Reprint Paper* Canine Atopic Dermatitis: Detailed Guidelines for Diagnosis and Allergen Identification
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Secretary's Pages
SECRETARY ’S PAGES MISSION STATEMENT The American Kennel Club is dedicated to upholding the ATTENTION DELEGATES integrity of its RMegIisStrSy, IpOroNmo ting the spSorTt Aof TpEurMebrEeNd dT ogs and breeding for type and function. ® NOTICE OF MEETING TFohuen Admederiin ca1n8 8K4e, ntnhelAKC Cluba nisd dites daicffailtieadte td o ourpghaonlidziantgio nths ea idnvteogcarittey foofr iths e Rpeugriset brrye, dp rdoomgo atisn ga tfhame islyp ocrot mofpapnuiroenb,r ead vdaongcs e acnad nibnree ehdeianlgthf oarndty pwe elal-nbd eifnugn,c wtioonrk. to protect the rights of all Fdougn odwedneinrs1 a8n8d4 ,ptrhoe mAKCote raensd piotns saifbflieli adtoegd orwgnaenrizsahtipio. ns advocate for the pure bred dog as a family companion, advance canine health and well-being, work to protect the rights of all The next meeting of the Delegates will be held dog owners and 805prom1 oAtrec ore Csopropnosribaltee dDorgiv oew, Snueirtseh 1ip0. 0, Raleigh, NC 276 17 101 Park Avenue, New York, NY 10178 at the Doubletree Newark Airport Hotel on 8051 Arco Corporate Drive, Suite 100, Raleigh, NC 276 17 Raleigh, NC Customer Call Center ..............................................................(919) 233-9767 260 Madison Avenue, New York, NY 10016 10, 2020, beginning no earlier New York, NY Office ...................................................................................(212) 696-8200 Tuesday, March Raleigh, NC Customer Call Center ..............................................................(919) 233-9767 9:00 a.m Fax .............................................................................................................(212) -

J This Week Two Sections 20 Pages COVERING Arne
UONliOUTH JO. HISTORICAL. ASS!| . , f a s s a o u ) . »HV.f.. J ■ X This Week COVERING / TOVVNSHIPB OF Two Sections HOLMDEL, MADISON MARLBORO, MATAWAN AND 20 Pages MATAWAN BOROUGH Member Member 90th YEAR — 15th WEEK National Editorial Association MATAWAN, N. J., THURSDAY, OCTOBER 9, 1958 New Jeney Preu Asiodition Single Copy Ten CenU Arne Kalma Test Cleanup Day Salary Ordinance Something Has Been Added At MHS Football Field Sawmill In Residential Zone On MatawanCoancUwoman Mrs. Genevieve Donnell announced Semi-Finalist Tuesday that the semt-a a n u a 1 Gains Adoption Middlesex Rd. Finally Rejected ‘,Cieanup OayJHa Matawan wtH 10,000 Highest To be held ThursdayrOctn«r“ An Township Sets Madison Township Committee Rules Out Compete Once Again residents of the borough are urg Date For Vote Recommendation For Zoning Variance i ed to co-operate .by making a Principal Luther Foster of Mata general cleanup campaign in An ordinance establishing a max Nn sawmill will be located and wan High School announced that their cellars and attics. imum range of salaries for mem Miss Joan Visits operated on the lands of Frederick Arne Kalma, a senior student, has Cleanup day presents an oppor nnd Wllllnm Formnn, Middlesex been named a semi-finalist in the tunity (or borough residents to bers of the police department, rep Nearly 1000 youngsters nnd Rd. Mnyor Jolm L. Clinmborlaln 1958-59 National Merit Scholarship dear out trash and refuse which resenting an Increase of $700 per adults overflowed the J. J. New nniiounccd thnt the township com- competition. will be carted away by the gar man, was introduced yesterday by berry Co., storo, West Front St., inlttec Monday wns awuro tlie run- As a Kemi-finalist. -
2017 Horrible Hundred Report
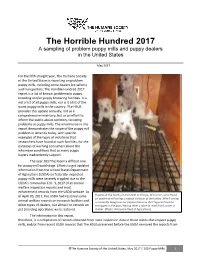
The Horrible Hundred 2017 A sampling of problem puppy mills and puppy dealers in the United States May 2017 For the fifth straight year, The Humane Society of the United States is reporting on problem puppy mills, including some dealers (re-sellers) and transporters. The Horrible Hundred 2017 report is a list of known, problematic puppy breeding and/or puppy brokering facilities. It is not a list of all puppy mills, nor is it a list of the worst puppy mills in the country. The HSUS provides this update annually, not as a comprehensive inventory, but as an effort to inform the public about common, recurring problems at puppy mills. The information in this report demonstrates the scope of the puppy mill problem in America today, with specific examples of the types of violations that researchers have found at such facilities, for the purposes of warning consumers about the inhumane conditions that so many puppy buyers inadvertently support. The year 2017 has been a difficult one for puppy mill watchdogs. Efforts to get updated information from the United States Department of Agriculture (USDA) on federally-inspected puppy mills were severely crippled due to the USDA’s removal on Feb. 3, 2017 of all animal welfare inspection reports and most enforcement records from the USDA website. As of April 20, 2017, the USDA had restored some Puppies at the facility of Alvin Nolt in Thorpe, Wisconsin, were found on unsafe wire flooring, a repeat violation at the facility. Wire flooring animal welfare records on research facilities and is especially dangerous for puppies because their legs can become other types of dealers, but almost no records on entrapped in the gaps, leaving them unable to reach food, water or pet breeding operations were restored. -

Anglo-American Blood Sports, 1776-1889: a Study of Changing Morals
University of Massachusetts Amherst ScholarWorks@UMass Amherst Masters Theses 1911 - February 2014 1974 Anglo-American blood sports, 1776-1889: a study of changing morals. Jack William Berryman University of Massachusetts Amherst Follow this and additional works at: https://scholarworks.umass.edu/theses Berryman, Jack William, "Anglo-American blood sports, 1776-1889: a study of changing morals." (1974). Masters Theses 1911 - February 2014. 1326. Retrieved from https://scholarworks.umass.edu/theses/1326 This thesis is brought to you for free and open access by ScholarWorks@UMass Amherst. It has been accepted for inclusion in Masters Theses 1911 - February 2014 by an authorized administrator of ScholarWorks@UMass Amherst. For more information, please contact [email protected]. ANGLO-AMERICAN BLOOD SPORTS, I776-I8891 A STUDY OF CHANGING MORALS A Thesis Presented By Jack William Berryman Submitted to the Graduate School of the University of Massachusetts in partial fulfillment of the requirements for the degree of MASTER OF ARTS April, 197^ Department of History » ii ANGLO-AMERICAN BLOOD SPORTS, 1776-1889 A STUDY OF CHANGING MORALS A Thesis By Jack V/illiam Berryman Approved as to style and content by« Professor Robert McNeal (Head of Department) Professor Leonard Richards (Member) ^ Professor Paul Boyer (I'/iember) Professor Mario DePillis (Chairman) April, 197^ ACKNOWLEDGMENTS Upon concluding the following thesis, the many im- portant contributions of individuals other than myself loomed large in my mind. Without the assistance of others the project would never have been completed, I am greatly indebted to Professor Guy Lewis of the Department of Physical Education at the University of Massachusetts who first aroused my interest in studying sport history and continued to motivate me to seek the an- swers why. -

Successful Medical Management of Tracheal Collapse and Cardiomegaly in a Dog Is Reported
Journal of Entomology and Zoology Studies 2021; 9(1): 1222-1224 E-ISSN: 2320-7078 P-ISSN: 2349-6800 Successful medical management of tracheal www.entomoljournal.com JEZS 2021; 9(1): 1222-1224 collapse and cardiomegaly in a dog © 2021 JEZS Received: 22-11-2020 Accepted: 24-12-2020 NG Amith, GK Chetan Kumar and L Ranganath NG Amith PG Scholar, Department of Abstract Surgery and Radiology, Veterinary College, Hebbal, A six year old female dog was presented to Department of Veterinary Surgery and Radiology, Veterinary Bangalore, Karnataka, India College, Hebbal, Bangalore with history of open mouth breathing, cough and exercise intolerance. Based on clinical signs, electrocardiographic and radiographic findings case was diagnosed as tracheal collapse GK Chetan Kumar with cardiomegaly. Dog was successfully managed with steroids, ACE inhibitors and chondroitin Assistant Professor, Department sulphate for more than eight months. of Veterinary Medicine, Veterinary College, Hebbal, Keywords: tracheal collapse, cardiomegaly, exercise intolerance, ACE inhibitors Bangalore, Karnataka, India Introduction L Ranganath Professor and Head, Department Tracheal collapse is a progressive, dorsoventral flattening of the tracheal lumen. It is most of Surgery and Radiology, common in middle-aged, small toy breed dogs like Yorkshire terrier, toy poodle, pomeranian, Veterinary College, Hebbal, chihuahua, pug (Hedlund, 1991) [6] and it is characterized by degeneration of the hyaline Bangalore, Karnataka, India cartilage rings and weakening of the dorsal trachealis muscle (Ettinger, 2010) [3]. This condition is a common cause of cough and airway obstruction in dogs but it is very rare in cats [4] (Foley and Krarup, 1991) . Cardiac diseases are also commonly associated with tracheal [9] collapse (Nelson, 2003) . -

The Blue in “Pit Bull”
Info shared by Pitbull SA. Manjaro APBT kennel. South Africa. My Website www.pitbullsa.co.za My E mail “[email protected]” My Facebook “Gawie Manjaro” My Facebook page “Manjaro Kennel” My mobile +27827838280. Zello.com “VoIP” – ask for info. The blue in “pit bull”. The blue in “pit bull” became a point of controversy. Various information extracts about the “Blue” in Pitbull’s – as with so many reasoning’s about “out” breed, this is what we have to work or deal with. Wayne D. Brown's book “History of the American Pit bull terrier” - on pages 25 and 26 he notes: That in the late 1930's one of the most important bloodlines of Pit Bulls was the Lightner dogs. He illustrates that in the conventions of 1936 and 1937, there were Lightner dogs of the dark variety and Lightner dogs of the red nose variety, and a classic confrontation of the two. When Bob Hemphill wrote to Lighter that they were going to use Hall's Searcy Jeff, of the red nose Lightner strain, in the Oklahoma Convention of 1936 at Medicine Park Oklahoma, Lightner wrote back that the red nose blood in Jeff was as game was would ever be bred and, further that the black and blue breeding in (Runyon's Colorado) Imp (II) was as game as would ever be bred. So, the contest between Hall's Searcy Jeff and Runyon's Colorado Imp II at the Oklahoma Convention of 1936 was a classic confrontation between the red nose Lightner dogs and the dark and blue Lightner dogs. -

Rougaroux Rum – Named for the Cajun Werewolf
LDAF assistant commissioner presented with 2017 Cox Conserves Hero Award >>page 20 VOL. 101, No. 2 www.LDAF.la.gov January 18, 2018 Rougaroux Rum – named for the Cajun werewolf “The story is so mysterious, just like our rum!” By Veronica Mosgrove Louisiana folklore is the inspiration behind Donner and whiskey named LA-1 referencing the first legally Peltier Distillers (DPD) Rougaroux Rum – named for made whiskey in Louisiana since prohibition. DPD is the Cajun werewolf. the only distillery in North America to use long grain “People love hearing the story about the Loup rice to make vodka which is typically potato based. Garoux which is the French word for werewolf. They The rice comes from Acadia Rice Mill in Rayne, La. get all into it,” said Danielle Stein, acting distillery The gin boasts citrus notes from Louisiana satsumas manager. “The story is so mysterious, just like our and other citrus. “As a small business, you don’t want rum!” to do anything that’s already been done. You want to The legend –and there are many versions- is that the do something that stands out.” And stand out it does. mythical creature has the body of a man, the face of “We’ve won several awards at spirit competitions. a wolf and six fingers on both hands. He lives in the We only participate in competitions where we are up swamp or a cane field and only comes out at night. The against well known vodkas and rums,” said Stein. distillery sits in the middle of a sugar cane field. -
Domestic Dog Breeding Has Been Practiced for Centuries Across the a History of Dog Breeding Entire Globe
ANCESTRY GREY WOLF TAYMYR WOLF OF THE DOMESTIC DOG: Domestic dog breeding has been practiced for centuries across the A history of dog breeding entire globe. Ancestor wolves, primarily the Grey Wolf and Taymyr Wolf, evolved, migrated, and bred into local breeds specific to areas from ancient wolves to of certain countries. Local breeds, differentiated by the process of evolution an migration with little human intervention, bred into basal present pedigrees breeds. Humans then began to focus these breeds into specified BREED Basal breed, no further breeding Relation by selective Relation by selective BREED Basal breed, additional breeding pedigrees, and over time, became the modern breeds you see Direct Relation breeding breeding through BREED Alive migration BREED Subsequent breed, no further breeding Additional Relation BREED Extinct Relation by Migration BREED Subsequent breed, additional breeding around the world today. This ancestral tree charts the structure from wolf to modern breeds showing overlapping connections between Asia Australia Africa Eurasia Europe North America Central/ South Source: www.pbs.org America evolution, wolf migration, and peoples’ migration. WOLVES & CANIDS ANCIENT BREEDS BASAL BREEDS MODERN BREEDS Predate history 3000-1000 BC 1-1900 AD 1901-PRESENT S G O D N A I L A R T S U A L KELPIE Source: sciencemag.org A C Many iterations of dingo-type dogs have been found in the aborigine cave paintings of Australia. However, many O of the uniquely Australian breeds were created by the L migration of European dogs by way of their owners. STUMPY TAIL CATTLE DOG Because of this, many Australian dogs are more closely related to European breeds than any original Australian breeds. -
1990.5421.Pdf
FILE NO. EL—4 BY—LAW NO. 5421/90 A By-law to amend By-law No. 2443/79 being The Pound By-law. WHEREAS following an extensive review and consideration of submissions to it , Council has determined that it is necessary to regulate and control existing Pit Bull dogs, and prohibit the keeping or harbouring of any more such dogs, as hereinafter set forth, for the health, safety and welfare of the public; NOW THEREFORE THE CITY OF WINNIPEG, in Council assembled, enacts as follows: 1. Clause (e) of Section 16 of By-law No. 2443/79 is amended by deleting the phrase “of this By-law” at the end thereof and substituting therefor “or pursuant to Section 20.2 of this By law”. 2. Section 16 of By-law No. 2443/79 is further amended by adding at the end thereof the following clause: “ (g) “Pit Bull dog” means (i) Pit Bull Terrier; or (ii) Staffordshire Bull Terrier; or (iii) American Staffordshire Terrier; or (iv) American Pit Bull Terrier; or (v) Any dog which has the appearance and physical characteristics predominantly conform ing to the standards for any of the above breeds, as established by the Canadian Kennel Club or the American Kennel Club or the United Kennel Club and attached as Schedule B, as determined by a veterinarian licensed to practice in Manitoba.” 3. By-law No. 2443/79 is further amended by adding immedi ately following Section 20.1 the following: By—law No. 5421/90 — 2 — “20.2 PIT BULL DOGS: (1) Notwithstanding subsections 20.1(1) to 20.1(8) inclusive, any Pit Bull dog within the City of Winnipeg is and shall be conclusively deemed a dangerous dog. -

Basenji Extensions
AUSTRALIAN NATIONAL KENNEL COUNCIL Extended Breed Standard of THE AMERICAN STAFFORDSHIRE TERRIER Original production by the Staffordshire Terrier Club of America Inc. Australian format produced by the ANKC with permission granted and approved by the Staffordshire Terrier Club of America Inc. Copyright Australian National Kennel Council 2006 Standard adopted by the American Kennel Club June 10, 1936 Standard adopted by the ANKC 1987 Amended 2002 FCI Standard No 286 adopted September 3, 1996 Breed Standard Extension adopted by ANKC 2006 Country of origin — USA Extended Standards are compiled purely for the purpose of training Australian judges and students of the breed. In order to comply with copyright requirements of authors, artists and photographers of material used, the contents must not be copied for commercial use or any other purpose. Under no circumstances may the Standard or Extended Standard be placed on the Internet without written permission of the ANKC. THOSE STUDYING THIS BREED STANDARD EXTENSION SHOULD NOTE: Australian law prohibits the cropping of ears; this practice is also prohibited by ANKC Regulations. For these reasons all reference to cropped ears has been deleted from the text. Cropped eared illustrations have, however, been used in the Breed Standard Extension to demonstrate other characteristics of the breed. HISTORY OF THE AMERICAN STAFFORDSHIRE TERRIER The ancient ancestors of the Am Staffs are the mastiff type dogs who appear in many breed histories. Although much of this information is lost in antiquity, we know from early art of the large heavy -headed strong dogs who were used throughout history for their strength and guarding abilities. -

Canine Breed-Specific Risks of Frequently Diagnosed Diseases at Veterinary Teaching Hospitals
CANINE BREED-SPECIFIC RISKS OF FREQUENTLY DIAGNOSED DISEASES AT VETERINARY TEACHING HOSPITALS C. Richard Dorn, D.V.M., M.P.H. Professor Emeritus Department of Veterinary Preventive Medicine College of Veterinary Medicine Ohio State University 1900 Coffey Road Columbus, OH 43210 and Science Officer AKC Canine Health Foundation P.O. Box 37941 Raleigh, NC 27627-7941 Introduction: Knowledge of the risk of various diseases in specific dog breeds is very useful in developing a differential diagnosis list compatible with clinical signs presented by the patient. Veterinary practice experience provides an impression of breed specific disease frequency that is useful in creating an initial prioritization of the differential diagnosis list. Published case series containing disease frequency data provide a qualitative impression of morbidity and is used to focus attention on specific diseases in specific breeds. Unfortunately, quantitative canine morbidity data, including incidence rates and relative risk estimates, are sparse compared to those available in human medicine. Population-at- risk denominators are required for calculation of disease-specific and breed-specific incidence rates. Because there is no periodic, standardized census of dogs to provide the population denominator data required for incidence rates, dog population surveys must be conducted within the same time period that the disease reports are being collected1-2, or a cohort of initially healthy dogs must be followed over time so that their disease occurrence can be ascertained in order to calculate incidence rates.3 Comparison groups are required for estimates of relative risk, such as Odds Ratio analysis, but they have not been previously used to compare the relative risk of diseases of dog breeds. -

2019 Horrible Hundred
The Horrible Hundred 2019 A sampling of problem puppy mills and puppy sellers in the United States For the seventh year in a row, the Humane Society of the United States is publishing a list of 100 problem puppy mills and dog sellers. The 2019 Horrible Hundred is a list of problem dealers in the United States that the HSUS is aware of, published annually to warn consumers about common problems at puppy mills, and to urge government oversight agencies, such as the United States Department of Agriculture, to live up to their enforcement obligations. It is not a list of the worst operations, because many puppy mills are not inspected at all and thus operate in secrecy. Since our last report was published in May 2018, some of the dealers listed in that report appear to have closed their doors, including the notorious Laughlin Kennel (Robert Fink) in Massachusetts, Georgia Puppies (Craig Gray aka Reason Gray) in Georgia, and Samples Creek Kennel (Pam Baldwin) in Missouri. A few other Missouri dealers, including Pup 4 U, aka Cedercrest Kennel (Marilyn Shepherd aka Above: State inspectors found filthy conditions and an emaciated Marilyn Williams), have been penalized by the Great Dane at D and S Puppies in Cumby, Texas. The operation state, but appear to still be operating as of the markets its puppies on Facebook and at flea markets. /TX Dept of Agriculture, 2018 time of this report. Missouri has a history of allowing problem kennels to continue to operate on a smaller scale even after they have been penalized and downsized.