19-0603 ) Issued: January 28, 2020 DEPARTMENT OF THE TREASURY, ) INTERNAL REVENUE SERVICE, ) Holtsville, NY, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Thomas S. Harkins, Esq., for the appellant1 Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge ALEC J. KOROMILAS, Alternate Judge VALERIE D. EVANS-HARRELL, Alternate Judge JURISDICTION On January 18, 2019 appellant, through counsel, filed a timely appeal from a July 26, 2018 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act2 (FECA) and 20 C.F.R. §§ 501.2(c) and 501.3, the Board has jurisdiction over the merits of this case.3 1 In all cases in which a representative has been authorized in a matter before the Board, no claim for a fee for legal or other service performed on appeal before the Board is valid unless approved by the Board. 20 C.F.R. § 501.9(e). No contract for a stipulated fee or on a contingent fee basis will be approved by the Board. Id. An attorney or representative’s collection of a fee without the Board’s approval may constitute a misdemeanor, subject to fine or imprisonment for up to one year or both. Id.; see also 18 U.S.C. § 292. Demands for payment of fees to a representative, prior to approval by the Board, may be reported to appropriate authorities for investigation. 2 5 U.S.C. -

Neck and Headache Pain
Neck and Headache Pain ICD-9-CM code: 723.2 cervicocranial syndrome ICF codes: Activities and Participation Domain code: d4158 Maintaining a body position, other specified - specified as: maintaining the head in a flexed position, such as when reading a book; or, maintaining the head in an extended position, such as when looking up at a computer screen or video monitor Body Structure codes: s7103 Joints of head and neck region Body Functions code: b28010 Pain in head and neck Common Historical Findings: Unilateral neck pain with referral to occipital, temporal, parietal, frontal or orbital areas Headache precipitated or aggravated by neck movements or sustained positions Noncontinuous headaches (usually < 1 episode/day; < 2 episodes/week) Common Impairment Findings - Related to the Reported Activity Limitation or Participation Restrictions: Observable postural asymmetry of the head on neck (sidebent or extended) Headache reproduced with provocation of the involved segmental myofascia and/or joints O/C1, C1/C2, or C2/C3 restricted accessory motions with associated myofascial trigger points Physical Examination Procedures: Palpation/Provocation of Suboccipital Myofascia Joe Godges DPT, MA, OCS 1 KP So Cal Ortho PT Residency O/C1, C1/C2, or C2/C3 accessory motion testing using posterior-to-anterior pressures 0/C1 accessory motion testing using C1 lateral translatoty pressures C1 – C2 Rotation ROM testing with the C2 – C7 segments in flexion Joe Godges DPT, MA, OCS 2 KP So Cal Ortho PT Residency Neck and Headache Pain: Description, Etiology, Stages, and Intervention Strategies The below description is consistent with descriptions of clinical patterns associated with the term “Cervicogenic Headache.” Description: Cervicogenic headache is a headache where the source of the ache is from a structure in the cervical spine, such as a cervical facet, muscle, ligament, or dura. -

Patellofemoral Pain Syndrome and Chondromalacia: the Effect of Ozone on Pain, Function and Quality of Life. a Non-Randomized Control-Trial
Central JSM Physical Medicine and Rehabilitation Bringing Excellence in Open Access Research Article *Corresponding author Marcos Edgar Fernández-Cuadros, Calle del Ánsar, 44, piso Segundo, CP 28047, Madrid, Spain, Tel: Patellofemoral Pain Syndrome 34-620314558; Email: [email protected]; Submitted: 23 November 2016 and Chondromalacia: The Effect Accepted: 05 December 2016 Published: 06 December 2016 of Ozone on Pain, Function Copyright © 2016 Fernández-Cuadros et al. and Quality of Life. A Non- OPEN ACCESS Keywords Randomized Control-Trial • Patellofemoral pain syndrome • Chondromalacia Marcos Edgar Fernández-Cuadros1,2*, Olga Susana Pérez-Moro1, • Pain and María Jesús Albaladejo-Florin1 • Ozone therapy • Quality of life 1Servicio de Rehabilitación, Hospital Universitario Santa Cristina, Spain 2de Rehabilitación, Fundación, Hospital General Santísima Trinidad, Spain Abstract Objectives: 1) To demonstrate the effectiveness of a treatment protocol with Ozone therapy on pain, function and quality of life in patients with Patellofemoral Pain Syndrome (PFPS) and Chondromalacia; and 2) to apply Ozone as a conservative treatment option with a demonstrable level of scientific evidence. Material and Methods: Prospective quasi-experimental before-after study (non-randomized control-trial) on 41 patients with PFPS and Chondromalacia grade 2 or more, who attended to Santa Cristina’s University Hospital, from January 2012 to November 2016 The protocol consisted of an intra articular infiltration of a medical mixture of Oxygen-Ozone (95% -5%) 20ml, at a 20ug / ml concentration, and a total number of 4 sessions (1 per week). Pain and quality of life were measured by Visual Analogical Scale (VAS) and Western Ontario and Mc Master Universities Index for Osteoarthritis (WOMAC) at the beginning / end of treatment. -

SODIUM HYALURONATE Policy Number: PHARMACY 059.37 T2 Effective Date: April 1, 2018
UnitedHealthcare® Oxford Clinical Policy SODIUM HYALURONATE Policy Number: PHARMACY 059.37 T2 Effective Date: April 1, 2018 Table of Contents Page Related Policies INSTRUCTIONS FOR USE .......................................... 1 Autologous Chondrocyte Transplantation in the CONDITIONS OF COVERAGE ...................................... 1 Knee BENEFIT CONSIDERATIONS ...................................... 2 Unicondylar Spacer Devices for Treatment of Pain COVERAGE RATIONALE ............................................. 2 or Disability APPLICABLE CODES ................................................. 4 DESCRIPTION OF SERVICES ...................................... 5 CLINICAL EVIDENCE ................................................. 5 U.S. FOOD AND DRUG ADMINISTRATION ................... 10 REFERENCES .......................................................... 12 POLICY HISTORY/REVISION INFORMATION ................ 14 INSTRUCTIONS FOR USE This Clinical Policy provides assistance in interpreting Oxford benefit plans. Unless otherwise stated, Oxford policies do not apply to Medicare Advantage members. Oxford reserves the right, in its sole discretion, to modify its policies as necessary. This Clinical Policy is provided for informational purposes. It does not constitute medical advice. The term Oxford includes Oxford Health Plans, LLC and all of its subsidiaries as appropriate for these policies. When deciding coverage, the member specific benefit plan document must be referenced. The terms of the member specific benefit plan document [e.g., -

A Thesis Submitted in Partial Fulfilment of the Requirements for the Degree of Doctor of Philosophy
MYOFASCIAL TRIGGER POINTS AND INNERVATION ZONE LOCATIONS IN UPPER TRAPEZIUS MUSCLES MARCO BARBERO A thesis submitted in partial fulfilment of the requirements for the degree of Doctor of Philosophy QUEEN MARGARET UNIVERSITY 2016 1 ABSTRACT Myofascial pain syndrome is characterized by sensory, motor and autonomic symptoms, and a myofascial trigger point (MTrP) is considered the principal clinical feature. Clinicians recognise myofascial pain syndrome as an important clinical entity but many basic and clinical issues need further research. Electrophysiological studies indicate that abnormal electrical activity is detectable near MTrPs. This phenomenon has been described as endplate noise and it has been purported to be associated MTrP pathophysiology. Authors also suggest that MTrPs are located in the innervation zone (IZ) of muscles. The aim of this thesis was to describe both the location of MTrP and the IZ’ locations in the upper trapezius muscle. The hypothesis was that distance between the IZ and the MTrP in upper trapezius muscle is equal to zero. This thesis includes two preliminary studies. The first one address the reliability of surface electromyography (EMG) in locating the IZ in upper trapezius muscle, and the second one address the reliability of a manual palpation protocol in locating the MTrP in upper trapezius muscle. The intra- rater reliability of surface EMG in locating the IZ was almost perfect; with Kappa = 0.90 for operator A and Kappa = 0.92 for operator B. Also the inter- rater reliability showed an almost perfect agreement, with Kappa = 0.82. Both the operators conducted 900 estimations of IZ’ location through visual analysis of the EMG signals. -

Lameness in Fattening Pigs – Mycoplasma Hyosynoviae, Osteochondropathy and Reduced Dietary Phosphorus Level As Three Infuencing Factors: a Case Report
Lameness in fattening pigs – Mycoplasma hyosynoviae, osteochondropathy and reduced dietary phosphorus level as three inuencing factors: A case report Birte Wegner Veterinary Practice Duemmerland Jörg Tenhündfeld Vetland Dr. Tenhündfeld & Kollegen Johanna Vogels Stiftung Tierarztliche Hochschule Hannover Marius Beumer Stiftung Tierarztliche Hochschule Hannover Josef Kamphues Stiftung Tierarztliche Hochschule Hannover Florian Hansmann Stiftung Tierarztliche Hochschule Hannover Hanna Rieger Stiftung Tierarztliche Hochschule Hannover Elisabeth grosse Beilage Stiftung Tierarztliche Hochschule Hannover Isabel Hennig-Pauka ( [email protected] ) University of Veterinary Medicine Hannover https://orcid.org/0000-0003-3994-5979 Case report Keywords: Locomotor disorder, mineral supply, Mycoplasma hyosynoviae, nutrition, swine Posted Date: September 25th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-35962/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/28 Version of Record: A version of this preprint was published on December 15th, 2020. See the published version at https://doi.org/10.1186/s40813-020-00184-w. Page 2/28 Abstract Background: Multiple diagnostic procedures, their results and interpretation in a case with severe lameness in fattening pigs are described. It is shown that selected diagnostic steps lead to identication of various risk factors for disease development in the affected herd. One focus of this case report is the prioritization of diagnostic steps to verify the impact of the different conditions, which nally led to the clinical disorder. Disease is the consequence of previously acting factors, and the involved diagnostic institute is the last stage in the timeline. Some diagnostic ndings might therefore no longer be signicant. -

Absolute Risk, 252 Acetabular Dysplasia, 38, 211, 213 Acetabular Protrusion, 38 Achondroplasia, 195, 197, 199–200, 205 Genetic
Cambridge University Press 978-0-521-86137-3 - Palaeopathology Tony Waldron Index More information Index absolute risk, 252 angular kyphosis acetabular dysplasia, 38, 211, 213 in Scheuermann’s disease, 45 acetabular protrusion, 38 in tuberculosis, 93–4 achondroplasia, 195, 197, 199–200, 205 ankylosing spondylitis, 57–60, 65 genetic defect in, 199 ankylosis in, 58 skeletal changes in, 200 bamboo spine in, 59 acoustic neuroma, 229–31 erosions in, 59 acromegaly, 78, 207–8 first description, 57 and DISH, 208 HLA B27 58 and, skeletal changes in, 208 operational definition of, 59 acromelia, 198 prevalence of, 58 aDNA sacroiliitis and, 59 in leprosy, 101 skip lesions in, 59 in syphilis, 108 ankylosis, 51 in tuberculosis, 92, 95–6 following fracture, 146 Albers-Schonberg˝ disease, see in ankylosing spondylitis, 58 osteopetrosis in brucellosis, 96 Alstrom syndrome, 78 in DISH, 73 alveolar margin, see periodontal disease in erosive osteoarthritis, 55 amputation, 158–61 in rheumatoid arthritis, 51 indications for, 160–1 in septic arthritis, 89 ancient DNA, see aDNA in tuberculosis, 93–4 anaemia, 136–7 annulus fibrosus, 42–3, 45 cribra obitalia and, 136–7 ante-mortem tooth loss, 238–9 aneurysms, 224–7 and periodontal disease, 238–9 aortic, 224–5 and scurvy, 132 and syphilis, 224 causes of, 238 of vertebral artery, 225–6 anterior longitudinal ligament popliteal, 226 in ankylosing spondylitis, 59 aneurysmal bone cyst, 177 in DISH, 73 angiosarcoma, 182 anti-CCP antibodies, 49, 53 © Cambridge University Press www.cambridge.org Cambridge University Press -

Non-Cardiac Manifestations of Marfan Syndrome
Keynote Lecture Series Non-cardiac manifestations of Marfan syndrome Anne H. Child Molecular and Clinical Sciences Research Institute, St George’s University of London, Cranmer Terrace, London, UK Correspondence to: Dr. Anne H. Child, MD, FRCP. Reader in Cardiovascular Genetics, Molecular and Clinical Sciences Research Institute, St George's University of London, Cranmer Terrace, London SW17 0RE, UK. Email: [email protected]. Because of the widespread distribution of fibrillin 1 in the body, Marfan syndrome (MFS) affects virtually every system. The expression of this single dominantly inherited gene is variable within a family, and between families. There is some genotype-phenotype correlation which is helpful in guiding long-term prognosis, and management. In general gene mutations have been reported in clusters, with those having mainly ocular manifestations occurring in exons 1 to 15 of this 65-exon gene; those causing cardiac problems often involving cysteine replacement in a calcium binding EGF-like sequence; the most severe mutations occurring in exons 25–32, causing neonatal MFS diagnosed at birth, and severe enough to cause death frequently before the age of 2. Other correlations will certainly be found in future. This condition is progressive, and the manifestations unfold according to age. For example, if the lens is going to dislocate this usually occurs by age 10; scoliosis usually presents itself between the ages of 8 and 15; height should be monitored carefully between the onset of puberty and cessation of growth approximately age 17 or 18. Holistic care should be offered by one doctor who oversees the patient’s welfare. This should be a paediatrician, paediatric cardiologist, or general practitioner in the case of an affected child. -

Frequency and Criticality of Diagnoses in Family Medicine Practices: from the National Ambulatory Medical Care Survey (NAMCS)
J Am Board Fam Med: first published as 10.3122/jabfm.2018.01.170209 on 12 January 2018. Downloaded from ORIGINAL RESEARCH Frequency and Criticality of Diagnoses in Family Medicine Practices: From the National Ambulatory Medical Care Survey (NAMCS) Michael R. Peabody, PhD, Thomas R. O’Neill, PhD, Keith L. Stelter, MD, MMM, and James C. Puffer, MD Background: Family medicine is a specialty of breadth, providing comprehensive health care for the individual and the family that integrates the broad scope of clinical, social, and behavioral sciences. As such, the scope of practice (SOP) for family medicine is extensive; however, over time many family phy- sicians narrow their SOP. We sought to provide a nationally representative description of the most com- mon and the most critical diagnoses that family physicians see in their practice. Methods: Data were extracted from the 2012 National Ambulatory Medical Care Survey (NAMCS) to select all ICD-9 codes reported by family physicians. A panel of family physicians then reviewed 1893 ICD-9 codes to place each code into an American Board of Family Medicine Family Medicine Certifica- tion Examination test plan specifications (TPS) category and provide a rating for an Index of Harm (IoH). Results: An analysis of all 1893 ICD-9 codes seen by family physicians in the 2012 NAMCS found that 198 ICD-9 codes could not be assigned a TPS category, leaving 1695 ICD-9 codes in the dataset. Top 10 lists of ICD-9 codes by TPS category were created for both frequency and IoH. Conclusions: This study provides a nationally representative description of the most common diag- copyright. -
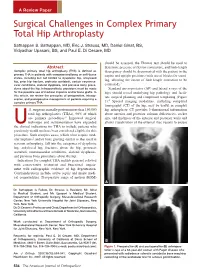
Surgical Challenges in Complex Primary Total Hip Arthroplasty
A Review Paper Surgical Challenges in Complex Primary Total Hip Arthroplasty Sathappan S. Sathappan, MD, Eric J. Strauss, MD, Daniel Ginat, BS, Vidyadhar Upasani, BS, and Paul E. Di Cesare, MD should be assessed, the Thomas test should be used to Abstract determine presence of flexion contracture, and limb-length Complex primary total hip arthroplasty (THA) is defined as discrepancy should be documented with the patient in the primary THA in patients with compromised bony or soft-tissue supine and upright positions (with use of blocks for stand- states, including but not limited to dysplastic hip, ankylosed hip, prior hip fracture, protrusio acetabuli, certain neuromus- ing, allowing the extent of limb-length correction to be 3 cular conditions, skeletal dysplasia, and previous bony proce- estimated). dures about the hip. Intraoperatively, provisions must be made Standard anteroposterior (AP) and lateral x-rays of the for the possible use of modular implants and/or bone grafts. In hips should reveal underlying hip pathology and facili- this article, we review the principles of preoperative, intraop- tate surgical planning and component templating (Figure erative, and postoperative management of patients requiring a 4 complex primary THA. 1). Special imaging modalities, including computed tomography (CT) of the hip, may be useful in complex .S. surgeons annually perform more than 150,000 hip arthroplasty. CT provides 3-dimensional information total hip arthroplasties (THAs), 90% of which about anterior and posterior column deficiencies, socket are primary procedures.1 Improved surgical size, and thickness of the anterior and posterior walls and technique and instrumentation have expanded allows visualization of the external iliac vessels to ensure Uthe clinical indications for THA to include patients who previously would not have been considered eligible for this procedure. -

Physical Examination of the Knee: Meniscus, Cartilage, and Patellofemoral Conditions
Review Article Physical Examination of the Knee: Meniscus, Cartilage, and Patellofemoral Conditions Abstract Robert D. Bronstein, MD The knee is one of the most commonly injured joints in the body. Its Joseph C. Schaffer, MD superficial anatomy enables diagnosis of the injury through a thorough history and physical examination. Examination techniques for the knee described decades ago are still useful, as are more recently developed tests. Proper use of these techniques requires understanding of the anatomy and biomechanical principles of the knee as well as the pathophysiology of the injuries, including tears to the menisci and extensor mechanism, patellofemoral conditions, and osteochondritis dissecans. Nevertheless, the clinical validity and accuracy of the diagnostic tests vary. Advanced imaging studies may be useful adjuncts. ecause of its location and func- We have previously described the Btion, the knee is one of the most ligamentous examination.1 frequently injured joints in the body. Diagnosis of an injury General Examination requires a thorough knowledge of the anatomy and biomechanics of When a patient reports a knee injury, the joint. Many of the tests cur- the clinician should first obtain a rently used to help diagnose the good history. The location of the pain injured structures of the knee and any mechanical symptoms were developed before the avail- should be elicited, along with the ability of advanced imaging. How- mechanism of injury. From these From the Division of Sports Medicine, ever, several of these examinations descriptions, the structures that may Department of Orthopaedics, are as accurate or, in some cases, University of Rochester School of have been stressed or compressed can Medicine and Dentistry, Rochester, more accurate than state-of-the-art be determined and a differential NY. -

Thieme: Teaching Atlas of Musculoskeletal Imaging
Teaching Atlas of Musculoskeletal Imaging Teaching Atlas of Musculoskeletal Imaging Peter L. Munk, M.D., C.M., F.R.C.P.C. Professor Departments of Radiology and Orthopaedics University of British Columbia Head Section of Musculoskeletal Radiology Vancouver General Hospital and Health Science Center Vancouver, British Columbia, Canada Anthony G. Ryan, M.B., B.C.H., B.A.O., F.R.C.S.I., M.Sc. (Engineering and Physical Sciences in Medicine), D.I.C., F.R.C.R., F.F.R.R.C.S.I. Consultant Musculoskeletal and Interventional Radiologist Waterford Regional Teaching Hospital Ardkeen, Waterford City, Republic of Ireland Radiologic Tutor and Clinical Instructor in Radiology The Royal College of Surgeons in Ireland Dublin, Republic of Ireland Thieme New York • Stuttgart [email protected] 66485438-66485457 Thieme Medical Publishers, Inc. 333 Seventh Ave. New York, NY 10001 Editor: Birgitta Brandenburg Assistant Editor: Ivy Ip Vice President, Production and Electronic Publishing: Anne T. Vinnicombe Production Editor: Print Matters, Inc. Vice President, International Marketing: Cornelia Schulze Sales Director: Ross Lumpkin Chief Financial Officer: Peter van Woerden President: Brian D. Scanlan Compositor: Compset, Inc. Printer: The Maple-Vail Book Manufacturing Group Library of Congress Cataloging-in-Publication Data Munk, Peter L. Teaching atlas of musculoskeletal imaging / Peter L. Munk, Anthony G. Ryan. p. ; cm. Includes bibliographical references and index. ISBN-13: 978-1-58890-372-3 (alk. paper) ISBN-10: 1-58890-372-9 (alk. paper) ISBN-13: 978-3-13-141981-1 (alk. paper) ISBN-10: 3-13-141981-4 (alk. paper) 1. Musculoskeletal system—Diseases—Imaging—Atlases. 2. Musculoskeletal system—Diseases—Case studies.