Occupational Interstitial Lung Disease Guideline
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Occupational Airborne Particulates
Environmental Burden of Disease Series, No. 7 Occupational airborne particulates Assessing the environmental burden of disease at national and local levels Tim Driscoll Kyle Steenland Deborah Imel Nelson James Leigh Series Editors Annette Prüss-Üstün, Diarmid Campbell-Lendrum, Carlos Corvalán, Alistair Woodward World Health Organization Protection of the Human Environment Geneva 2004 WHO Library Cataloguing-in-Publication Data Occupational airborne particulates : assessing the environmental burden of disease at national and local levels / Tim Driscoll … [et al.]. (Environmental burden of disease series / series editors: Annette Prüss-Ustun ... [et al.] ; no. 7) 1.Dust - adverse effects 2.Occupational exposure 3.Asthma - chemically induced 4.Pulmonary disease, Chronic obstructive - chemically induced 5.Pneumoconiosis - etiology 6.Cost of illness 7.Epidemiologic studies 8.Risk assessment - methods 9.Manuals I.Driscoll, Tim. II.Prüss-Üstün, Annette. III.Series. ISBN 92 4 159186 2 (NLM classification: WA 450) ISSN 1728-1652 Suggested Citation Tim Driscoll, et al. Occupational airborne particulates: assessing the environmental burden of disease at national and local levels. Geneva, World Health Organization, 2004. (Environmental Burden of Disease Series, No. 7). © World Health Organization 2004 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). -
SIGN158 British Guideline on the Management of Asthma
SIGN158 British guideline on the management of asthma A national clinical guideline First published 2003 Revised edition published July 2019 Key to evidence statements and recommendations Levels of evidence 1++ High-quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias 1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias 1– Meta-analyses, systematic reviews, or RCTs with a high risk of bias 2++ High-quality systematic reviews of case-control or cohort studies High-quality case-control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal 2+ Well-conducted case-control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal 2– Case-control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal 3 Non-analytic studies, eg case reports, case series 4 Expert opinion Grades of recommendation Note: The grade of recommendation relates to the strength of the supporting evidence on which the evidence is based. It does not reflect the clinical importance of the recommendation. A At least one meta-analysis, systematic review, or RCT rated as 1++, and directly applicable to the target population; or A body of evidence consisting principally of studies rated as 1+, directly applicable to the target population, and demonstrating overall consistency of results B A body of evidence including studies rated -
Effects of Indium Exposure on Respiratory Symptoms: a Retrospective Cohort Study in Japanese Workers Using Health Checkup Data
Effects of indium exposure on respiratory symptoms: a retrospective cohort study in Japanese workers using health checkup data Toshiharu Mitsuhashi Center for Innovative Clinical Medicine, Okayama University Hospital, Okayama, Japan ABSTRACT Background. Indium compounds are known health hazards for lung cancer and interstitial pneumonia. Furthermore, they are related to emphysema, alveolar pro- teinosis, and cholesterol granuloma. In Japan, laws were revised in 2013 to tighten regulations on indium exposure in workplaces. However, its impact on the health of workers who handle indium has not been evaluated. This study aimed to investigate whether subjective respiratory symptoms in these workers have reduced after the 2013 amendment in the regulations. Methods. The subjects were workers from certain areas of Japan who had undergone health checkups between January 1, 2013, and June 30, 2015. Indium-handling and non-handling workers were categorized into the exposed and less-exposed groups, respectively. Based on the findings of health checkups during this period, the hazard ratio of subjective respiratory symptoms (cough, sputum production, shortness of breath, and palpitation) and its 95% confidence intervals (CIs) were calculated with the less-exposed group as the reference. The Prentice-Williams-Peterson model was used for calculation, and a model that adjusted for coarse analysis and potential confounding factors was adopted. Results. Overall, 2,561 workers (from 22 companies) who underwent 6,033 health checkups were included. The total person-years were 2,562.8 years, and 162 outcome Submitted 9 October 2019 events occurred. The hazard ratios of the exposed group were 1.65 (95% CI [1.14–2.39]: Accepted 16 December 2019 p D 0:008) and 1.61 (95% CI [1.04–2.50]: p D 0:032) in the crude and adjusted models, Published 15 January 2020 respectively. -

A Professional Development Framework for Paediatric Respiratory Nursing
A professional development framework for paediatric respiratory nursing ISSN 2040-2023: British Thoracic Society Reports Vol 12, Issue 2, May 2021 1 ACKNOWLEDGEMENTS: We are grateful to colleagues at the National Paediatric Respiratory and Allergy Nurses Group (NPRANG) for their support with the development of this document. In particular: Ann McMurray Asthma Nurse Specialist, Royal Hospital for Children and Young People, Edinburgh. NPRANG Chair Bethan Almeida Clinical Nurse Specialist for Paediatric Asthma and Allergy, Imperial College Healthcare NHS Trust Tricia McGinnity Paediatric Cystic Fibrosis Nurse Specialist, Southampton Children's Hospital Emma Bushell Paediatric Respiratory Nurse Specialist – Asthma, Frimley Health NHS Foundation Trust This document has been adapted from the following publication: British Thoracic Society, A professional development framework for respiratory nursing (1). The authors of this original document are: Samantha Prigmore, Co-chair Consultant respiratory nurse, St Georges University Hospitals NHS Foundation Trust Helen Morris, Co-chair ILD nurse specialist, Wythenshawe Hospital Alison Armstrong Nurse consultant (assisted ventilation), Royal Victoria Infirmary Susan Hope Respiratory nurse specialist, Royal Stoke University Hospital Karen Heslop-Marshall Nurse consultant, Royal Victoria Infirmary Jacqui Pollington Respiratory nurse consultant, Rotherham NHS Foundation Trust CONTENTS: Introduction Method of production How to use this document Competency table (Band 5, 6, 7 and 8) Supporting evidence Acknowledgements Declarations of Interest References Content from this document may be reproduced with permission from BTS as long as you conform to the following conditions: • The text must not be altered in any way. • The correct acknowledgement must be included. 2 Introduction Paediatric respiratory nurses are an important component of the multi-professional team for a wide variety of respiratory conditions, providing holistic care for patients in a variety of settings. -

PICTORIAL REVIEW Thoracic Involvement in Connective
JBR–BTR, 2015, 98: 3-19. PICTORIAL REVIEW THORACIC INVOLVEMENT IN CONNECTIVE TISSUE DISEASES: RADIO- LOGICAL PATTERNS AND FOLLOW-UP G. Serra1, A.-L. Brun1, P. Ialongo2, M.-L. Chabi1, P.A. Grenier1 Connective tissue diseases (CTDs) are a heterogeneous group of idiopathic inflammatory diseases involving various organs. A thoracic involvement is frequent, and chest-CT represents the imaging technique of reference in its assess- ment. Pulmonary abnormalities related to CTDs are various; although several disease-specific aspects have been described, the two most clinically relevant complications are represented by interstitial lung disease and pulmonary arterial hypertension. The early identification of a thoracic involvement, with the adoption of specific therapies, can significantly change patient’s prognosis. The aim of this article is to review the most common typical and atypical CT features of thoracic involvement occurring in CT, especially focusing on interstitial lung disease. Key-word: Connective tissue, diseases – Lung, interstitial disease – Hypertension, pulmonary. Connective tissue diseases (CTDs) at the time of diagnosis of CTD, or chronic inflammation in the alveolar are a heterogeneous group of in- more commonly manifest later in the walls. The patients usually response flammatory diseases derived from course of the disease (5, 6). well to corticosteroid therapy and an immunologic deregulation affect- The most common histopatholog- have a good prognosis. However pa- ing various organs. A thoracic in- ic patterns of ILD seen in the setting tients with OP associated with CTD volvement (pulmonary, pleural or of CTDs are non specific interstitial seem to have a greater tendency to mediastinal) can be frequently pneumonia (NSIP), usual interstitial develop fibrosis and a higher mortal- found; its frequency and expression pneumonia (UIP), organizing pneu- ity than patients with cryptogenic depends on the type of disease, and monia (OP), diffuse alveolar damage OP (5, 6). -
17Th & 18Th June 2021 Speakers' Details and Presentation Summaries
th th SUMMER MEETING ONLINE – 17 & 18 June 2021 Speakers’ Details and Presentation Summaries The following details are in programme order. Use the PDF search button to quickly find a session or speaker. OPEN SESSION – NATIONAL ASTHMA AND COPD AUDIT PROGRAMME Thursday 17th June: 08:00-09:00 Dr James Calvert qualified in Medicine from Oxford Session aims and overview University in 1992. He studied Public Health as a 1) To summarise the main findings of the 2020/21 Fulbright Scholar at Harvard University before NACAP reports. completing his PhD in Asthma Epidemiology in South 2) To outline the QI support opportunities offered by Africa and London. NACAP to clinical and audit teams. He was a Consultant Respiratory Specialist in Bristol from 2006-2021. He is now a Respiratory Consultant Professor Roberts will present a summary of key and Medical Director of Aneurin Bevan University reported findings from across the audits from the last Health Board in Wales. 12 months, highlighting areas for further James has worked with colleagues in the South West improvement. He will speak about the impact of and at NHS England to improve access to integrated COVID-19 on standards of care and on audit services for respiratory patients. He has Chaired the participation, along with plans to improve automated British Thoracic Society (BTS) Professional and extraction of NACAP data. Organisational Standards Committee and has been Dr Calvert will talk about the QI programme to be the BTS National Audit Lead. He has a longstanding launched this year. interest in quality improvement in health care and has A discussion will follow around ideas for improving worked with the BTS, NHS Improving Value, the Royal NACAP support to clinical and audit teams. -

Disparities in Respiratory Health
American Thoracic Society Documents An Official American Thoracic Society/European Respiratory Society Policy Statement: Disparities in Respiratory Health 6 Dean E. Schraufnagel, Francesco Blasi, Monica Kraft, Mina Gaga, Patricia Finn, Klaus Rabe This official statement of the American Thoracic Society (ATS) and the European Respiratory Society (ERS) was approved by the ATS Board of Directors, XXXXXXXXX, and by the ERS XXXXXXXX, XXXXXXXXXX [[COMP: Insert internal ToC]] 1 Abstract Background: Health disparities, defined as a significant difference in health between populations, are more common for diseases of the respiratory system than for those of other organ systems because of the environmental influence on breathing and the variation of the environment among different segments of the population. The lowest social groups are up to 14 times more likely to have respiratory diseases than are the highest. Tobacco smoke, air pollution, environmental exposures, and occupational hazards affect the lungs more than other organs and occur disproportionately in ethnic minorities and those with lower socioeconomic status. Lack of access to quality health care contributes to disparities. Methods: The executive committees of the American Thoracic Society (ATS) and European Respiratory Society (ERS) established a writing committee to develop a policy on health disparities. The document was reviewed, edited, and approved by their full executive committees and boards of directors of the societies. Results: This document expresses a policy to address health disparities by promoting scientific inquiry and training, disseminating medical information and best practices, and monitoring and advocating for public respiratory health. ERS and ATS have strong international commitments and work with leaders from governments, academia, and other organizations to address and reduce avoidable health inequalities. -

Management of Malignant Pleural Effusions an Official ATS/STS/STR Clinical Practice Guideline David J
AMERICAN THORACIC SOCIETY DOCUMENTS Management of Malignant Pleural Effusions An Official ATS/STS/STR Clinical Practice Guideline David J. Feller-Kopman*, Chakravarthy B. Reddy*, Malcolm M. DeCamp, Rebecca L. Diekemper, Michael K. Gould, Travis Henry, Narayan P. Iyer, Y. C. Gary Lee, Sandra Z. Lewis, Nick A. Maskell, Najib M. Rahman, Daniel H. Sterman, Momen M. Wahidi, and Alex A. Balekian; on behalf of the American Thoracic Society, Society of Thoracic Surgeons, and Society of Thoracic Radiology THIS OFFICIAL CLINICAL PRACTICE GUIDELINE WAS APPROVED BY THE AMERICAN THORACIC SOCIETY OCTOBER 2018, THE SOCIETY OF THORACIC SURGEONS JUNE 2018, AND THE SOCIETY OF THORACIC RADIOLOGY JULY 2018 Background: This Guideline, a collaborative effort from the MPE; 3) using either an indwelling pleural catheter (IPC) or American Thoracic Society, Society of Thoracic Surgeons, and chemical pleurodesis in symptomatic patients with MPE and Society of Thoracic Radiology, aims to provide evidence-based suspected expandable lung; 4) performing large-volume recommendations to guide contemporary management of patients thoracentesis to assess symptomatic response and lung expansion; with a malignant pleural effusion (MPE). 5) using either talc poudrage or talc slurry for chemical pleurodesis; 6) using IPC instead of chemical pleurodesis in patients with Methods: A multidisciplinary panel developed seven questions nonexpandable lung or failed pleurodesis; and 7) treating using the PICO (Population, Intervention, Comparator, and IPC-associated infections with antibiotics and not removing the Outcomes) format. The GRADE (Grading of Recommendations, catheter. Assessment, Development and Evaluation) approach and the Evidence to Decision framework was applied to each question. Recommendations Conclusions: These recommendations, based on the best available were formulated, discussed, and approved by the entire panel. -

Pneumoconiosis
Prim Care Respir J 2013; 22(2): 249-252 PERSPECTIVE Pneumoconiosis *Paul Cullinan1, Peter Reid2 1 Consultant Physician, Royal Brompton and Harefield NHS Foundation Trust, London, UK 2 Consultant Physician, Western General Hospital, Edinburgh, UK Introduction Figure 1. Asbestosis; the HRCT scan shows the typical The pneumoconioses are parenchymal lung diseases that arise from picture of subpleural fibrosis (solid arrow); in addition inhalation of (usually) inorganic dusts at work. Some such dusts are there is diffuse, left-sided pleural thickening (broken biologically inert but visible on a chest X-ray or CT scan; thus, while arrow), characteristic too of heavy asbestos exposure they are radiologically alarming they do not give rise to either clinical disease or deficits in pulmonary function. Others – notably asbestos and crystalline silica – are fibrogenic so that the damage they cause is through the fibrosis induced by the inhaled dust rather than the dust itself. Classically these give rise to characteristic radiological patterns and restrictive deficits in lung function with reductions in diffusion capacity; importantly, they may progress long after exposure to the causative mineral has finished. In the UK and similar countries asbestosis is the commonest form of pneumoconiosis but in less developed parts of the world asbestosis is less frequent than silicosis; these two types are discussed in detail below. Other, rarer types of pneumoconiosis include stannosis (from tin fume), siderosis (iron), berylliosis (beryllium), hard metal disease (cobalt) and coal worker’s pneumoconiosis. Asbestosis Clinical scenario How is the diagnosis made? Asbestosis is the ‘pneumoconiosis’ that arises from exposure to A man of 78 reports gradually worsening breathlessness; he has asbestos in the workplace.1 The diagnosis is made when, on the no relevant medical history of note and has never been a regular background of heavy occupational exposure to any type of asbestos, smoker. -
Respiratory Function Changes After Asbestos Pleurisy
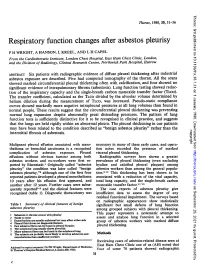
Thorax: first published as 10.1136/thx.35.1.31 on 1 January 1980. Downloaded from Thorax, 1980, 35, 31-36 Respiratory function changes after asbestos pleurisy P H WRIGHT, A HANSON, L KREEL, AND L H CAPEL From the Cardiothoracic Institute, London Chest Hospital, East Ham Chest Clinic, London, and the Division of Radiology, Clinical Research Centre, Northwick Park Hospital, Harrow ABSTRACT Six patients with radiographic evidence of diffuse pleural thickening after industrial asbestos exposure are described. Five had computed tomography of the thorax. All the scans showed marked circumferential pleural thickening often with calcification, and four showed no significant evidence of intrapulmonary fibrosis (asbestosis). Lung function testing showed reduc- tion of the inspiratory capacity and the single-breath carbon monoxide transfer factor (TLco). The transfer coefficient, calculated as the TLCO divided by the alveolar volume determined by helium dilution during the measurement of TLco, was increased. Pseudo-static compliance curves showed markedly more negative intrapleural pressures at all lung volumes than found in normal people. These results suggest that the circumferential pleural thickening was preventing normal lung expansion despite abnormally great distending pressures. The pattern of lung function tests is sufficiently distinctive for it to be recognised in clinical practice, and suggests that the lungs are held rigidly within an abnormal pleura. The pleural thickening in our patients may have been related to the condition described as "benign asbestos pleurisy" rather than the copyright. interstitial fibrosis of asbestosis. Malignant pleural effusion associated with meso- necessary in many of these early cases, and opera- thelioma or bronchial carcinoma is a recognised tion notes recorded the presence of marked http://thorax.bmj.com/ complication of asbestos exposure. -

Occupational Lung Diseases
24 Occupational lung diseases Introduction i Occupational diseases are often thought to be Key points uniquely and specifically related to factors in the work environment; examples of such diseases are • Systematic under-reporting and the pneumoconioses. However, in addition to other difficulties in attributing causation both contribute to underappreciation of the factors (usually related to lifestyle), occupational burden of occupational respiratory exposures also contribute to the development or diseases. worsening of common respiratory diseases, such • Work-related exposures are estimated as chronic obstructive pulmonary disease (COPD), to account for about 15% of all adult asthma and lung cancer. asthma cases. • Boththe accumulation of toxic dust in the Information about the occurrence of occupational lungs and immunological sensitisation respiratory diseases and their contribution to to inhaled occupational agents can morbidity and mortality in the general population is cause interstitial lung disease. provided by different sources of varying quality. Some • Despite asbestos use being phased European countries do not register occupational out, mesothelioma rates are forecast diseases and in these countries, information about to continue rising owing to the long latency of the disease. the burden of such diseases is completely absent. • The emergence of novel occupational In others, registration is limited to cases where causes of respiratory disease in compensation is awarded, which have to fulfil specific recent years emphasises the need for administrative or legal criteria as well as strict continuing vigilance. medical criteria; this leads to biased information and underestimation of the real prevalence. Under- reporting of occupational disease is most likely to occur in older patients who are no longer at work but whose condition may well be due to their previous job. -

Causal Relationship Between Indium Compound Inhalation and Effects on the Lungs
Journal of J Occup Health 2009; 51: 513–521 Occupational Health Causal Relationship between Indium Compound Inhalation and Effects on the Lungs Makiko NAKANO1, Kazuyuki OMAE1, Akiyo TANAKA2, Miyuki HIRATA2, Takehiro MICHIKAWA1, Yuriko KIKUCHI1, Noriyuki YOSHIOKA1, Yuji NISHIWAKI1 and Tatsuya CHONAN3 1Department of Preventive Medicine and Public Health, School of Medicine, Keio University, 2Department of Hygiene, Graduate School of Medical Sciences, Kyushu University and 3Department of Medicine, Nikko Memorial Hospital, Japan Abstract: Causal Relationship between Indium SP-D and SP-A, respectively. Conclusion: Dose- Compound Inhalation and Effects on the Lungs: dependent lung effects due to indium exposure were Makiko NAKANO, et al. Department of Preventive shown, and a decrease of indium exposure reduced Medicine and Public Health, School of Medicine, the lung effects. An In-S value of 3 ng/ml may be a Keio University—Background: Recent case reports cut-off value which could be used to prevent early and epidemiological studies suggest that inhalation of effects on the lungs. indium dust induces lung damage. Objectives: To (J Occup Health 2009; 51: 513–521) elucidate the dose-dependent effects of indium on the lungs and to prove a causal relationship more clearly. Key words: Cross-sectional study, Indium, Interstitial Methods: A baseline observation was conducted on pneumonitis, KL-6, HRCT, SP-D 465 workers currently exposed to indium, 127 workers formerly exposed to indium and 169 workers without Due to the rapid expansion of flat panel displays and indium exposure in 12 factories and 1 research solar cells, indium demand has increased every year, and laboratory from 2003 to 2006.