Travancore Government and Public Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Particulars of Some Temples of Kerala Contents Particulars of Some
Particulars of some temples of Kerala Contents Particulars of some temples of Kerala .............................................. 1 Introduction ............................................................................................... 9 Temples of Kerala ................................................................................. 10 Temples of Kerala- an over view .................................................... 16 1. Achan Koil Dharma Sastha ...................................................... 23 2. Alathiyur Perumthiri(Hanuman) koil ................................. 24 3. Randu Moorthi temple of Alathur......................................... 27 4. Ambalappuzha Krishnan temple ........................................... 28 5. Amedha Saptha Mathruka Temple ....................................... 31 6. Ananteswar temple of Manjeswar ........................................ 35 7. Anchumana temple , Padivattam, Edapalli....................... 36 8. Aranmula Parthasarathy Temple ......................................... 38 9. Arathil Bhagawathi temple ..................................................... 41 10. Arpuda Narayana temple, Thirukodithaanam ................. 45 11. Aryankavu Dharma Sastha ...................................................... 47 12. Athingal Bhairavi temple ......................................................... 48 13. Attukkal BHagawathy Kshethram, Trivandrum ............. 50 14. Ayilur Akhileswaran (Shiva) and Sri Krishna temples ........................................................................................................... -

Struggle of the Linguistic Minorities and the Formation of Pattom Colony
ADVANCE RESEARCH JOURNAL OF SOCIAL SCIENCE A CASE STUDY Volume 9 | Issue 1 | June, 2018 | 130-135 e ISSN–2231–6418 DOI: 10.15740/HAS/ARJSS/9.1/130-135 Visit us : www.researchjournal.co.in Struggle of the linguistic minorities and the formation of Pattom Colony C.L. Vimal Kumar Department of History, K.N.M. Government Arts and Science College, Kanjiramkulam, Thiruvananthapuram (Kerala) India ARTICLE INFO : ABSTRACT Received : 07.03.2018 Land has many uses but its availability is limited. During the early 1940s extensive Accepted : 28.05.2018 food shortages occurred throughout Travancore. As a result, the government opened forestlands on an emergency basis for food cultivation and in 1941 granted exclusive cultivation rights known as ‘Kuthakapattam’ was given (cultivation on a short-term KEY WORDS : lease) in state forest areas. Soon after independence, India decided to re-organize Kuthakapattam, Annas, Prathidwani, state boundaries on a linguistic basis. The post Independence State reorganization Pattayam, Blocks, Pilot colony period witnessed Tamil-Malayali dispute for control of the High Ranges. The Government of Travancore-Cochin initiated settlement programmes in the High Range HOW TO CITE THIS ARTICLE : areas in order to alter the regional linguistic balance. Pattom colony, which was Vimal Kumar, C.L. (2018). Struggle of sponsored by Pattom Thanupillai ministry, as a part of High Range colonization scheme. the linguistic minorities and the formation It led to forest encroachment, deforestation, soil erosion, migration, conflict over control of Pattom Colony. Adv. Res. J. Soc. Sci., of land and labour struggle and identity crisis etc. 9 (1) : 130-135, DOI: 10.15740/HAS/ ARJSS/9.1/130-135. -

Travancore Engineering College, Oyoor, Kollam (Unaided College) - Shifting of 6 Th and 8 Th Semester Students- 2016-17- Sanctioned- Orders Issued
UNIVERSITY OF KERALA (Abstract) Travancore Engineering College, Oyoor, Kollam (Unaided College) - shifting of 6 th and 8 th semester students- 2016-17- sanctioned- orders issued. ACADEMIC ‘BI’ SECTION No. AcBI/12235/2017 Thiruvananthapuram, Dated: 17.03.2017 Read: 1.UO No.Ac.BI/13387/2002-03 dated 23.05.2003 2.Letter No. ASC(P)19/17/HO/TVPM/ENGG/TEC dated 15.02.2017 from the Admission Supervisory Committee for Professional Colleges. 3.Additional item No.2 of the minutes of the meeting of the Syndicate held on 10.02.2017. 4.Minutes of the meeting of the Standing Committee of the Syndicate on Affiliation of Colleges held on 27.02.2017 ORDER The University of Kerala vide paper read (1) above granted provisional affiliation to the Travancore Engineering College, Oyoor, Kollam to function on self financing basis from the academic year 2002-03. Various complaints had been received from the students of Travancore Engineering College, Oyoor, Kollam, their parents and teachers regarding the non conduct of classes and non payment of salary to teachers. In view of the above grave issues in the college, the Admission Supervisory Committee vide paper read as (2) above requested the University to take necessary steps to transfer the students of S6 and S8 to some other college/ colleges of Engineering. The Syndicate held on 10.02.2017 considered the representation submitted by the Students of Travancore Engineering College, Oyoor and resolved to entrust the Convenor, Standing Committee of the Syndicate on Examinations and Students Discipline and the Controller of Examinations to reallocate the students to neighboring college for the conduct of lab examinations for the 5 th Semester students and to work out the modalities for their registration to the 6 th Semester. -

Supremacy of Dutch in Travancore (1700-1753)
http://www.epitomejournals.com Vol. 4, Issue 6, June 2018, ISSN: 2395-6968 SUPREMACY OF DUTCH IN TRAVANCORE (1700-1753) Dr. B. SHEEBA KUMARI, Assistant Professor, Department of History, S. T. Hindu College, Nagercoil - 629 002. ABSTRACT in Travancore especially the Dutch from 1700 to 1753 A.D. was noted worthy in Travancore, a premier princely state of the history of the state. In this context, this south India politically, occupied an paper high lights the part of the Dutch to important place in Travancore history. On attain the political supremacy in the eve of the eighteenth century the Travancore. erstwhile state Travancore was almost like KEYWORDS a political Kaleidoscope which was greatly Travancore, Kulachal, Dutch Army, disturbed by internal and external Ettuveettil Pillamar, Marthanda Varma, dissensions. The internal feuds coupled Elayadathu Swarupam with machinations of the European powers. Struggled for political supremacy RESEARCH PAPER Travancore the princely state became an attractive for the colonists of the west from seventeenth century onwards. The Portuguese, the Dutch and the English developed commercial relations with the state of Travancore1. Among the Europeans the Portuguese 70 BSK Impact Factor = 3.656 Dr. Pramod Ambadasrao Pawar, Editor-in-Chief ©EIJMR All rights reserved. http://www.epitomejournals.com Vol. 4, Issue 6, June 2018, ISSN: 2395-6968 were the first to develop commercial contacts with the princes, and establish and fortress in the regions2. Their possessions were taken over by the later adventurers, the Dutch3. The aim of the Dutch in the beginning of the seventeenth century was to take over the whole of the Portuguese trading empire in Asia. -

The Ascent of 'Kerala Model' of Public Health
THE ASCENT OF ‘KERALA MODEL’ OF PUBLIC HEALTH CC. Kartha Kerala Institute of Medical Sciences, Trivandrum, Kerala [email protected] Kerala, a state on the southwestern Coast of India is the best performer in the health sector in the country according to the health index of NITI Aayog, a policy think-tank of the Government of India. Their index, based on 23 indicators such as health outcomes, governance and information, and key inputs and processes, with each domain assigned a weight based on its importance. Clearly, this outcome is the result of investments and strategies of successive governments, in public health care over more than two centuries. The state of Kerala was formed on 1 November 1956, by merging Malayalam-speaking regions of the former states of Travancore-Cochin and Madras. The remarkable progress made by Kerala, particularly in the field of education, health and social transformation is not a phenomenon exclusively post 1956. Even during the pre-independence period, the Travancore, Cochin and Malabar provinces, which merged to give birth to Kerala, have contributed substantially to the overall development of the state. However, these positive changes were mostly confined to the erstwhile princely states of Travancore and Cochin, which covered most of modern day central and southern Kerala. The colonial policies, which isolated British Malabar from Travancore and Cochin, as well as several social and cultural factors adversely affected the general and health care infrastructure developments in the colonial Malabar region. Compared to Madras Presidency, Travancore seems to have paid greater attention to the health of its people. Providing charity to its people through medical relief was regarded as one of the main functions of the state. -

Travancore-Cochin Integration; a Model to Native States of India
Journal of Xi'an University of Architecture & Technology ISSN No : 1006-7930 Travancore-Cochin Integration; A model to Native states of India Dr Suresh J Assistant Professor, Department Of History University College, Thiruvanathapuram Kerala University Abstract The state of Kerala once remained as an integral part of erstwhile Tamizakaom. Towards the beginning of the modern age this political terrain gradually enrolled as three native kingdoms with clear cut boundaries. The three native states comprised kingdom of Travancore of kingdom of Cochin, kingdom of Calicut These territories never enjoyed a single political structure due to the internal and foreign interventions. Travancore and Cochin were neighboring states enjoyed cordial relations. The integration of both states is a unique event in the history of India as well as History of Kerala. The title of Rajapramukh and the administrative division of Dewaswam is unique aspect in the course of History. Keywords Rajapramukh , Dewaswam , Panjangam, Yogam, annas, oorala, Melkoima Introduction The erstwhile native state of Travancore and Cochin forms political unity of Indian sub- continent through discussions debates and various agreements. The states situating nearby maintained interstate reactions in various realms. At occasionally they maintained cordial relation on the other half hostile in every respect. In different epochs the diplomatic relations of both the state were unique interns of political economic, social and cultural aspects. This uniqueness ultimately enabled both the state to integrate them ultimate into the concept of the formation of the state of Kerala. The division of power in devaswams and assumed the title Rajapramukh is unique chapters in Kerala as well as Indian history Volume XII, Issue VII, 2020 Page No: 128 Journal of Xi'an University of Architecture & Technology ISSN No : 1006-7930 Scope and relevance of Study Travancore and Cochin the native states of southern kerala. -

Travancore Medical College
Travancore Medical College https://www.indiamart.com/company/9403426/ Travancore Medical College Hospital, functioning in Kollam Medi City is a unit under the Quilon Medical trust. TMCH is ISO 9001: 2008 certified and spread over 98 acres of land. The hospital is facilitated with 850 bedded and is a ... About Us Travancore Medical College Hospital, functioning in Kollam Medi City is a unit under the Quilon Medical trust. TMCH is ISO 9001: 2008 certified and spread over 98 acres of land. The hospital is facilitated with 850 bedded and is a multi-specialty hospital equipped with state-of-the-art equipment providing end-to-end treatment in the field of almost all branches of Medicine. The Medical College is provided with a most advanced level for all super-specialty units and colleges for medical and nursing courses. The campus is half a kilometer away from NH-47 (Kollam-Thiruvananthapuram portion). Kollam Medicity stands as the nerve center in medical field, located in midst of Kollam-Kerala with a lovely ambiance apart from the crowded city life. The best approach to patients with the best modern medical facilities at reasonable rate highlighted the hospital since its establishment in 2009. Our focus on professional excellence and community engagement draws an increasing number of patients, bright students and technicians to our campus.Travancore Medical College is a gang up of a diverse team of doctors, nursing staff, allied health professionals, teachers, researchers and administrators, from highly experienced to the young and enthusiastic, comprising of the finest healthcare professionals in the region. It is our belief that access to better and quality healthcare can deliver outstanding benefits to all stakeholders in the larger community we serve. -
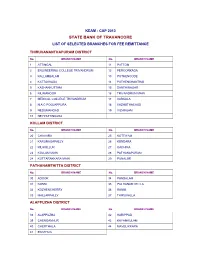
State Bank of Travancore List of Selected Branches for Fee Remittance
KEAM : CAP 2013 STATE BANK OF TRAVANCORE LIST OF SELECTED BRANCHES FOR FEE REMITTANCE THIRUVANANTHAPURAM DISTRICT No. BRANCH NAME No. BRANCH NAME 1 ATTINGAL 11 PATTOM 2 ENGINEERING COLLEGE TRIVANDRUM 12 PEROORKADA 3 KALLAMBALAM 13 POTHENCODE 4 KATTAKKADA 14 PUTHENCHANTHAI 5 KAZHAKKUTTAM 15 SANTHINAGAR 6 KILIMANOOR 16 TRIVANDRUM MAIN 7 MEDICAL COLLEGE TRIVANDRUM 17 VARKALA 8 N A C POOJAPPURA 18 VAZHUTHACAUD 9 NEDUMANGAD 19 VIZHINJAM 10 NEYYATTINKARA KOLLAM DISTRICT No. BRANCH NAME No. BRANCH NAME 20 CHAVARA 25 KOTTIYAM 21 KARUNAGAPALLY 26 KUNDARA 22 KILIKOLLUR 27 OACHIRA 23 KOLLAM MAIN 28 PATHANAPURAM 24 KOTTARAKKARA MAIN 29 PUNALUR PATHANAMTHITTA DISTRICT No. BRANCH NAME No. BRANCH NAME 30 ADOOR 34 PANDALAM 31 KONNI 35 PATHANAMTHITTA 32 KOZHENCHERRY 36 RANNI 33 MALLAPPALLY 37 THIRUVALLA ALAPPUZHA DISTRICT No. BRANCH NAME No. BRANCH NAME 38 ALAPPUZHA 42 HARIPPAD 39 CHENGANNUR 43 KAYAMKULAM 40 CHERTHALA 44 MAVELIKKARA 41 EDATHUA KOTTAYAM DISTRICT No. BRANCH NAME No. BRANCH NAME 45 ANTHINAD 54 MANIMALA 46 CHANGANASSERRY MAIN 55 MEDICAL COLLEGE KOTTAYAM 47 CHINGAVANAM 56 PALA 48 C M S COLLEGE KOTTAYAM 57 PAMPADY 49 ETTUMANOOR 58 PUTHUPALLY 50 KADUTHURUTHY 59 THALAYOLAPARAMBU 51 KANJIKUZHY 60 UZHAVOOR 52 KANJIRAPALLY 61 VAIKOM 53 KOTTAYAM MAIN 62 VAKATHANAM IDUKKI DISTRICT No. BRANCH NAME No. BRANCH NAME 63 IDUKKI 67 NEDUMKANDAM 64 KATTAPPANA 68 PEERUMEDU 65 KUMILY 69 THODUPUZHA 66 MUNNAR 70 VANDIPERIYAR ERNAKULAM DISTRICT No. BRANCH NAME No. BRANCH NAME 71 ALUVA 78 KOTHAMANGALAM 72 ANGAMALI 79 MG ROAD ERNAKULAM 73 EDAPPALLY 80 MUVATTUPUZHA 74 KAKKANAD CIVIL STATION 81 PANAMPALLY NAGAR 75 KALAMASSERRY MAIN 82 PERUMBAVOOR 76 KOCHI 83 TRIPPUNITHURA 77 KOOTHATTUKULAM THRISSUR DISTRICT No. -
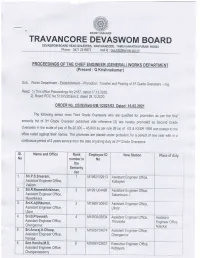
Travancore Devaswom Board D Evasw
SWAMY SARANAM TRAVANCORE DEVASWOM BOARD D EVASW. M B oA - -Hii]! R:J:t?,:'AilE7; -A M 6e 500 3 ^ ?,,-o[ff*X$l[]1ff ' HIEF GE RKS DEP (Present : G,Krishnakumar) Sub: Works Department - Establishment - Promotion, Transfer and Posting of 3'd Grade Overseers - reg Read: 1)This office Proceedings N0,2182, dated 1T,j2.ZO2C., 2) Board ROC No.51391t20lEst-2, dated 28,,10,2020, The following senior most Third Grade Overseers who are qualified for promotion as per the final seniority list of 3rd Grade Overseer published vide reference (2) are hereby promoted as Second Grade overseers in the scale of pay of Rs.20,000 - 45,800 as per rule 28 (a) of KS & KSSR 1g5g and posted to the office noted against names, promotes their The are placed under probatron for a period of one year with in a continuous period of 2 years service from the date of joining duty as 2rd Grade Overseers, st. Name and Office Rank Employee lD New Station Place of duiy No number in No the Seniority list 1 Sri.P.S.Sreeram, 1 M1 982Y0291 3 Assistant Engineer Office, Assistant Engineer Office, Kottayam Vaikom 2, Sri.R.Ramesh krishnan, 2 M1991J04498 Assistant Engineer Office, Assistant Engineer Office, Sabarimala -l Mavelikkara 3. Sri.K.Ajithkumar, J M1 966Y00843 Assistant Engineer Office, Assistant Engineer Office, Ulloor Uloor 4, Sri.B.Praveesh, 4 M1993A03834 Assistant Engineer Office, Assistant Assistant Engineer Office, Thiruvalla Engrneer Office Chengannur Nilackal ( 5. Sri.Anuraj.K,Dileep, M1995Y04674 Assistant Engineer Offi ce, Assistant Engineer Office, Chengannur Pampa 6, Smt.Harsha.M.D, 0 M1 994Y03837 Executive Engineer Office, Assistant Engineer Office, Kottayam Chanoanasserrry st. -

The Turning Point in a Living Tradition (PDF)
The Turning Point in a Living Tradition Somayāgam 2003 T. P. Mahadevan & Frits Staal 1. Introduction During April 7–12, 2003, a “Somayāgam,” i.e., agniṣṭoma-somayāga, was per- formed by Nambudiri Brahmans in Trichur in central Kerala, formerly the Cochin State. 1 It was preceded by “Ādhānam,” i.e., agnyādhāna or punarādheya, on April 6. The location of the ceremonies was the “Vadakke Madham Brahmaswam,” the Northern (vadakke) of two Vedic institutions within Trichur town where the Ṛgve- da has been taught to young pupils for four centuries or more. (The Southern Mad- ham is for saṁnyāsins of which there is at present one.) The last performance of Somayāgam was in 1984. It is one of two large Vedic rituals that are preserved in the Nambudiri community, the other being the 12-day “Agni” or atirātra-agnicayana. One of the many characteristic differences bet- ween the two rituals is that there are twelve “Soma-sequences” in the somayāga and twenty-nine in the atirātra-agnicayana. A soma sequence consists of a Sāma- veda chant (stotra or stuti, as the Nambudiris call it), ṚṚgveda recitation (śastra), soma offerings to the deities and soma drinking by the Yajamāna and his priests. The first twelve soma sequences of the agnicayana are similar to the twelve se- quences of the somayāga, but all of them are not the same. And only a ritualist who has performed a Somayāga and become a Somayāji, is eligible for an Agnica- yana and to become an Akkitiri. The authors of the present article were both able to attend the 2003 ceremonies at Trichur but Mahadevan (TP) could spend more time than Staal (FS) in Kerala 1 We are profoundly grateful to Vaidikan Taikkat Nilakanthan Nambudiri, Vaidikan for the 2003 Somayāgam, and to Shri O.N.Damodaran Nambudiripad, Vice President of the Vadakke Madham Brahmaswam, for welcoming us on the occasion of the Somayāgam performance and assisting us in countless ways. -

Impact of Vaikom and Suchidram Satyagrahas in Travancore- an Historical Overview
IMPACT OF VAIKOM AND SUCHIDRAM SATYAGRAHAS IN TRAVANCORE- AN HISTORICAL OVERVIEW Dr. PRAVEEN. O.K Assistant professor, Department of History, SREE KERALA VARMA COLLE, THRISSUR, KERALA, INDIA. ABSTRACT The chief social evil in Travancore, as elsewhere in India, was caste. Though the traditional caste system was not in vogue in Travancore, the Brahmins held the highest place in society. And owners of all land in the country they depended upon the Nairs for the proper management of of the land. The Nairs grew into a warrior class protecting the interests of the Brahmins to form the upper class. The Ezhavas or Tiyas, the Nadars, the pulayas and the parayas were the low caste. These low castes were subjected to glaring disabilities on account of the peculiar social customs which were very strictly followed in Travancore. The treatment which the untouchables received at the hands of the caste Hindus from time immemorial was unsympathetic and even inhuman. Broadly speaking the people of Travancore divided into Avarnas and Savarnas. The avarnas were low castes such as the Adidravidians, Alvans, Aryans, Baratars, Chakaravars, Ezhavas, Kaniyans, Kuravans, Nadars, panas, pulayas, parayas, velan, vedann etc. KEY WORDS: TRAVANCORE, SATYAGRAHA, TEMPLE, VAIKOM SATYAGRHA, SUCHIDRAM SATYAGRHA, TEMPLE ENTRY PROCLAMATION INTRODUCTION They were strictly prohibited from entering into the temples and using public wells, tanks and chatrams (rest houses). Equal opportunity of education and employment was denied to the Avarnas. Unapprochability was also very severe in Travancore. Francis Day says that, Ilava (Ezhava) must keep 36 paces from Brahmin and 12 from a Nayar while a Kaniyan would pollute a Nambudiri Brahmin at 24 ft., 96 paces as the4 distance for a Pulayan from Nair. -

Idukki District Kerala
Vol. 5 No. 4 April 2018 ISSN: 2321-788X UGC Approval No: 43960 Impact Factor: 3.025 MIGRATION AND CHANGES IN LAND USE PATTERN IN UDUMBANCHOLA TALUK- IDUKKI DISTRICT KERALA DIBU AVIRACHAN Research Scholar in History, University of Kerala, India Article Particulars: Received: 23.02.2018 Accepted: 23.04.2018 Published: 28.04.2018 Abstract This paper outlines the history of migration and the changes in land use pattern in Udumbanchola taluk in Idukki district, Kerala. The relationship between various religious communities has greatly influenced migration, forest enchrochment and conflict over land controle in this area. A historical analysis of this relationship is essential to understanding the causes of changes in land use pattern in the study area. The comparative study shows that the settlement areas that occupied hardly 0.73% in 1910 were increased to 30.57% in 1990 by transferring forest lands, grasslands and cardamom plantations. Due to the depletion of natural vegetation and grass land system by the establishment of houses, cash crops and infrastructural facilities, combined with the absence of sufficient land management measures in the side slopes resulted severe land degradation in the study area. Introduction Idukki district was formed in the year 1972 as per Government notification No54131/C2/72/RD dated 24th January 1972. The district consists of Devikulam, Udumbanchola and Peerumedu taluk of the earst while Kottayam district and Thodupuzha taluk of the earstwhile Ernakulam district¹. At the time of formation, the district headquarters started functioning at kottayam and from there it was shifted to painavu in Thodupuzha taluk in june 1976, where it is proposed to build a new planned forest township².