Procreative Liberty and Harm to Offspring in Assisted Reproduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1 Setting up Offspring Pairing
SETUP GUIDE Indicator Scale Weigh XR5000 the using pairing Offspring Offspring pairing XR5000 Weigh Scale Indicator The offspring pairing feature allows a breeder to link offspring to a dam so they can look up an animal's lineage. This feature is intended to be used in a workflow where the Dam ID is entered first and then its offspring IDs are entered. You can achieve the following with this feature: • Link a Dam with its current offspring and record into the offspring lifetime information • Record other information for the offspring and/or Dam such as DOB, Breed • Optionally record weights either by connecting to a load cell/ load bar or by manually entering • Look up the statistics of the lambing (or calving) percentages to monitor reproductive performance Note: This feature is only available on the XR5000 model. 1 Setting up offspring pairing 1. Go to the Settings screen. 2. Press 3. In the Weight Recording drop down list, select Offspring Pairing. 4. Go to the Weigh screen to start. In offspring pairing mode, you will notice some changes to the Weigh screen: • The right hand pane provides status information on the current Dam. • The size of the weight has been reduced and you have the option to manually enter a weight. • The left hand pane remains the same as in other modes. You can configure what information you want to display and record. • A new soft key is displayed that you use to set or clear the Dam. • A table at the bottom of the screen provides a quick view of the last four records. -

Psychosocial Consequences in Offspring of Women with Breast Cancer
Received: 6 August 2019 Revised: 11 October 2019 Accepted: 14 November 2019 DOI: 10.1002/pon.5294 PAPER Psychosocial consequences in offspring of women with breast cancer Arlene Chan1,2 | Christopher Lomma1 | HuiJun Chih3 | Carmelo Arto1 | Fiona McDonald4,5 | Pandora Patterson4,5 | Peter Willsher1 | Christopher Reid3 1Breast Cancer Research Centre-WA, Medical Oncology, Nedlands, Western Australia, Abstract Australia Objective: Breast cancer (BC) accounts for 24% of female cancers, with approxi- 2 School of Medicine, Curtin University, mately one quarter of women likely to have offspring aged less than 25 years. Recent Bentley, Perth, Western Australia, Australia 3School of Public Health, Curtin University, publications demonstrate negative psychosocial well-being in these offspring. We Bentley, Perth, Western Australia, Australia prospectively assessed for psychological distress and unmet needs in offspring of BC 4 CanTeen Australia, Sydney, New South patients. Wales, Australia Methods: Eligible offspring aged 14 to 24 years were consented and completed the 5Cancer Nursing Research Unit, University of Sydney, Sydney, New South Wales, Australia Kessler-10 Questionnaire and Offspring Cancer Needs Instrument. Demographic and BC details were obtained. Correspondence Chan Arlene, School of Medicine, Curtin Results: Over a 7-month period, 120 offspring from 74 BC patients were included. University, Kent Street, Bentley, Perth, Fifty-nine mothers had nonmetastatic BC (nMBC), and 27 had metastatic BC (MBC) Western Australia 6102, Australia with median time from diagnosis of 27.6 and 36.1 months, respectively. The preva- lence of high/very high distress was 31%, with significantly higher scores reported by female offspring (P = .017). Unmet needs were reported by more than 50% of off- spring with the majority of needs relating to information about their mother's cancer. -

NT Drama Prospectus AUS-NZ 2020 V2 130819
2020 Drama Aust/NZ Students COURSE PROSPECTUS TABLE OF CONTENTS Section One - Introduction and General Information .................................................................. 3 Section Two - Schools and Course Information .............................................................................. 5 Part 1 - National Theatre Ballet School ............................. Error! Bookmark not defined. Part 3- National Theatre Student Policies ..................................................................................... 12 Section Four - Application Process ................................................................................................... 21 Section Five - RTO information .......................................................................................................... 23 The National Theatre Melbourne RTO: 3600 Page 2 of 23 Cricos 01551E Section One – Welcome to the National Theatre Hello and a very warm welcome to the National Theatre Drama School. Creativity is a natural human expression. It’s a necessity for human evolution. At the National we seek to nurture and encourage this creativity. Einstein said, “It’s not that I’m so smart, it’s just that I stay with the problems longer.” We commit to you and your training over a three year period. Because creative artists need time. Time to grow, develop and mature. You need to invest the time to discover the artist you want to be. Our creative staff have been producing and nurturing artists since 1936, making us Australia’s original actor training academy. We employ working actors, directors and teachers who train our students with knowledge of the real world and all its demands. The caring and supportive nature of our staff is second to none. The training at the National is up-to-date, comprehensive and fresh. You will draw upon the teachings of Stanislavski, Mike Alfreds and Michael Chekhov. Classes include Shakespearean text, Suzuki, American text, Theatre creation, Film, TV and new media training, Yoga, Clown and voice and body work. -

The Countdown To 1,000 Chicks Is On!
FOR IMMEDIATE RELEASE CONTACT: Jane Ballentine 26 October 2017 O: 443/552-5275 C: 301/332-1742 THE COUNTDOWN TO 1,000 CHICKS IS ON! --Maryland Zoo welcomes first penguin chicks of the 2017-2018 breeding season-- BALTIMORE, MD – The Maryland Zoo in Baltimore is excited to announce the hatching of two African penguin chicks – the first to hatch during the 2017-2018 breeding season at Penguin Coast. The chicks, which hatched on October 13 and 14, are being reared behind-the-scenes in the Penguin Conservation Center. One chick is being reared by its parents while the other is being hand-reared by the staff. “This breeding season is off to a wonderful start,” said Jen Kottyan, avian collection and conservation manager. “As soon as the nest boxes were made available to the penguins, they began exhibiting breeding behaviors and claiming their nests. We are really excited about the prospects for this season, and these two are just the beginning.” This breeding season at The Maryland Zoo could mark the first time that any zoo or aquarium in North America has hatched 1,000 African penguin chicks during the course of their history with the birds. “Since we began working with African penguins in 1967, the Zoo has successfully hatched 989 penguin chicks, which includes the two we are announcing today,” continued Kottyan. “If our penguin pairs hatch eleven more healthy chicks this season, then we will hit the 1,000 mark. Spoiler alert – we have several more eggs incubating under their parents right now! We really have high hopes of hatching at least eleven chicks, if not more, this season.” The Maryland Zoo has been a leader in African penguins for 50 years, winning the prestigious Edward H. -

Should This Dog Be Called Spot?
SHOULD THIS DOG BE CALLED SPOT? Imagine this microscopic drama. A sperm cell from a male dog fuses with an egg cell from a female dog. Each dog’s gamete carries 39 chromosomes. The zygote that results from the fusion of the gametes contains 78 chromosomes – one set of 39 chromosomes from each parent. One pair of the zygote’s chromosomes is shown below. Chromosome from the female dog L T h A Chromosome from the male dog l T H a Each chromosome of the homologous pair contains alleles for the same traits. But one chromosome may have a dominant allele and the other may have a recessive allele. Use the drawing above and the table below to answer the questions. TRAIT Dominant Gene Recessive Gene Hair length Short (L) Long ( l ) Hair Texture Wiry (T) Silky ( l ) Hair Curliness Curly (H) Straight ( h ) Coat Pattern Spotted (A) Solid ( a ) 1. Will the new puppy have a spotted coat? _ yes ________ Explain why or why not: The puppy inherited the dominant allele for spots from its father. 2. Does the female dog (mother) have a spotted coat? _ not enough info ____ Explain how you know this: _She could have a dominant allele on her other chromosome, which is information we don’t have. _____ _____________________________________________________________________ _____________________________________________________________________ 3. Does the male dog (dad) have a spotted coat? __yes _____ Explain how you know this: _The male has at least one dominant allele that he gave to the puppy so we know that the male is spotted. ______________________________________________________________________ Page 5 4. -
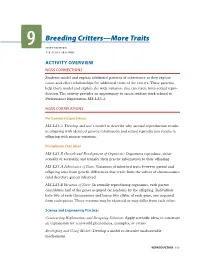
9 Breeding Critters—More Traits
Breeding Critters—More Traits 9 INVESTIGATION 1–2 CLASS SESSIONS ACTIVITY OVERVIEW NGSS CONNECTIONS Students model and explain additional patterns of inheritance as they explore cause-and-effect relationships for additional traits of the critters. These patterns help them model and explain the wide variation that can result from sexual repro- duction. The activity provides an opportunity to assess student work related to Performance Expectation MS-LS3-2. NGSS CORRELATIONS Performance Expectations MS-LS3-2: Develop and use a model to describe why asexual reproduction results in offspring with identical genetic information and sexual reproduction results in offspring with genetic variation. Disciplinary Core Ideas MS-LS1.B Growth and Development of Organisms: Organisms reproduce, either sexually or asexually, and transfer their genetic information to their offspring. MS-LS3.A Inheritance of Traits: Variations of inherited traits between parent and offspring arise from genetic differences that result from the subset of chromosomes (and therefore genes) inherited. MS-LS3.B Variation of Traits: In sexually reproducing organisms, each parent contributes half of the genes acquired (at random) by the offspring. Individuals have two of each chromosome and hence two alleles of each gene, one acquired from each parent. These versions may be identical or may differ from each other. Science and Engineering Practices Constructing Explanations and Designing Solutions: Apply scientifc ideas to construct an explanation for real-world phenomena, examples, or events. Developing and Using Models: Develop a model to describe unobservable mechanisms. REPRODUCTION 155 ACTIVITY 9 BREEDING CRITTERS—MORE TRAITS Crosscutting Concepts Patterns: Patterns can be used to identify cause and effect relationships. -
SUMMER 2018 Sibling and Offspring Camp What Is a PICC-Line?
SUMMER 2018 A MAGAZINE FOR KIDS WHO HAVE CF AND THEIR SIBLINGS A Day in the Life of: Brandan What is a PICC-Line? Going to School with a PICC Line: David What is Cross-infection? Crazy Hair Day Sibling and Offspring Camp How to Make: A Smoothie Bowl 1ALL AWESOME! EDITOR: Gillian Hoyland Editor’s Letter CONTRIBUTORS: Katrina, Brandan, Welcome to the 6th edition of Rozee! David, Zoe, Zac, In this edition, we learn all about PICC Blake and Natalie. lines- what are they, what activities can/ ON THE FRONT COVER: can’t you do with one in, and we even Siblings Cam, Brandan hear from an adult with CF about her and Addi experiences with PICC lines. PRINTED BY: We also talk about anxiety. Anxiety is Picton Press very normal and common for many pictonpress.com.au people to experience. It can be described DESIGN: as butterflies or a knot in your stomach. We talk about what you can do to minimise and cope with these feelings. Function Creative functioncreative.com.au We have some member interviews, including Brandan from York, who shares a day in his life, as well as a couple of interviews from kids who went on our Sibling and Offspring Camp. Rozee Magazine There are also lots of fun sections, CFWA including a craft activity, puzzles, PO Box 959 and a recipe. So, take a look inside! Nedlands WA 6909 Bye for now, P. 08 6457 7337 E. [email protected] Gillian W. www.cysticfibrosiswa.org.au/wa P.S. We hope you have a wonderful Christmas Disclaimer This magazine is edited and and happy school holidays too. -

Why We Should Create Artificial Offspring: Meaning and the Collective Afterlife
Why we should create artificial offspring: meaning and the collective afterlife By John Danaher, NUI Galway Forthcoming in Science and Engineering Ethics This article argues that the creation of artificial offspring could make our lives more meaningful (i.e. satisfy more meaning-relevant conditions of value). By ‘artificial offspring’ is meant beings that we construct, with a mix of human and non-human-like qualities. Robotic artificial intelligences are paradigmatic examples of the form. There are two reasons for thinking that the creation of such beings could make our lives more meaningful. The first is that the existence of a collective afterlife — i.e. a set of human-like lives that continue in this universe after we die — is likely to be an important source and sustainer of meaning in our present lives (Scheffler 2013). The second is that the creation of artificial offspring provides a plausible and potentially better pathway to a collective afterlife than the traditional biological pathway (i.e. there are reasons to favour this pathway and there are no good defeaters to trying it out). Both of these arguments are defended from a variety of objections and misunderstandings. 1. Introduction This article defends an unusual thesis. An illustration might help. In season 3 of Star Trek: The Next Generation, in an episode entitled “The Offspring”, Lt. Commander Data (an artificial humanoid life-form) decides to create an artificial child of his own. He calls the child “Lal” and gives it the characteristics of a female human. The episode then tells the charming story of Data’s emerging bond with Lal, a bond which is threatened by a group of scientists who try to take her away and study her, and eventually leads to heartbreak as Lal “dies” due to a design fault (though not before Data downloads her memories into his own brain so that a part of her can live on). -

Theatre Costume, Celebrity Persona, and the Archive
Persona Studies 2019, vol. 5, no. 2 THEATRE COSTUME, CELEBRITY PERSONA, AND THE ARCHIVE EMILY COLLETT ABSTRACT This essay considers the archived costume in relation to the concept of the celebrity performer’s persona. It takes as its case study the Shakespearean costume of Indigenous actress Deborah Mailman, housed in the Australian Performing Arts Collection. It considers what the materiality of the theatre costume might reveal and conceal about a performer’s personas. It asks to what extent artefacts in an archive might both create a new persona or freezeframe a particular construct of a performer. Central to the essay are questions of agency in relation to the memorialisation of a still living actress and the problematisation of persona in terms of the archived object. Can a costume generate its own persona in relation to the actress? And what are the power dynamics involved in persona construction when an archived costume presents a charged narrative which is very different to the actress’s current construction of her persona? KEY WORDS Costume; Archive; Deborah Mailman; Indigenous; Memory; Shakespeare COSTUME IN THE ARCHIVE: A CHARGED OBJECT In this essay I consider the archived theatre costume in relation to persona studies and what the materiality of costume might reveal or conceal about the celebrity performer’s persona(s). Can an archived costume have its own persona? What complexities arise when the charged historical narrative of an archived costume is at odds with a current persona? And in the following case study of Deborah Mailman, what happens when the framing of a living Indigenous actress’s costume constructs a persona that is quite different to the one that the actress currently constructs for herself? A costume worn by a performer live on stage is remembered in particular ways – and many in the audience might focus more on the performer’s stance, physicality, and verbal prowess than what they are wearing. -

Publicity Campaigns & Print Advertising
Fashion Stylist & Costume Buyer 0411 343 353 Agent: Freelancers 03 9682 2722 www.anitafitzgerald.com [email protected] Publicity Campaigns & Print Advertising Chrissie Swan & Anh Do Long Lost Family Stylist Publicity stills campaign 2016 Photography: Ben King Jo Stanley & Lehmo Gold FM/ARN Stylist Publicity stills campaign 2016 Photography: Elizabeth Allnutt SIDS & Kids Australia Photographer: Norman Krueger Stylist Safe Sleeping brochure 2016 Nadine Garner, Dr Blake Photography: Narelle Sheean Stylist Publicity stills campaign 2015 Kat Stewart, Mr and Mrs Murder Network Ten Stylist Publicity stills campaign 2013 Photography: Ben King Anthony La Paglia, Underground Network Ten Stylist Publicity stills campaign 2012 Photography: John Tsiavis Asher Keddie, Offspring Network Ten Stylist Publicity stills campaign 2012 Photography: John Tsiavis Carrie Bickmore Sunday Life Magazine Stylist Cover story 2012 Photography: Sam Ruttyn Clare Bowditch The Sunday Age, M Magazine Stylist Cover story 2012 Photography: Simon Schlutter Asher Keddie, Carrie Bickmore, TV Week Magazine Stylist Hamish Blake and TV Week Gold Logie Nominees Adam Hills Photography: Tina Smigielski Cover story 2012 Shaun Micallef, Amanda Keller OK Magazine Stylist Charlie Pickering, Josh Thomas Photography: Tina Smigielski Talking Bout Your Generation Stills 2012 Asher Keddie TV Week Stylist Cover story 2012 Photography: Tina Smigielski Lisa McCune, Matt Day Network Ten, Reef Doctors Stylist Publicity stills campaign 2012 Photography: Ellis Parrinder Kate Langbroek, Dave -

LEGAL TOOLS for URBAN AGRICULTURE in Baltimore City N Io
Legal Tools for Urban A griculture in Baltimore City 1st Edition t Communiity Law Center, Inc.T Acknowledgements: Community Law Center gratefully acknowledges the contributions of the Community Law Center staff, interns, and volunteers for their contributions to this book. The following individuals have provided editorial assistance, prepared charts and sample documents, gathered research, and authored sections of the book: Megan Wakefield, Esq., Kristine Dunkerton, Esq., Becky Witt, Esq., Kelly Pfeifer, Esq., Robin Jacobs, Esq., Shana Roth- Gormley, Esq., Elsa Lankford, Benjamin Smith, Douglas A. Sampson, and David T. Shafer. Community Law Center’s urban agriculture logo is by pr8rdesign. Disclaimer: This book is intended to provide general information and should not be construed as legal advice or legal opinions concerning any specific facts or circumstances. Readers should consult an experienced attorney if advice is required concerning any specific situation or legal matter. The publisher makes no warranties, express or implied, with respect to the information provided herein. IRS Circular 230 Disclosure: The Internal Revenue Service requires disclosure that any tax advice in this book is not intended or written to be used, and cannot be used, by any taxpayer for the purposes of avoiding U.S. federal tax law penalties, or in connection with marketing, promoting, or recommending any transaction in this book to another party. Published by Community Law Center, Inc. About Community Law Center, Inc. Since 1986, Community Law Center, Inc. has been Baltimore’s only legal services organization dedicated solely to strengthening neighborhoods and nonprofits. Community Law Center, a nonprofit law firm, provides legal services to community and nonprofit organizations throughout Maryland to promote stronger nonprofits and more vibrant neighborhoods. -
Baltimore's Forest Patches: Emerald Assets for Ecosystem Services
Baltimore’s Forest Patches June 2013 Baltimore’s Forest Patches: emerald assets For ecosystem services miriam avins Baltimore Green space June 2013 1 Baltimore’s Forest Patches June 2013 Baltimore Green Space gratefully acknowledges support from numerous partners who provided funding or expertise. Thanks are due to the Rauch Foundation; the Fund for Change; The U.S. Forest Service, and most especially David Nowak, Ian Yesilonis, and Jarlath O’Neill-Dunne; the Parks & People Foundation, and particularly Guy Hager; Matthew Baker of the University of Maryland, Baltimore County; Thom Myers; the Baltimore Office of Sustainability and the Departments of Planning and of Public Works, whose staff patiently answered questions; Delegate Mary Washington; and Mike Hudson. We are proud to work and learn with resident forest patch stewards, including Mabel Smith, Charles Brown, Helene Perry, Cathy Browhan, Henashena Hayes, Stephen Cotton, Denise Blackwell, Butch Berry, Janet Abramovitz, and Randy Baker. Miriam Avins particularly thanks Katie Lautar for her research assistance and Jason Hesch for his GIS analysis and map-making. 2 Baltimore’s Forest Patches June 2013 eXecUtive sUMMARY • Forest Patches – areas of canopy at least 10,000 square feet – make up 34 percent of Baltimore’s tree canopy. Twenty percent of Baltimore’s tree canopy is in forest patches outside parks. Trees, and forest patches in particular, provide important ecosystem services such as cleaning stormwater and air, cooling the air, and removing carbon from the atmosphere. They provide food and habitat to wildlife and migratory birds. They can provide a venue for education and community involvement. There is also the potential for agroforestry (growing or harvesting foods and fibers in a forest).