The Importance of Genetic Influences in Asthma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Long Noncoding Rnas in Lipid Metabolism
Long noncoding RNAs in lipid metabolism: literature review and conservation analysis across species Kévin Muret, Colette Désert, Laetitia Lagoutte, Morgane Boutin, Florence Gondret, Tatiana Zerjal, Sandrine Lagarrigue To cite this version: Kévin Muret, Colette Désert, Laetitia Lagoutte, Morgane Boutin, Florence Gondret, et al.. Long noncoding RNAs in lipid metabolism: literature review and conservation analysis across species. BMC Genomics, BioMed Central, 2019, 20, pp.882. 10.1186/s12864-019-6093-3. hal-02387579 HAL Id: hal-02387579 https://hal.archives-ouvertes.fr/hal-02387579 Submitted on 29 Nov 2019 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License Muret et al. BMC Genomics (2019) 20:882 https://doi.org/10.1186/s12864-019-6093-3 REVIEW Open Access Long noncoding RNAs in lipid metabolism: literature review and conservation analysis across species Kevin Muret1, Colette Désert1, Laetitia Lagoutte1, Morgane Boutin1, Florence Gondret1, Tatiana Zerjal2 and Sandrine Lagarrigue1* Abstract Background: Lipids are important for the cell and organism life since they are major components of membranes, energy reserves and are also signal molecules. The main organs for the energy synthesis and storage are the liver and adipose tissue, both in humans and in more distant species such as chicken. -

Screening Differentially Expressed Genes of Pancreatic Cancer
Xu et al. BMC Cancer (2020) 20:298 https://doi.org/10.1186/s12885-020-06722-7 RESEARCH ARTICLE Open Access Screening differentially expressed genes of pancreatic cancer between Mongolian and Han people using bioinformatics technology Jiasheng Xu1†, Kaili Liao2†, Zhonghua Fu3* and Zhenfang Xiong1* Abstract Background: To screen and analyze differentially expressed genes in pancreatic carcinoma tissues taken from Mongolian and Han patients by Affymetrix Genechip. Methods: Pancreatic ductal cell carcinoma tissues were collected from the Mongolian and Han patients undergoing resection in the Second Affiliated Hospital of Nanchang University from March 2015 to May 2018 and the total RNA was extracted. Differentially expressed genes were selected from the total RNA qualified by Nanodrop 2000 and Agilent 2100 using Affymetrix and a cartogram was drawn; The gene ontology (GO) analysis and Pathway analysis were used for the collection and analysis of biological information of these differentially expressed genes. Finally, some differentially expressed genes were verified by real-time PCR. Results: Through the microarray analysis of gene expression, 970 differentially expressed genes were detected by comparing pancreatic cancer tissue samples between Mongolian and Han patients. A total of 257 genes were significantly up-regulated in pancreatic cancer tissue samples in Mongolian patients; while a total of 713 genes were down-regulated. In the Gene Ontology database, 815 differentially expressed genes were identified with clear GO classification, and CPB1 gene showed the highest increase in expression level (multiple difference: 31.76). The pathway analysis detected 28 signaling pathways that included these differentially expressed genes, involving a total of 178 genes. Among these pathways, the enrichment of differentially expressed genes in the FAK signaling pathway was the strongest and COL11A1 gene showed the highest multiple difference (multiple difference: 5.02). -

Updating Phospholipase A2 Biology
biomolecules Review Updating Phospholipase A2 Biology Makoto Murakami * , Hiroyasu Sato and Yoshitaka Taketomi Laboratory of Microenvironmental and Metabolic Health Sciences, Center for Disease Biology and Integrative Medicine, Graduate School of Medicine, The University of Tokyo, Bunkyo-ku, Tokyo 113-8655, Japan; [email protected] (H.S.); [email protected] (Y.T.) * Correspondence: [email protected]; Tel.: +81-3-5841-1431 Received: 24 September 2020; Accepted: 15 October 2020; Published: 19 October 2020 Abstract: The phospholipase A2 (PLA2) superfamily contains more than 50 enzymes in mammals that are subdivided into several distinct families on a structural and biochemical basis. In principle, PLA2 has the capacity to hydrolyze the sn-2 position of glycerophospholipids to release fatty acids and lysophospholipids, yet several enzymes in this superfamily catalyze other reactions rather than or in addition to the PLA2 reaction. PLA2 enzymes play crucial roles in not only the production of lipid mediators, but also membrane remodeling, bioenergetics, and body surface barrier, thereby participating in a number of biological events. Accordingly, disturbance of PLA2-regulated lipid metabolism is often associated with various diseases. This review updates the current state of understanding of the classification, enzymatic properties, and biological functions of various enzymes belonging to the PLA2 superfamily, focusing particularly on the novel roles of PLA2s in vivo. Keywords: fatty acid; knockout mouse; lipid mediator; lipidomics; lysophospholipid; membrane; phospholipase A2; phospholipid 1. Introduction Based on their structural relationships, the PLA2 superfamily is classified into several 2+ families, including the secreted PLA2 (sPLA2), cytosolic PLA2 (cPLA2), Ca -independent PLA2 (iPLA2, also called patatin-like phospholipase (PNPLA)), platelet-activating factor acetylhydrolase (PAF-AH), lysosomal PLA2 (LPLA2), PLA/acyltransferase (PLAAT), α/β hydrolase (ABHD), and glycosylphosphatidylinositol (GPI)-specific PLA2 families. -

Screening Differentially Expressed Genes of Pancreatic Cancer Between Mongolian and Han People Using Bioinformatics Technology
Screening differentially expressed genes of pancreatic cancer between Mongolian and Han people using bioinformatics technology Jiasheng Xu First Aliated Hospital of Nanchang University Kaili Liao Second Aliated Hospital of Nanchang University ZHONGHUA FU First Aliated Hospital of Nanchang University ZHENFANG XIONG ( [email protected] ) The First Aliated Hospital of Nanchang University https://orcid.org/0000-0003-2062-9204 Research article Keywords: Pancreatic ductal cell carcinoma, Affymetrix gene expression prole, Gene differential expression, GO analysis, Pathway analysis, Mongolian Posted Date: July 9th, 2019 DOI: https://doi.org/10.21203/rs.2.11118/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published at BMC Cancer on April 9th, 2020. See the published version at https://doi.org/10.1186/s12885-020-06722-7. Page 1/18 Abstract Objective To screen and analyze differentially expressed genes in pancreatic carcinoma tissues taken from Mongolian and Han patients by Affymetrix Genechip. Methods: Pancreatic ductal cell carcinoma tissues were collected from the Mongolian and Han patients undergoing resection in the Second Aliated Hospital of Nanchang University during March 2015 to May 2018 and the total RNA was extracted. Differentially expressed genes were selected from the total RNA qualied by Nanodrop 2000 and Agilent 2100 using Affymetrix and a cartogram was drawn; The gene ontology (GO) analysis and Pathway analysis were used for the collection and analysis of biological information of these differentially expressed genes. Finally, some differentially expressed genes were veried by real-time PCR. Results Through the microarray analysis of gene expression, 970 differentially expressed genes were detected by comparing pancreatic cancer tissue samples between Mongolian and Han patients. -

Comparison of Human and Mouse Tissues with Focus on Genes with No 1-To-1 Homology
bioRxiv preprint doi: https://doi.org/10.1101/2021.05.22.445250; this version posted May 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. Comparison of human and mouse tissues with focus on genes with no 1-to-1 homology 1,2* 1,2* Jieun Jeong , Manolis Kellis 1 MIT Computer Science and Artificial Intelligence Laboratory, Cambridge, MA 2 Broad Institute of MIT and Harvard, Cambridge, MA *Corresponding author: [email protected], [email protected] Abstract We assembled a panel of 28 tissue pairs of human and mouse with RNA-Seq data on gene expression. We focused on genes with no 1-to-1 homology, because they pose special challenges. In this way, we identified expression patterns that identify and explain differences between the two species and suggest target genes for therapeutic applications. Here we mention three examples. One pattern is observed by defining the aggregate expression of immunoglobulin genes (which have no homology) as a measure of different levels of an immune response. In Lung, we used this statistic to find genes that have significantly higher expression in low/moderate response, and thus they may be therapy targets: increasing their expression or mimicking their function with medications may help in recovery from inflammation in the lungs. Some of the observed associations are common to human and mouse; other associations involve genes involved in cell-to-cell signaling or in regeneration but were not known to be important in Lung. -

Mouse Pla2g1b Conditional Knockout Project (CRISPR/Cas9)
https://www.alphaknockout.com Mouse Pla2g1b Conditional Knockout Project (CRISPR/Cas9) Objective: To create a Pla2g1b conditional knockout Mouse model (C57BL/6J) by CRISPR/Cas-mediated genome engineering. Strategy summary: The Pla2g1b gene (NCBI Reference Sequence: NM_011107 ; Ensembl: ENSMUSG00000029522 ) is located on Mouse chromosome 5. 4 exons are identified, with the ATG start codon in exon 1 and the TAG stop codon in exon 4 (Transcript: ENSMUST00000031495). Exon 2 will be selected as conditional knockout region (cKO region). Deletion of this region should result in the loss of function of the Mouse Pla2g1b gene. To engineer the targeting vector, homologous arms and cKO region will be generated by PCR using BAC clone RP23-87P14 as template. Cas9, gRNA and targeting vector will be co-injected into fertilized eggs for cKO Mouse production. The pups will be genotyped by PCR followed by sequencing analysis. Note: Mice homozygous for disruptions in this gene display abnormalities in lipid absorption, increased insulin sensitivity and improved glucose tolerance. Exon 2 starts from about 7.99% of the coding region. The knockout of Exon 2 will result in frameshift of the gene. The size of intron 1 for 5'-loxP site insertion: 4461 bp, and the size of intron 2 for 3'-loxP site insertion: 1051 bp. The size of effective cKO region: ~660 bp. The cKO region does not have any other known gene. Page 1 of 8 https://www.alphaknockout.com Overview of the Targeting Strategy Wildtype allele gRNA region 5' gRNA region 3' 1 2 3 4 Targeting vector Targeted allele Constitutive KO allele (After Cre recombination) Legends Exon of mouse Pla2g1b Homology arm cKO region loxP site Page 2 of 8 https://www.alphaknockout.com Overview of the Dot Plot Window size: 10 bp Forward Reverse Complement Sequence 12 Note: The sequence of homologous arms and cKO region is aligned with itself to determine if there are tandem repeats. -

Role of Group 1B Phospholipase A2 in Diet-Induced Hyperlipidemia and Selected
Role of Group 1B Phospholipase A2 in Diet-induced Hyperlipidemia and Selected Disorders of Lipid Metabolism A dissertation submitted to the Graduate School at the University of Cincinnati in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Pathobiology and Molecular Medicine of the College of Medicine By Norris Isaac Hollie, II B.S., B.A. Oakwood University, Huntsville, Alabama July 23, 2013 Committee Chair: David Y. Hui, Ph.D. Abstract As obesity rates increase in developed nations, the prevalence of other obesity-related metabolic disorders such as hyperlipidemia, atherosclerosis, and non-alcoholic fatty liver disease (NAFLD) has also increased drastically. A greater understanding of the pathobiology and molecular mechanisms of these disorders becomes increasingly relevant. Recent studies demonstrated that certain alleles of the pancreatic group 1B phospholipase A2 (PLA2G1B) are associated with increased obesity and that Pla2g1b-deficient (Pla2g1b-/-) mice are protected against diet-induced obesity and diabetes. Furthermore, supplying mice with lysophosphatidylcholine (LPC), the enzymatic product of Pla2g1b, causes hyperglycemia and insulin resistance, which are risk factors for hyperlipidemia, atherosclerosis, and NAFLD. Thus, Pla2g1b may play a role in the development of these obesity-related diseases and inhibiting Pla2g1b and/or LPC may change the progression of these metabolic disorders. The goal of the first part of this dissertation was to identify a Pla2g1b-mediated protection against hyperlipidemia. Findings from these studies indicate that Pla2g1b-/- mice are protected against high fat diet-induced hyperlipidemia and gain less weight than Pla2g1b+/+ controls due to decreased very-low-density lipoprotein (VLDL) production and increased postprandial triglyceride-rich lipoprotein clearance. -
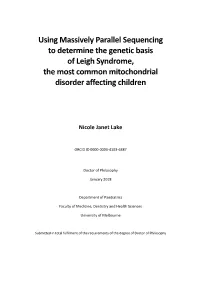
Using Massively Parallel Sequencing to Determine the Genetic Basis of Leigh Syndrome, the Most Common Mitochondrial Disorder Affecting Children
Using Massively Parallel Sequencing to determine the genetic basis of Leigh Syndrome, the most common mitochondrial disorder affecting children Nicole Janet Lake ORCID ID 0000-0003-4103-6387 Doctor of Philosophy January 2018 Department of Paediatrics Faculty of Medicine, Dentistry and Health Sciences University of Melbourne Submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy Abstract Mitochondrial diseases are debilitating illnesses caused by mutations that impair mitochondrial energy generation. The most common clinical presentation of mitochondrial disease in children is Leigh syndrome. This neurodegenerative disorder can be caused by mutations in more than 85 genes, encoded by both nuclear and mitochondrial DNA (mtDNA). When this PhD commenced, massively parallel sequencing for genetic diagnosis of Leigh syndrome was transitioning into the clinic, however its diagnostic utility in a clinical setting was unknown. Furthermore, a significant number of Leigh syndrome patients remained without a genetic diagnosis, indicating that further research was required to expand our understanding of the genetic basis of disease. To identify the maximum diagnostic yield of massively parallel sequencing in patients with Leigh syndrome, and to provide insight into the genetic basis of disease, unsolved patients from a historical Leigh syndrome cohort were studied. This cohort is comprised of 67 clinically- ascertained patients diagnosed with Leigh or Leigh-like syndrome according to stringent criteria. DNA from all 33 patients lacking a genetic diagnosis underwent whole exome sequencing, with parallel sequencing of the mtDNA. A targeted analysis of 2273 genes was performed, which included known and candidate mitochondrial disease genes, and differential diagnosis genes underlying distinct disorders with phenotypic overlap. -

Gene Ontology DBGGA Analysis Dynamic Bayesian Network Modeling
Seralogix Computational Systems Biology Approach to Comparative Pathogenicity Transcriptome Analysis and Modeling A Service provided by the Animal Systems Biology ASBAMC at UC Davis Huaijun Zhou, PhD Kenneth Drake, PhD ASBAMC Program Director (PI) ASBAMC (Co-PI) Department of Animal Science Chief Technology Officer University of California, Davis Seralogix [email protected] [email protected] This presentation is supported by Agriculture and Food Research Initiative Competitive Grant no. 2011-67015-30196 from the USDA National Institute of Food and Agriculture Computational tool development supported by National Institutes of Allergies and Infectious Diseases (SBIR grants 2R44AI058362-02 and R43AI084223-01) and National Human Genome Research Institute (SBIR grants 2R44HG004457-02) Presentation Outline • Animal Systems Biology Analysis and Modeling Center – Rationale and mission • In Silico System Biology Analysis and Modeling Overview – Computational pipeline in an integrated analysis and modeling platform • Case study: comparative pathogenicity analysis and modeling – Chickens inoculated with Campylobacter jejuni (C. jejuni) • Broiler chickens: Resistant (Line A) and susceptible (Line B) – C. jejuni colonization in ceca • Wild type and mutant strains • Important Contact Information The ASBAMC at UC Davis A joint university and industrial program • Rationale – Exponential growth of “omic” data past and future • Microarray. next generation sequencing, metabolomics, and proteomics • Significant challenges to animal molecular biologists/researchers -

Phospholipase a Subclasses in Acute Respiratory Distress Syndrome Eirini Kitsiouli, George Nakos, Marilena E
Phospholipase A Subclasses in Acute Respiratory Distress Syndrome Eirini Kitsiouli, George Nakos, Marilena E. Lekka To cite this version: Eirini Kitsiouli, George Nakos, Marilena E. Lekka. Phospholipase A Subclasses in Acute Respiratory Distress Syndrome. Biochimica et Biophysica Acta - Molecular Basis of Disease, Elsevier, 2009, 1792 (10), pp.941. 10.1016/j.bbadis.2009.06.007. hal-00521089 HAL Id: hal-00521089 https://hal.archives-ouvertes.fr/hal-00521089 Submitted on 25 Sep 2010 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. ÔØ ÅÒÙ×Ö ÔØ Phospholipase A2 Subclasses in Acute Respiratory Distress Syndrome Eirini Kitsiouli, George Nakos, Marilena E. Lekka PII: S0925-4439(09)00138-0 DOI: doi:10.1016/j.bbadis.2009.06.007 Reference: BBADIS 62968 To appear in: BBA - Molecular Basis of Disease Received date: 19 March 2009 Revised date: 25 June 2009 Accepted date: 25 June 2009 Please cite this article as: Eirini Kitsiouli, George Nakos, Marilena E. Lekka, Phospho- lipase A2 Subclasses in Acute Respiratory Distress Syndrome, BBA - Molecular Basis of Disease (2009), doi:10.1016/j.bbadis.2009.06.007 This is a PDF file of an unedited manuscript that has been accepted for publication. -

(12) United States Patent (10) Patent No.: US 9,163,078 B2 Rao Et Al
US009 163078B2 (12) United States Patent (10) Patent No.: US 9,163,078 B2 Rao et al. (45) Date of Patent: *Oct. 20, 2015 (54) REGULATORS OF NFAT 2009.0143308 A1 6, 2009 Monk et al. 2009,0186422 A1 7/2009 Hogan et al. (75) Inventors: Anjana Rao, Cambridge, MA (US); 2010.0081129 A1 4/2010 Belouchi et al. Stefan Feske, New York, NY (US); Patrick Hogan, Cambridge, MA (US); FOREIGN PATENT DOCUMENTS Yousang Gwack, Los Angeles, CA (US) CN 1329064 1, 2002 EP O976823. A 2, 2000 (73) Assignee: Children's Medical Center EP 1074617 2, 2001 Corporation, Boston, MA (US) EP 1293569 3, 2003 WO 02A30976 A1 4, 2002 (*) Notice: Subject to any disclaimer, the term of this WO O2/O70539 9, 2002 patent is extended or adjusted under 35 WO O3/048.305 6, 2003 U.S.C. 154(b) by 0 days. WO O3/052049 6, 2003 WO WO2005/O16962 A2 * 2, 2005 This patent is Subject to a terminal dis- WO 2005/O19258 3, 2005 claimer. WO 2007/081804 A2 7, 2007 (21) Appl. No.: 13/161,307 OTHER PUBLICATIONS (22) Filed: Jun. 15, 2011 Skolnicket al., 2000, Trends in Biotech, vol. 18, p. 34-39.* Tomasinsig et al., 2005, Current Protein and Peptide Science, vol. 6, (65) Prior Publication Data p. 23-34.* US 2011 FO269174 A1 Nov. 3, 2011 Smallwood et al., 2002, Virology, vol. 304, p. 135-145.* • - s Chattopadhyay et al., 2004. Virus Research, vol. 99, p. 139-145.* Abbas et al., 2005, computer printout pp. 2-6.* Related U.S. -

The Transition from Primary Colorectal Cancer to Isolated Peritoneal
www.nature.com/scientificreports OPEN The transition from primary colorectal cancer to isolated peritoneal malignancy is associated with an increased tumour mutational burden Sally Hallam, Joanne Stockton, Claire Bryer, Celina Whalley, Valerie Pestinger, Haney Youssef & Andrew D. Beggs* Colorectal Peritoneal metastases (CPM) develop in 15% of colorectal cancers. Cytoreductive surgery and heated intraperitoneal chemotherapy (CRS & HIPEC) is the current standard of care in selected patients with limited resectable CPM. Despite selection using known prognostic factors survival is varied and morbidity and mortality are relatively high. There is a need to improve patient selection and a paucity of research concerning the biology of isolated CPM. We aimed to determine the biology associated with transition from primary CRC to CPM and of patients with CPM not responding to treatment with CRS & HIPEC, to identify those suitable for treatment with CRS & HIPEC and to identify targets for existing repurposed or novel treatment strategies. A cohort of patients with CPM treated with CRS & HIPEC was recruited and divided according to prognosis. Molecular profling of the transcriptome (n = 25), epigenome (n = 24) and genome (n = 21) of CPM and matched primary CRC was performed. CPM were characterised by frequent Wnt/ β catenin negative regulator mutations, TET2 mutations, mismatch repair mutations and high tumour mutational burden. Here we show the molecular features associated with CPM development and associated with not responding to CRS & HIPEC.