Livedoid Vasculopathy Further Evidence for Procoagulant Pathogenesis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Review Cutaneous Patterns Are Often the Only Clue to a a R T I C L E Complex Underlying Vascular Pathology
pp11 - 46 ABstract Review Cutaneous patterns are often the only clue to a A R T I C L E complex underlying vascular pathology. Reticulate pattern is probably one of the most important DERMATOLOGICAL dermatological signs of venous or arterial pathology involving the cutaneous microvasculature and its MANIFESTATIONS OF VENOUS presence may be the only sign of an important underlying pathology. Vascular malformations such DISEASE. PART II: Reticulate as cutis marmorata congenita telangiectasia, benign forms of livedo reticularis, and sinister conditions eruptions such as Sneddon’s syndrome can all present with a reticulate eruption. The literature dealing with this KUROSH PARSI MBBS, MSc (Med), FACP, FACD subject is confusing and full of inaccuracies. Terms Departments of Dermatology, St. Vincent’s Hospital & such as livedo reticularis, livedo racemosa, cutis Sydney Children’s Hospital, Sydney, Australia marmorata and retiform purpura have all been used to describe the same or entirely different conditions. To our knowledge, there are no published systematic reviews of reticulate eruptions in the medical Introduction literature. he reticulate pattern is probably one of the most This article is the second in a series of papers important dermatological signs that signifies the describing the dermatological manifestations of involvement of the underlying vascular networks venous disease. Given the wide scope of phlebology T and its overlap with many other specialties, this review and the cutaneous vasculature. It is seen in benign forms was divided into multiple instalments. We dedicated of livedo reticularis and in more sinister conditions such this instalment to demystifying the reticulate as Sneddon’s syndrome. There is considerable confusion pattern. -

Clinical Manifestations and Management of Livedoid Vasculopathy
Clinical Manifestations and Management of Livedoid Vasculopathy Elyse Julian, BS,* Tania Espinal, MBS,* Jacqueline Thomas, DO, FAOCD,** Nason Rouhizad, MS,* David Thomas, MD, JD, EdD*** *Medical Student, 4th year, Nova Southeastern University College of Osteopathic Medicine, Ft. Lauderdale, FL **Assistant Professor, Nova Southeastern University, Department of Dermatology, Ft. Lauderdale, FL ***Professor and Chairman of Surgery, Nova Southeastern University, Ft. Lauderdale, FL Abstract Livedoid vasculopathy (LV) is an extremely rare and distinct hyalinizing vascular disease affecting only one in 100,000 individuals per year.1,2 Formerly described by Feldaker in 1955 as livedo reticularis with summer ulcerations, LV is a unique non-inflammatory condition that manifests with thrombi formation and painful ulceration of the lower extremities.3 Clinically, the disease often displays a triad of livedo racemosa, slow-healing ulcerations, and atrophie blanche scarring.4 Although still not fully understood, the primary pathogenic mechanism is related to intraluminal thrombosis of the dermal microvessels causing occlusion and tissue hypoxia.4 We review a case in which the patient had LV undiagnosed and therefore inappropriately treated for more than 20 years. To reduce the current average five-year period from presentation to diagnosis, and to improve management options, we review the typical presentation, pathogenesis, histology, and treatment of LV.4 Upon physical exam, the patient was found to have the patient finally consented to biopsy. The ACase 62-year-old Report Caucasian male presented in an a wound on the right medial malleolus measuring pathology report identified ulceration with fibrin assisted living facility setting with chronic, right- 6.4 cm x 4.0 cm x 0.7 cm with moderate serous in vessel walls associated with stasis dermatitis lower-extremity ulcers present for more than 20 exudate, approximately 30% yellow necrosis characterized by thick-walled capillaries and years. -

Lessons from Dermatology About Inflammatory Responses in Covid‐19
Received: 2 May 2020 Revised: 14 May 2020 Accepted: 15 May 2020 DOI: 10.1002/rmv.2130 REVIEW Lessons from dermatology about inflammatory responses in Covid-19 Paulo Ricardo Criado1,2 | Carla Pagliari3 | Francisca Regina Oliveira Carneiro4 | Juarez Antonio Simões Quaresma4 1Dermatology Department, Centro Universitário Saúde ABC, Santo André, Brazil 2Dermatology Department, Faculdade de Medicina, Centro Universitário Saúde ABC, Santo André, Brazil 3Pathology Department, Faculdade de Medicina, Universidade de S~ao Paulo, S~ao Paulo, Brazil 4Center of Biological and Health Sciences, State University of Pará, Belém, Brazil Correspondence Professor Paulo Ricardo Criado MD, PhD, Summary Dermatology Department, Centro The SARS-Cov-2 is a single-stranded RNA virus composed of 16 non-structural pro- Universitário Saúde ABC, Rua Carneiro Leao~ 33 Vila Scarpelli, Santo André, SP 09050-430, teins (NSP 1-16) with specific roles in the replication of coronaviruses. NSP3 has the Brazil. property to block host innate immune response and to promote cytokine expression. Email: [email protected] NSP5 can inhibit interferon (IFN) signalling and NSP16 prevents MAD5 recognition, depressing the innate immunity. Dendritic cells, monocytes, and macrophages are the first cell lineage against viruses' infections. The IFN type I is the danger signal for the human body during this clinical setting. Protective immune responses to viral infec- tion are initiated by innate immune sensors that survey extracellular and intracellular space for foreign nucleic acids. In Covid-19 the pathogenesis is not yet fully under- stood, but viral and host factors seem to play a key role. Important points in severe Covid-19 are characterized by an upregulated innate immune response, hypercoagulopathy state, pulmonary tissue damage, neurological and/or gastrointes- tinal tract involvement, and fatal outcome in severe cases of macrophage activation syndrome, which produce a ‘cytokine storm’. -

Livedoid Vasculopathy – Benefit of Intravenous Immunoglobulin in A
CASE REPORTS Ref: Ro J Rheumatol. 2021;30(1) DOI: 10.37897/RJR.2021.1.4 LIVEDOID VASCULOPATHY – BENEFIT OF INTRAVENOUS IMMUNOGLOBULIN IN A REFRACTORY CASE Stefan Cristian Dinescu1, Andreea Lili Barbulescu2, Paulina Lucia Ciurea1, Roxana Mihaela Dumitrascu3, Beatrice Andreea Chisalau3, Cristina Dorina Parvanescu3, Sineta Cristina Firulescu4, Florentin Ananu Vreju1 1 Department of Rheumatology, University of Medicine and Pharmacy, Craiova, Romania 2 Department of Pharmacology, University of Medicine and Pharmacy, Craiova, Romania 3Doctoral School, University of Medicine and Pharmacy, Craiova, Romania 4 Department of Rheumatology, Emergency County Hospital, Craiova, Romania Abstract Livedoid vasculopathy is a rare vascular disease which typically manifests as recurrent ulcerative lesions on the lower extremities. It is classified as a vasculopathy, not a true vasculitis, and defined as a vasooclusive syndrome, caused by non-inflammatory thrombosis of the upper and mid-dermal venulae. Main disorders associated with LV include thrombophilias, autoimmune diseases and neoplasia. A triad of clinical features is present in most patients and consist of livedo racemosa (less frequently livedo reticularis), ulcerations and atrophie blanche. Management generally relies on antiplatelet drugs, anticoagulants, vasodilators and fibrinolytic therapy. Some benefit has been observed with intravenous immunoglobulin, colchicine, hyperbaric oxygen, while glucocorticoids are efficient to a lesser extent. This case report highlights a refractory clinical form with no identifiable predisposing condition, which proved responsive only to intravenous immunoglobulin. Keywords: thrombosis, purpura, ulcer, intravenous immunoglobulins INTRODUCTION cal form with no identifiable predisposing condition, which proved responsive only to intravenous immu Livedoid vasculopathy (LV) is a rare vascular dis noglobulin. ease which typically manifests as recurrent ulcerative lesions on the lower extremities. -

PRES Abstracts 1-99
17th Pediatric Rheumatology European Society Congress September 9-12, 2010 València, Spain Abstracts Page no. Oral Abstracts (1 – 36) xxx Poster Abstracts (1 – 306) xxx Clinical and Experimental Rheumatology 2011; xx: xxx-xxx. Oral abstracts 17th Pediatric Rheumatology European Society Congress Oral Abstracts RESULTS: This study had >80% to detect an odds ratio >1.25 for SNPs with allele frequencies >0.1. Two SNPs in the MVK gene, rs1183616 (ptrend=0.006 OR 1.17 95% CI 1.04-1.30) and rs7957619 (ptrend=0.005 OR 1.23 95% CI 1.07- O 01 1.43) are significantly associated with JIA. These two SNPs are in modest linkage Distinctive gene expression in patients with juvenile spondylo- disequilibrium (r2=0.36, D’=1). Logistic regression of the two SNPs, after condi- arthropathy is related to autoinflammatory diseases tioning on the most significant SNP, found that the rs1183616 SNP was no longer significant (p=0.3), suggesting that the association is a single effect driven by the Marina Frleta, Lovro Lamot, Fran Borovecki, Lana Tambic Bukovac, Miroslav rs7957619 SNP. This SNP lies within exon 3 of the MVK gene and is a Serine to Harjacek Asparagine substitution at position 52. There was no significant evidence of a dif- Children’s Hospital Srebrnjak, Srebrnjak, Zagreb, Croatia ference in allele frequencies between the seven ILAR subtypes for the rs7957619 SNP (p=0.32). INTRODUCTION: Juvenile Spondyloarthropathies (jSpA) are characterized by One SNP at the 3’ end of the TNFRSF1A gene, which actually lies within the dysregulation of the inflammatory processes and bone metabolism which may be adjacent gene SLCNN1A, rs2228576, was associated with protection from JIA clarified by gene expression profiles. -

Livedoid Vasculopathy
r e v b r a s r e u m a t o l . 2 0 1 6;5 6(6):554–556 REVISTA BRASILEIRA DE REUMATOLOGIA w ww.reumatologia.com.br Case report ଝ Livedoid vasculopathy Vasculopatia livedoide a a,∗ b José Roberto Provenza , Lucas Eduardo Pedri , Gabriel Mesquita Provenza a Pontifícia Universidade Católica de Campinas, Hospital e Maternidade Celso Pierro, Servic¸o de Reumatologia, Campinas, SP, Brazil b Pontifícia Universidade Católica de Campinas, Hospital e Maternidade Celso Pierro, Servic¸o de Radiologia, Campinas, SP, Brazil a r t i c l e i n f o Article history: Received 18 September 2014 Accepted 25 September 2015 Available online 19 March 2016 Introduction Case report Livedoid vasculopathy (LV) is a recurrent, chronic and painful Female patient, 60, married, tradeswoman. Twelve years ago, skin disease, characterized by lesions that arise as punctate or this patient began a clinical picture of bilateral ulcers in her lenticular purple-colored macules and/or papules occurring in legs and feet, accompanied by color changes, with intense the lower limbs (lower third of the legs and ankles), which worsening in cold weather. Initially, the superficial ulcers were commonly progress to ulceration, and subsequently heal few in number, with a gradual increase in their number and slowly over weeks or months, giving rise to pearly atrophic depth. The patient had no other systemic and/or joint com- scars (white atrophy), punctate telangiectasia, and brownish plaint, no comorbidities, and no family history of rheumatic 1–3 pigmentation, accompanied by a racemous livedo. disease. The disease usually settles bilaterally in the legs, often On physical examination, no change in cardiac, pulmonary causing edema in the lower third of the limbs. -

Livedoid Vasculopathy: a French Observational Study Including
Livedoid Vasculopathy: A French Observational Study Including Therapeutic Options Emma Gardette, Philippe Moguelet, Jean David Bouaziz, Dan Lipsker, Olivier Dereure, François Le Pelletier, Catherine Lok, Thierry Maisonobe, Didier Bessis, Jacqueline Conard, et al. To cite this version: Emma Gardette, Philippe Moguelet, Jean David Bouaziz, Dan Lipsker, Olivier Dereure, et al.. Live- doid Vasculopathy: A French Observational Study Including Therapeutic Options. Acta Dermato- Venereologica, Society for Publication of Acta Dermato-Venereologica, 2018, 98 (9), pp.842 - 847. 10.2340/00015555-2965. hal-01901846 HAL Id: hal-01901846 https://hal.sorbonne-universite.fr/hal-01901846 Submitted on 23 Oct 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License 842 CLINICAL REPORT Livedoid Vasculopathy: A French Observational Study Including DV Therapeutic Options Emma GARDETTE1, Philippe MOGUELET2, Jean David BOUAZIZ3, Dan LIPSKER4, Olivier DEREURE5, François LE PELLETIER6, cta Catherine LOK7, -
Livedo Reticularis: an Enigma Shirish R
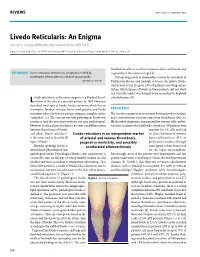
REVIEWS IMAJ • VOL 17 • FebruAry 2015 Livedo Reticularis: An Enigma Shirish R. Sangle MBBS MD and David P. D’Cruz MD FRCP Lupus Research Unit, Guy’s and St Thomas’ Hospital NHS Foundation Trust and Kings College Medical School, London, UK livedoid vasculitis is used for cutaneous ulcers with livedo and KEY WORDS: livedo reticularis, thrombosis, pregnancy morbidity, is generally of the racemosa type [4]. accelerated atherosclerosis, livedoid vasculopathy Certain drugs such as amantadine used in the treatment of IMAJ 2015; 17: 104–107 Parkinson’s disease and multiple sclerosis can induce livedo, which may occur in up to 28% of patients receiving aman- tadine. Skin biopsies of livedo in these patients did not show any vasculitis and it was thought to be secondary to depleted ivedo reticularis, as the name suggests, is a livedoid discol- catecholamines [5]. L oration of the skin in a reticular pattern. In 1907 Ehrmann described two types of livedo: livedo racemosa which has an incomplete (broken) reticular lattice work pattern, and livedo PREVALENCE reticularis where the reticular pattern comprises complete circles The first description of an association between livedo reticularis (unbroken) [1]. The concept was that pathological livedo was and cerebrovascular accidents came from Sneddon in 1965 [6]. racemosa and the reticularis pattern was non-pathological. He described six patients, one man and five women, with cerebro- However, in clinical practice there is no clear-cut differentiation vascular accidents who had livedo reticularis. All patients were between these forms of livedo, negative for LE cells and had and often “livedo reticularis” Livedo reticularis is an independent marker no clinical features of systemic is the term used to describe all of arterial and venous thrombosis, lupus erythematosus (SLE) or types of livedo. -

Cytokine and Platelet P-Selectin Studies
STUDY Livedo Vasculopathy vs Small Vessel Cutaneous Vasculitis Cytokine and Platelet P-Selectin Studies Massimo Papi, MD; Biagio Didona, MD; Ornella De Pita`, MD; Alessandra Frezzolini, PhD; Stefano Di Giulio, MD; Walter De Matteis, MD; Domenico Del Principe, MD; Rino Cavalieri, MD Objective: To assess the role of platelets and lymphocyte- both LV (1.24 ± 0.46 IU/mL [mean ± SD] vs 0.46 ± 0.24 related immunological mechanisms in livedo vasculopa- IU/mL, P,.001; 899 ± 368 IU/mL vs 628 ± 132 IU/mL, thy (LV) and cutaneous small vessel vasculitis (CSVV). P<.02) and CSVV (0.91 ± 0.57 IU/mL, P,.02; 1087 ± 451 Livedo vasculopathy is thought to be related to the throm- IU/mL, P,.001) than in those from the healthy con- botic occlusion of small and medium-sized dermal ves- trols. The serum levels of IL-1b, TNF-a, and IL-8 were sels. Cutaneous small vessel vasculitis comprises a het- higher in patients with CSVV than in controls (7.53 ± erogeneous group of disorders in which the main 6.7 pg/mL vs 4.58 ± 2.72 pg/mL; 23.7 ± 12.6 pg/mL vs pathogenetic events could be modulated by circulating 10.82 ± 2.46 pg/mL, P,.001; 37.8 ± 46 pg/mL vs 8.25 ± cytokines. 3.53 pg/mL, P,.02, respectively). No significant differ- ence in the serum levels of IL-1b (7.2 ± 4.9 pg/mL), TNF-a Design: Case series study of 2 groups of patients af- (12.9 ± 3.47 pg/mL), and IL-8 (5.9 ± 4.13 pg/mL) was fected respectively with LV and CSVV. -

Cutaneous Vasculitis
Cutaneous Vasculitis Authors: Lorinda Chung, M.D. and David Fiorentino1, M.D., Ph.D. Creation date: March 2005 Scientific editor: Prof Loïc Guillevin 1Department of Dermatology, Division of Rheumatology and Immunology, Stanford University School of Medicine, 900 Blake Wilbur Drive W0074, Stanford, CA. USA. [email protected] Abstract Keywords Definition Classification / Etiology Approach to the Patient Treatment Future Directions References Abstract Cutaneous vasculitis is a histopathologic entity characterized by neutrophilic transmural inflammation of the blood vessel wall associated with fibrinoid necrosis, termed leukocytoclastic vasculitis (LCV). Clinical manifestations of cutaneous vasculitis occur when small and/or medium vessels are involved. Small vessel vasculitis can present as palpable purpura, urticaria, pustules, vesicles, petechiae, or erythema multiforme-like lesions. Signs of medium vessel vasculitis include livedo reticularis, ulcers, subcutaneous nodules, and digital necrosis. The frequency of vasculitis with skin involvement is unknown. Vasculitis can involve any organ system in the body, ranging from skin-limited to systemic disease. Although vasculitis is idiopathic in 50% of cases, common associations include infections, inflammatory diseases, drugs, and malignancy. The management of cutaneous vasculitis is based on four sequential steps: confirming the diagnosis with a skin biopsy, evaluating for systemic disease, determining the cause or association, and treating based on the severity of disease. Keywords Cutaneous vasculitis, leukocytoclastic vasculitis Definition Vasculitis is inflammation of the blood vessel Classification / Etiology wall that leads to various clinical manifestations The classification schemes for the vasculitides depending on which organ systems are involved. are based on several criteria, including the size Cutaneous vasculitis is a histopathologic entity of the vessel involved, clinical and characterized by neutrophilic transmural histopathologic features, and etiology. -

Atrophie Blanche: Is It Associated with Venous Disease Or Livedoid Vasculopathy?
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2014 Atrophie blanche: Is it associated with venous disease or livedoid vasculopathy? Alavi, Afsaneh ; Hafner, Jurg ; Dutz, Jan P ; Mayer, Dieter ; Sibbald, R Gary ; Criado, Paulo Ricardo ; Senet, Patricia ; Callen, Jeffery P ; Phillips, Tania J ; Romanelli, Marco ; Kirsner, RobertS Abstract: PURPOSE: The purpose of this learning activity is to provide information about the etiology and treatment of atrophie blanche. TARGET AUDIENCE: This continuing education activity is intended for physicians and nurses with an interest in skin and wound care. OBJECTIVES: After participating in this educational activity, the participant should be better able to:1. Discuss the pathophysiology of atrophie blanche.2. Explore treatment options for livedoid vasculopathy. ABSTRACT: Atrophie blanche (AB) is a porcelain-white scar that may be seen at the base of a healed ulcer or in association with livedoid vasculopathy (LV). The term AB originally had been used synonymously with LV, whereas LV is a noninflammatory thrombotic condition presenting as either a primary or secondary event (often associated with coagulation). DOI: https://doi.org/10.1097/01.ASW.0000455098.98684.95 Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-106873 Journal Article Published Version Originally published at: Alavi, Afsaneh; Hafner, Jurg; Dutz, Jan P; Mayer, Dieter; Sibbald, R Gary; Criado, Paulo Ricardo; Senet, Patricia; Callen, Jeffery P; Phillips, Tania J; Romanelli, Marco; Kirsner, Robert S (2014). Atrophie blanche: Is it associated with venous disease or livedoid vasculopathy? Advances in Skin Wound Care, 27(11):518-524. -

Review Skin Changes Are One of the Earliest Signs of Venous a R T I C L E Hypertension
p-p - ABSTRACT Review Skin changes are one of the earliest signs of venous A R T I C L E hypertension. Some of these changes such as venous eczema are common and easily identified whereas DERMATOLOGICAL other changes such as acroangiodrmatitis are less common and more difficult to diagnose. Other vein MANIFESTATIONS OF VENOUS related and vascular disorders can also present with specific skin signs. Correct identification of these DISEASE: PART I skin changes can aid in making the right diagnosis and an appropriate plan of management. Given KUROSH PARSI, the significant overlap between phlebology and Departments of Dermatology, St. Vincent’s Hospital and dermatology, it is essential for phlebologists to be Sydney Children’s Hospital familiar with skin manifestations of venous disease. Sydney Skin & Vein Clinic, This paper is the first installment in a series of 3 Bondi Junction, NSW, Australia and discusses the dermatological manifestations of venous insufficiency as well as other forms of vascular ectasias that may present in a similar Introduction fashion to venous incompetence. atients with venous disease often exhibit dermatological Pchanges. Sometimes these skin changes are the only clue to an appropriate list of differential diagnoses. Venous ulceration. Less common manifestations include pigmented insufficiency is the most common venous disease which purpuric dermatoses, and acroangiodermatitis. Superficial presents with a range of skin changes. Most people are thrombophlebitis (STP) can also occur in association with familiar with venous eczema, lipodermatosclerosis and venous incompetence but will be discussed in the second venous ulcers as manifestations of long-term venous instalment of this paper (Figure 2).