Ligaments Je
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole with Concurrent Scapholunate Dissociation
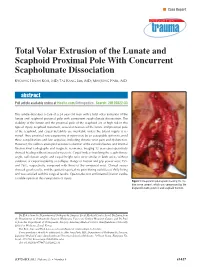
n Case Report Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole With Concurrent Scapholunate Dissociation KYOUNG HWAN KOH, MD; TAE KANG LIM, MD; MIN JONG PARK, MD abstract Full article available online at Healio.com/Orthopedics. Search: 20120822-33 This article describes a case of a 24-year-old man with a total volar extrusion of the lunate and scaphoid proximal pole with concurrent scapholunate dissociation. The viability of the lunate and the proximal pole of the scaphoid are at high risk in this type of injury. Scaphoid nonunion, avascular necrosis of the lunate and proximal pole of the scaphoid, and carpal instability are inevitable unless the blood supply is re- stored. Thus, proximal row carpectomy at injury may be an acceptable option to avoid these complications and late sequelae, including chronic wrist pain and dysfunction. However, the authors attempted accurate reduction of the extruded bones and internal fixation.Final radiographs and magnetic resonance imaging 12 years postoperatively showed healing without avascular necrosis. Carpal indices involving the scapholunate angle, radiolunate angle, and carpal height ratio were similar in both wrists without evidence of carpal instability or collapse. Range of motion and grip power were 75% and 76%, respectively, compared with those of the uninjured wrist. Clinical scores showed good results, and the patient reported no pain during activities of daily living and was satisfied with his surgical results. Open reduction and internal fixation can be a viable option in this rare pattern of injury. Figure: Intraoperative photograph showing the me- dian nerve (arrow), which was compressed by the displaced lunate (asterisk) and scaphoid fracture. -

THE STUDY of CORACOACROMIAL LIGAMENT MORPHOLOGY and ITS CLINICAL ASPECTS Sowmya S *1, Sharmada Kl 2, Meenakshi Parthasarathy 3
International Journal of Anatomy and Research, Int J Anat Res 2020, Vol 8(1.2):7342-45. ISSN 2321-4287 Original Research Article DOI: https://dx.doi.org/10.16965/ijar.2019.377 THE STUDY OF CORACOACROMIAL LIGAMENT MORPHOLOGY AND ITS CLINICAL ASPECTS Sowmya S *1, Sharmada Kl 2, Meenakshi Parthasarathy 3. *1 Associate professor, Dept of Anatomy, Bowring & Lady Curzon Medical College & Research Institute, Karnataka, India, [email protected] 2 Tutor, Dept of Anatomy, Bowring & Lady Curzon Medical College & Research Institute, Karnataka, India, [email protected] 3 Professor, Dept of Anatomy, Bowring & Lady Curzon Medical College & Research Institute, Karnataka, India, [email protected] ABSTRACT Background: The coracoacromial ligament (CAL) as an integral component of the coracoacromial arch, plays an important role in shoulder biomechanics, joint stability, and proprioception thus maintains static restraint due to its dynamic interactions with ligaments, muscles and bony elements around the shoulder joint. Age-dependent changes due to chronic stress and cellular degradation cause thickening and stiffening of the CAL that may contribute to a spectrum of shoulder pathology from capsular tightness to rotator cuff tear arthropathy and impingement syndrome. Objectives: This study conducted to observe the different types of CAL and its relationship with coracoacromial veil. Materials and Methods: The study conducted on 50 upper limbs at Bowring & Lady Curzon medical college & research institute and Bangalore medical college & research institute. The upper limbs were dissected at the shoulder joint complex and acromion process and coracoid process were appreciated and coracoacromial ligaments were appreciated for their types and morphometry. Results and Conclusion: Four types of CAL were observed in this study. -

Treatment of Common Hip Fractures: Evidence Report/Technology
This report is based on research conducted by the Minnesota Evidence-based Practice Center (EPC) under contract to the Agency for Healthcare Research and Quality (AHRQ), Rockville, MD (Contract No. HHSA 290 2007 10064 1). The findings and conclusions in this document are those of the authors, who are responsible for its content, and do not necessarily represent the views of AHRQ. No statement in this report should be construed as an official position of AHRQ or of the U.S. Department of Health and Human Services. The information in this report is intended to help clinicians, employers, policymakers, and others make informed decisions about the provision of health care services. This report is intended as a reference and not as a substitute for clinical judgment. This report may be used, in whole or in part, as the basis for the development of clinical practice guidelines and other quality enhancement tools, or as a basis for reimbursement and coverage policies. AHRQ or U.S. Department of Health and Human Services endorsement of such derivative products may not be stated or implied. Evidence Report/Technology Assessment Number 184 Treatment of Common Hip Fractures Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services 540 Gaither Road Rockville, MD 20850 www.ahrq.gov Contract No. HHSA 290 2007 10064 1 Prepared by: Minnesota Evidence-based Practice Center, Minneapolis, Minnesota Investigators Mary Butler, Ph.D., M.B.A. Mary Forte, D.C. Robert L. Kane, M.D. Siddharth Joglekar, M.D. Susan J. Duval, Ph.D. Marc Swiontkowski, M.D. -

Subacromial Decompression in the Shoulder
Subacromial Decompression Geoffrey S. Van Thiel, Matthew T. Provencher, Shane J. Nho, and Anthony A. Romeo PROCEDURE 2 22 Indications P ITFALLS ■ Impingement symptoms refractory to at least • There are numerous possible 3 months of nonoperative management causes of shoulder pain that can ■ In conjunction with arthroscopic treatment of a mimic impingement symptoms. All potential causes should be rotator cuff tear thoroughly evaluated prior to ■ Relative indication: type II or III acromion with undertaking operative treatment clinical fi ndings of impingement of isolated impingement syndrome. Examination/Imaging Subacromial Decompression PHYSICAL EXAMINATION ■ Assess the patient for Controversies • Complete shoulder examination with range of • Subacromial decompression in motion and strength the treatment of rotator cuff • Tenderness with palpation over anterolateral pathology has been continually acromion and supraspinatus debated. Prospective studies • Classic Neer sign with anterolateral shoulder have suggested that there is no difference in outcomes with and pain on forward elevation above 90° when without subacromial the greater tuberosity impacts the anterior decompression. acromion (and made worse with internal rotation) • Subacromial decompression • Positive Hawkins sign: pain with internal rotation, performed in association with a forward elevation to 90°, and adduction, which superior labrum anterior- causes impingement against the coracoacromial posterior (SLAP) repair can potentially increase ligament postoperative stiffness. ■ The impingement test is positive if the patient experiences pain relief with a subacromial injection of lidocaine. ■ Be certain to evaluate for acromioclavicular (AC) joint pathology, and keep in mind that there are several causes of shoulder pain that can mimic impingement syndrome. P ITFALLS IMAGING • Ensure that an axillary lateral ■ Standard radiographs should be ordered, view is obtained to rule out an os acromiale. -

Osteoarthritis Epidemiologicosteoarthritis and Genetic Aspects Epidemiologic and Genetic Aspects
From the Department of Orthopedics, Clinical Sciences From the DepartmentLund University, of Orthopedics, Lund, Sweden Clinical Sciences Lund University, Lund, Sweden Osteoarthritis EpidemiologicOsteoarthritis and genetic aspects Epidemiologic and genetic aspects Jonas Franklin Jonas Franklin Thesis 2010 Thesis 2010 Contact address Jonas Franklin Department of Orthopedics Akureyri University Hospital IS-600 Akureyri Iceland E-mail: [email protected] ISSN 1652-8220 ISBN 978-91-86443-87-0 Lund University, Faculty of Medicine Doctoral Dissertation Series 2010:71 Printed in Sweden Mediatryck, Lund 2010 To Hlíf Atli Egill and Jóhann Jonas Franklin 1 Contents List of papers, 2 Radiographic techniques, 17 Radiographic classification, 17 Definitions and abbreviations, 3 Statistical methods, 17 Thesis at a glance, 4 Ethics, 18 Description of contributions, 6 Data encryption and protection of the individual, 18 Introduction, 7 Symptoms and signs of osteoarthritis, 7 Summary of results of papers I-V, 19 Natural history of osteoarthritis, 8 Discussion, 24 Radiographic features of osteoarthritis, 8 Research methodology, 24 Definition of osteoarthritis, 9 Abnormal mechanical loading is a risk factor for Definition of hip fractures, 9 OA, 25 Study methodology, 9 Natural history of OA, 27 Epidemiology of osteoarthritis, 11 OA and hip fracture, 28 Epidemiology of hip fractures, 11 Conclusions, 30 Risk factors for osteoarthritis ,12 Summary, 31 Risk factors for hip fracture, 13 Populärvetenskaplig sammanfattning på Aims, 14 svenska, 33 Patients and methods, 15 Ágrip á íslensku, 35 Overview of patient/subject allocation, 15 Acknowledgements, 37 Patient identification, 15 References, 38 Populations examined, 16 2 Osteoarthritis - Epidemiologic and genetic aspects List of papers This thesis is based on the following papers: I. -

Coracoid Process Anatomy: a Cadaveric Study of Surgically Relevant Structures Jorge Chahla, M.D., Ph.D., Daniel Cole Marchetti, B.A., Gilbert Moatshe, M.D., Márcio B
Quantitative Assessment of the Coracoacromial and the Coracoclavicular Ligaments With 3-Dimensional Mapping of the Coracoid Process Anatomy: A Cadaveric Study of Surgically Relevant Structures Jorge Chahla, M.D., Ph.D., Daniel Cole Marchetti, B.A., Gilbert Moatshe, M.D., Márcio B. Ferrari, M.D., George Sanchez, B.S., Alex W. Brady, M.Sc., Jonas Pogorzelski, M.D., M.H.B.A., George F. Lebus, M.D., Peter J. Millett, M.D., M.Sc., Robert F. LaPrade, M.D., Ph.D., and CAPT Matthew T. Provencher, M.D., M.C., U.S.N.R. Purpose: To perform a quantitative anatomic evaluation of the (1) coracoid process, specifically the attachment sites of the conjoint tendon, the pectoralis minor, the coracoacromial ligament (CAL), and the coracoclavicular (CC) ligaments in relation to pertinent osseous and soft tissue landmarks; (2) CC ligaments’ attachments on the clavicle; and (3) CAL attachment on the acromion in relation to surgically relevant anatomic landmarks to assist in planning of the Latarjet procedure, acromioclavicular (AC) joint reconstructions, and CAL resection distances avoiding iatrogenic injury to sur- rounding structures. Methods: Ten nonpaired fresh-frozen human cadaveric shoulders (mean age 52 years, range 33- 64 years) were included in this study. A 3-dimensional coordinate measuring device was used to quantify the location of pertinent bony landmarks and soft tissue attachment areas. The ligament and tendon attachment perimeters and center points on the coracoid, clavicle, and acromion were identified and subsequently dissected off the bone. Coordinates of points along the perimeters of attachment sites were used to calculate areas, whereas coordinates of center points were used to determine distances between surgically relevant attachment sites and pertinent bony landmarks. -

Lunate Flattening in Rheumatoid Wrists
Central Annals of Orthopedics & Rheumatology Research Article *Corresponding author Ryogo Nakamura, Nagoya Hand Center, Chunichi Hospital, 3-12-3 Marunouchi, Naka-ku, Nagoya 460- Lunate Flattening in 0002, Japan, Email: Submitted: 04 February 2014 Accepted: 28 May 2014 Rheumatoid Wrists Published: 30 May 2014 Ryogo Nakamura1, Satoshi Niwa1, Sayako Takahashi1, Etushiro Copyright © 2014 Nakamura et al. Naka1 and Masahiro Tatebe2* 1Nagoya Hand Center Chunichi Hospital, Nagoya, Japan OPEN ACCESS 2Hand and Microsurgery Center Anjo Kosei Hospital, Japan Abstract Lunate flattening was studied in 36 patients (62 wrists) with rheumatoid arthritis (RA) who were age- and gender-matched to people with normal wrists. The carpal height ratio (CHR) and lunate compression ratio (LCR; lunate height/ lunate diameter×100, Ståhl index) were measured from wrist radiographs of both groups and the lunate flattening ratio (LFR) was calculated by dividing the LCR by the CHR. The LFR reflects lunate flattening compared to carpal collapse. Twenty-four wrists underwent MRI study. T1-weighted images were evaluated for bone necrosis of the lunate. Results: the normal LFR value obtained from normal wrists ranged from 79.9 to 113.5 (mean±2SD). Lunates with RA could be classified into three groups by LFR values- lunates with a LFR above 113.5 (10 wrists, 16%), lunates with a LFR within the normal range (34 wrists, 55%), and lunates with a LFR lower than 79.9 (18 wrists, 29%). Twelve (50%) of the 24 wrists that underwent MRI study showed a low signal of the lunate in T1-weighted images showing osteonecrosis. Although a satisfactory cor- relation was not confirmed between a LFR value and a low signal on T1-weighted im- ages, lunate avascular necrosis was suspected to play a role in flattening of the lunate. -

A Thesis Entitled the Effects of Radial Core Decompression on Lunate
A Thesis entitled The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering Dr. Mohamed Samir Hefzy, Committee Chair Dr. Vijay Goel, Committee Member Dr. Michael Dennis, Committee Member Dr. Abdul-Azim Mustapha, Committee Member Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo May 2012 Copyright 2012, Andrew E. Smith This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering The University of Toledo May 2012 Kienbocks disease causes degeneration of the lunate bone in the wrist leading to pain and reduced function of the joint. Clinical studies have found a new technique, radial core decompression (RCD) to be clinically effective in improving early stage Kienbock's disease. However, there have been no biomechanical studies characterizing the changes in wrist kinematics following the RCD procedure. The purpose of this study is to determine the changes in lunate and scaphoid motions following the RCD procedure. This study employs an electromagnetic 3-dimensional tracking system, Polhemus 3-SPACE to measure the motions of the lunate, scaphoid, and third metacarpal in four cadaveric specimens. Specimens were partially dissected and sutures were attached to five major tendons used for wrist motion. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

Single Screw Type of Lag Screw Results Higher Reoperation Rate in the Osteosynthesis of Basicervical Hip Fracture
Journal of Orthopaedic Science xxx (xxxx) xxx Contents lists available at ScienceDirect Journal of Orthopaedic Science journal homepage: http://www.elsevier.com/locate/jos Original Article Single screw type of lag screw results higher reoperation rate in the osteosynthesis of basicervical hip fracture * Jung-Taek Kim a, Yong-Chan Ha b, Chan-Ho Park c, Jun-Il Yoo d, Tae-Young Kim e, a Ajou University Hospital, Department of Orthopaedic Surgery, 164, World cup-ro, Yeongtong-gu, Suwon-si, Gyeonggi-do, 16499, South Korea b Chung-Ang University, College of Medicine, Department of Orthopaedic Surgery, 102, Heukseok-ro, Dongjak-gu, Seoul, 06973, South Korea c Yeungnam University Medical Center, Department of Orthopedic Surgery, 170, Hyeonchung-ro, Nam-gu, Daegu, 42415, South Korea d Gyeongsang National University Hospital, Department of Orthopaedic Surgery, 79, Gangnam-ro, Jinju, Gyeongsangnam-do, 52727, South Korea e Konkuk University Medical Center, Department of Orthopaedic Surgery, School of Medicine, Konkuk University, 120-1, Neungdong-ro, Gwangjin-gu, Seoul, 05030, South Korea article info abstract Article history: Background: Basicervical hip fractures are relatively rare with greater biomechanical instability Received 8 January 2019 compared to the other types of hip fractures. Several studies have reported ambivalent surgical outcomes Received in revised form of basicervical hip fractures. The purpose of this multicenter study was to analyze surgical outcomes of 7 February 2019 basicervical hip fractures according to the fixation type of proximal femur and lag screw type. Accepted 12 February 2019 Methods: Among 3220 hip fractures, 145 were classified as basicervical hip fractures. Of those, 106 Available online xxx patients treated with osteosynthesis were included to analyze the surgical complications according to fixation type of proximal femur: sliding hip screw(SHS) and cephalomedullary nail (CMN) groups. -

Ulnar Variance and the Shape of the Lunate Bone a Radiological Investigation
ULNAR VARIANCE AND THE SHAPE OF THE LUNATE BONE A RADIOLOGICAL INVESTIGATION A. H. SCHUURMAN1, M. MAAS2, P. F. DIJKSTRA2, J. M. G. KAUER3 The authors designed a study to test the hypothesis Ulnar variance is the roentgenographic difference that the length of the ulna might affect the shape of of the length of the ulna relative to the radius. the lunate bone because of long-term molding during Positive ulna variance or ulna plus refers to an ulna life. This might then be useful to predict the presence longer than the radius, while the opposite is true in or absence of a dynamic or static ulna plus by the the ulna minus or negative ulnar variance. shape of the lunate bone. Obermann (6) correlated lunate shape and ulnar In a prospective study, posterior-anterior wrist xrays length in 68 patients. Although he found a 13% were taken in a standard fashion in 68 patients with a mean age of 34.5 years. Dominance, grip strength, incidence of type 1, 62% type 2 and 25% type 3, he ulnar variance and the shape of the lunate were found no correlation between type 1 and ulna recorded. length (even distribution in all). Type 2 was found Lunate shape, type 1, which is the least molded, was less often in the ulna minus group and type 3 was seen most frequently on both the left and right side most often found in the ulna plus group. Unfortu- and did not correlate with the dominant side. The nately no statistical analysis was performed. -

Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child
ISSN: 2469-5726 Roberts et al. J Rheum Dis Treat 2018, 4:063 DOI: 10.23937/2469-5726/1510063 Volume 4 | Issue 2 Journal of Open Access Rheumatic Diseases and Treatment CASE REPORT Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child with Systemic Lupus Erythematosus Roberts DC1*, Jester A1, Southwood T2, Johnson K3 and Oestreich K1 1 Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK Check for 2Department of Rheumatology, Birmingham Children’s Hospital, UK updates 3Department of Radiology, Birmingham Children’s Hospital, UK *Corresponding author: Darren Roberts, Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK, E-mail: [email protected] We present, to our knowledge, the first case of syn- Abstract chronous lunate and triquetral AVN in a child with SLE. Avascular necrosis is a known complication of systemic lu- The aetiology and management of carpal AVN in child- pus erythematosus. We report an unusual case of avas- cular necrosis affecting both the lunate and triquetrum in a hood SLE are also discussed based on the available lit- child with this condition. Vasculitis, synovitis and IgM anti- erature. cardiolipin antibodies were probable predisposing factors. The use of arthroscopic synovial debridement improves Case Report symptoms even in the presence of carpal chondromalacia and potentially delays the need for salvage surgery. A 14-year-old girl, diagnosed with SLE five years pre- viously, presented with a two-year history of non-trau- Introduction matic pain and stiffness of her right dominant wrist. She was able to write and self-care, however she was unable Avascular necrosis (AVN) of the carpus typically af- to partake in hand-held ball and racquet sports at school.