How to Care for Your Child After Tonsillectomy Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(FNE) and Nasal Endoscopy in Ireland During COVID-19 Pandemic Rev 1
Royal College of Surgeons in Ireland Coláiste Ríoga na Máinleá in Éirinn Interim Clinical Guidance on Flexible Nasendoscopy (FNE) and Nasal Endoscopy in Ireland during COVID-19 pandemic Rev 1 INTERIM CLINICAL GUIDANCE ON FLEXIBLE NASENDOSCOPY (FNE) AND NASAL ENDOSCOPY IN IRELAND DURING COVID-19 PANDEMIC Rev 1 INTERIM CLINICAL GUIDANCE ON FLEXIBLE NASENDOSCOPY (FNE) AND NASAL ENDOSCOPY IN IRELAND DURING COVID-19 PANDEMIC Table of Contents 1. Overview ............................................................................................................................................................................. 2 2. Purpose ............................................................................................................................................................................... 2 3. Authorship ......................................................................................................................................................................... 2 4. Target Audience .............................................................................................................................................................. 2 5. Introduction ....................................................................................................................................................................... 2 6. Risk of infection associated with FNE .................................................................................................................. 2 7. Aerosol Generating Procedures -

Home Care After Sleep Surgery-Uvulopalatopharyngoplasty (UP3) And/Or Tonsillectomy
Home Care after Sleep Surgery-Uvulopalatopharyngoplasty (UP3) and/or Tonsillectomy The above surgeries are all performed on patients to help relieve or lessen the symptoms of sleep apnea. All address the palate, or the upper part of your throat. General Information You may lack energy for several days, and may also be restless at night. This will improve over the next 10 to 14 days. It is quite common to feel progressively worse during the first five to six days after surgery. You may also become constipated during this time for three reasons: you will not be eating a regular diet, you will be taking pain medications, and you may be less active. Wound Care All of the above surgeries are performed within the mouth on the upper throat. No external incisions are made, all are internal. Depending on the surgery, you may feel and/or see some suture on your palate (upper throat). This is normal and will dissolve over the next two weeks. No specific wound care is necessary for these procedures. Diet It is important for you to drink plenty of fluids after surgery. Drink every hour while awake. A soft diet is recommended for the first 14 days (anything that you may eat without teeth constitutes as a soft diet). Avoid hot liquids/solids. It is alright if you don’t feel like eating much, as long as you drink lots of fluids. Signs that you need to drink more are when the urine is darker in color (urine should be pale yellow). A high fever that persists may also be a sign that you are not taking in enough fluids. -

MERCY PROJECT How to Serve As a Small Group
MERCY PROJECT How to Serve as a Small Group In John 13:15, Jesus sets an example for us to follow. After washing His disciples' feet - an act of love, humility, and service - He encourages us to follow His lead and serve one another. "I have set you an example that you should do as I have done for you." "For even the Son of Man did not come to be served, but to serve, and to give his life as a ransom for many." Mark 10:45 "Serve wholeheartedly, as if you were serving the Lord, not men." Ephesians 6:7 “And let us consider how we may spur one another on toward love and good deeds” Hebrews 10:24 If our heart is to serve the least, the last and the lost then we are always looking for opportunities to reach out and serve our community and neighbors. God has shaped your group with unique gifting, passions, abilities, talents and resources. We were saved to serve and have the privilege to be Jesus heart, hands and feet as we help those that are hurting and in need. Your challenge as a group leader is to help people get out of their comfort zones and see that God wants to use them in ministry. I love this quote: “People grow the most when they are serving and taking responsibility. Every task, no matter how small, is an opportunity to serve.” Below is a simple outline to help your group prepare for a Mercy Project. How To PREPARE For Your Mercy Project Pray for God to present an opportunity for your group to reach out and serve others. -
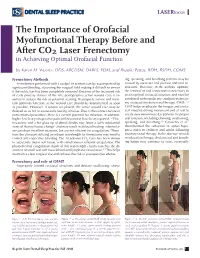
The Importance of Orofacial Myofunctional Therapy Before and After CO2 Laser Frenectomy in Achieving Optimal Orofacial Function
LASERfocus The Importance of Orofacial Myofunctional Therapy Before and After CO2 Laser Frenectomy in Achieving Optimal Orofacial Function by Karen M. Wuertz, DDS, ABCDSM, DABLS, FOM, and Brooke Pettus, RDH, BSDH, COMS Frenectomy Methods ing, speaking, and breathing patterns may be Frenotomies performed with a scalpel or scissors can be accompanied by caused by incorrect oral posture and oral re- significant bleeding, obscuring the surgical field making it difficult to ensure strictions. Therefore, in the authors’ opinion, if the restriction has been completely removed. Because of the increased risk the removal of oral restrictions is necessary to of early primary closure of the site, postoperative active wound care is es- attain optimal orofacial function, and must be sential to reduce the risk of potential scarring. To properly restore and main- combined with regular pre- and post-frenecto- tain optimum function, active wound care should be implemented as soon my orofacial myofunctional therapy (OMT).1,4 as possible. However, if sutures are placed, the active wound care may be OMT helps re-educate the tongue and orofa- delayed so as not to cause early tearing of tissue. Due to the contact nature of cial muscles during movement and at rest to conventional procedure, there is a certain potential for infection; in addition, create new neuromuscular patterns for proper higher levels of postoperative pain and discomfort have been reported.1,2 Elec- oral function, including chewing, swallowing, trocautery and a hot glass tip of dental diodes may leave a fairly substantial speaking, and breathing.5,6 Camacho et al.7 zone of thermal tissue change3 and may result in delayed healing. -

Family Education and Resources Guide
The Family Childbirth & Children’s Center AT MERCY Family Education and Resources Guide Welcome to The Family Childbirth and Children’s Center at Mercy It is our pleasure to take care of you during this very special time. We are dedicated to providing excellent patient care in an atmosphere of safety, comfort, courtesy, and respect. Please feel free to ask us any questions during your stay. This Family Education and Resources Guide provides information you or your family may need during your stay as well as for when you go home. Our nursing staff will point out the items that pertain specifically to you. On behalf of all the doctors and health professionals of The Family Childbirth and Children’s Center, thank you for choosing Mercy for your care. 1 2 Table of Contents About Your Stay ..........................5 Patient Information ............................. 9 Post Partum Care .................................... 21 • Your Room • Visiting Hours • Normal Physical Appearance - Linen Changes - Labor & Delivery • Cramping - Housekeeping (8th floor, The Bunting Center) • Bleeding - Wireless Internet Access - Mother/Baby • Stitches - GetWell Network (10th floor, The Bunting Center) • Cesarean Section - The Mothers Gardens - NICU (8th floor, The Bunting Center) • Controlling Pain Levels - Shift Change - Overnight Visitors • Breast Pain • Your Safety - Brother and Sister Visits • Uterine or Abdominal Pain - Mother and Baby Identification • Chapels • Emptying your Bladder - Fall Prevention - McAuley Chapel • Bowels - Infant Safety Instructions - Chapel of Light • Hemorrhoids • Your Meals • Gift Shops • Constipation - Meal Selection - The Bunting Lobby • Breast Care - Patient Meal Times - The McAuley Lobby • Mood Swings • Understanding MRSA • Cafés • Your Weight and Staying Healthy - What is MRSA? - Corcoran Café - What is infection vs. -

Mercy-Benefits-Exempt.Pdf
2021 Salaried/Exempt Employee Benefits Summary At Mercy Medical Center we value our employees and strive to offer competitive compensation and benefits. We are committed to ensuring both our patients and employees receive The Mercy Touch©. Benefit Description Who is Eligible When Eligible Who Pays Medical Comprehensive medical coverage that Employees 0.5 FTE First of the month following Mercy & Insurance includes physician services, hospitalization, or greater date of employment Employee and prescription drugs. Choose between a HMO and HDHP/HSA. Dental Insurance Comprehensive dental coverage that Employees 0.5 FTE First of the month following Mercy & includes preventative, routine, and major or greater date of employment Employee care/services. Vision Insurance Comprehensive vision coverage that Employees 0.5 FTE First of the month following Employee includes exam, prescription glasses, and or greater date of employment contact lenses. Choose from the Base or Premier Plan. Health Care Flex Opportunity to make pre-tax elections for Employees 0.5 FTE First of the month following Employee Spending qualifying out-of-pocket medical, dental, and or greater date of employment Account vision expenses. Dependent Care Opportunity to make pre-tax elections for Employees 0.5 FTE First of the month following Employee Spending qualifying out-of-pocket dependent care or greater date of employment Account expenses. Short-Term Partial income protection of monthly Employees 0.5 FTE First of the month following Employee Disability earnings for disability after elimination or greater date of employment period. Pays 60% of salary to a max of $1,500 per week. Long-Term Partial income protection of monthly Employees 0.9 FTE First of the month following Mercy Disability earnings for disability after 90-day or greater one year of employment elimination period. -
The Year of Mercy Thoughts for the Catechist by Martha S
The Year of Mercy Thoughts for the Catechist by Martha S. Long Delivered to the Catechetical Leaders of the Diocese of Arlington (CDLA) St. Joseph Catholic Church Herndon, Virginia February 18, 2016 "For His mercy endures forever."(Psalm 136) “He has shown you, O mortal, what is good. And what does the Lord require of you? To act justly and to love mercy and to walk humbly with your God.” (Micah 6:8). The Prodigal Son Pompeo Botoni (1773) I. INTRODUCTION Pope Francis has proclaimed this year as a Jubilee Year of Mercy. This Jubilee year began on the Feast of the Immaculate Conception (December 8, 2015) and will end on the Feast of Christ the King (November 20, 2016). It is a great opportunity for us to grow in faith and grace. Before discussing the mercy of God, let us consider what is meant by a “Jubilee Year.” The idea of a year of jubilee comes from the Old Testament. In the book of Leviticus, the chosen people were instructed to celebrate a jubilee every fifty years. It was a special year in which slaves and prisoners would be freed, debts would be forgiven and the mercies of God would be particularly manifest. Building on this tradition from the Old Covenant, the Church has, throughout her history, often celebrated a Jubilee year as a special year for the remission of sins and universal pardon. Such Jubilees have usually involved pilgrimage to a sacred site, frequently the city of Rome. The most distinctive feature in the ceremonial of the Jubilee is the un-walling and the final walling up of the "holy door" at St. -

2015 Medical Staff Goals It's That Time Again
March 2015 2015 Medical Staff Goals It’s that time again! Dr. Matt Anderson led the Medical Executive Nominate an Outstanding Provider TODAY! Committee membership in a discussion of goals for the coming year. Several goals were discussed, including: • Review and revise all OPPE department scorecards. • Create and implement a proctoring policy. • Establish department quality Matt Anderson, MD improvement initiatives. He also shared that the primary goal for the coming year is to better integrate the work that is being done regarding the quality of our clinical care and its reporting between the formal Medical Staff and the Medical Director Council. The Medical Staff is actively seeking to build a more cohesive framework that will result in greater collaboration between the two groups while enhancing the quality of our care and the means by which we as providers hold each other accountable for advancing the quality of care that we provide at Mercy. ICD-10 coding implementation and the review and revision of The Annual Provider Awards originated in 2003 as a way for Mercy Medical Staff Bylaws and Rules and Regulations will also be a focus. staff and providers to recognize outstanding provider role models and colleagues. Anyone can nominate physicians, nurse practitioners or physician assistants for these exclusive awards. Nominations are WANTED: Chief Medical Information Officer being accepted now through March 13, so submit your nomination Mercy is looking to hire a full-time Chief Medical Information today! Forms can be found on the physician website at p.mercycare. Officer to take the place of Donald Hilliard, M.D. -

Tide-Spring-2016 – a Year of Mercy
Spring 2016 A Year of Mercy Pope Francis has done it again – making history with a jubilee celebration that is having a worldwide impact. His official procla- mation on Divine Mercy Sunday 2015 announced a Year of Mercy that extends from December 2015 to November 2016, the solem- nity of Christ the King. The opening of the Door of Mercy in each diocese symbolically illustrates an extraordinary path to salvation during this time of jubilee. St. Faustina Kosalska is credited for introducing devotion to Jesus in the mid-20th century with the title “Divine Mercy.” [In this issue of the Tide, on the next page, you will see the image of Christ that Faustina saw in her visions of Christ.] His right hand is raised in blessing and his left hand rests on his heart from which two rays of light flow. Jesus told Faustina, “Paint an image according to the pattern you see, with the prayer, Jesus, I trust in you.” She herself could not paint but eventually persuaded her spiritual director to find an artist to create the painting which is entitled The Divine Mercy. By now, as they tell you in the movie theaters, you probably know where the nearest Door of Mercy is – usually in the cathedral, the Bishop’s church in your diocese. Pope Francis’ opening of the Door of Mercy at St. Peter’s in Rome on December 8, 2015, was the first of four to be officially opened in and around Rome. A special path leads toward the Holy Door marking out the path for pilgrims to enter through the “Door of Mercy.” However, the door finds meaning only when the believer associates the door with Christ who has said: “I am the door.” In January, our community gathered in chapel to give expression to a very special act of mercy. -

Tonsillotomy (Partial) and Complete Tonsillectomy
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY TONSILLOTOMY (PARTIAL) & COMPLETE TONSILLECTOMY - SURGICAL TECHNIQUE Klaus Stelter and Goetz Lehnerdt Acute tonsillitis is treated with steroids e.g. first and easiest-to-reach station of the dexamethasone, NSAIDs e.g. ibuprofen and mucosa associated lymphoid tissue system beta-lactam antibiotics e.g. penicillin or cef- (MALT) 2-4. As the main phase of the im- uroxime. Only 10 days of antibiotic therapy mune acquisition continues until the age of has proven to be effective to prevent rheu- 6yrs, the palatine tonsils are physiological- matic fever and glomerulonephritis. ly hyperplastic at this time 5, 6. This is followed by involution, which is reflected Tonsillectomy is only done for recurrent by regression of tonsil size until age 12yrs acute bacterial tonsillitis, or for noninfec- 7. tious reasons such as suspected neoplasia. The lymphoid tissue is separated by a cap- Partial tonsillectomy (tonsillotomy) is the sule from the surrounding muscle (superior 1st line treatment for snoring due to tonsillar pharyngeal constrictor) 8. The blood supply hyperplasia. It is low-risk, and postopera- originates from four different vessels, the tive pain and risk of haemorrhage are much lingual artery, the ascending pharyngeal less than with tonsillectomy. It is immate- artery and the ascending and descending rial whether the tonsillotomy is done with palatine arteries. These vessels radiate laser, radiofrequency, shaver, coblation, bi- mainly to the upper and lower tonsillar polar scissors or monopolar electrocautery, poles, as well as to the centre of the tonsil as long as the crypts remain open and some from laterally 9. -

Some Non-Religious Views Against Proposed 'Mercy-Killing' Legislation Part II Yale Kamisar University of Michigan Law School, [email protected]
University of Michigan Law School University of Michigan Law School Scholarship Repository Articles Faculty Scholarship 1976 Some Non-Religious Views against Proposed 'Mercy-Killing' Legislation Part II Yale Kamisar University of Michigan Law School, [email protected] Available at: https://repository.law.umich.edu/articles/1065 Follow this and additional works at: https://repository.law.umich.edu/articles Part of the Comparative and Foreign Law Commons, Criminal Law Commons, Medical Jurisprudence Commons, and the Natural Law Commons Recommended Citation Kamisar, Yale. "Some Non-Religious Views against Proposed 'Mercy-Killing' Legislation Part II." Hum. Life Rev. 2, no. 3 (1976): 34-63. This Article is brought to you for free and open access by the Faculty Scholarship at University of Michigan Law School Scholarship Repository. It has been accepted for inclusion in Articles by an authorized administrator of University of Michigan Law School Scholarship Repository. For more information, please contact [email protected]. Some Non-Religious Views against Proposed "Mercy-Killing" Legislation Yale Kamisar PART II A Long Range View of Euthanasia A. Voluntary v. Involuntary Euthanasia EVER SINCE the 1870's, when what was probably the first eutha nasia debate of the modern era took place/50 most proponents of the movement-at least when they are pressed-have taken consid erable pains to restrict the question to the plight of the unbearably suffering who voluntarily seeks death while most of their opponents have striven equally hard to frame the issue in terms which would encompass certain involuntary situations as well, e.g., the "congenital idiots," the "permanently insane," and the senile. -

Read Full Article
PEDIATRIC/CRANIOFACIAL Pharyngeal Flap Outcomes in Nonsyndromic Children with Repaired Cleft Palate and Velopharyngeal Insufficiency Stephen R. Sullivan, M.D., Background: Velopharyngeal insufficiency occurs in 5 to 20 percent of children M.P.H. following repair of a cleft palate. The pharyngeal flap is the traditional secondary Eileen M. Marrinan, M.S., procedure for correcting velopharyngeal insufficiency; however, because of M.P.H. perceived complications, alternative techniques have become popular. The John B. Mulliken, M.D. authors’ purpose was to assess a single surgeon’s long-term experience with a Boston, Mass.; and Syracuse, N.Y. tailored superiorly based pharyngeal flap to correct velopharyngeal insufficiency in nonsyndromic patients with a repaired cleft palate. Methods: The authors reviewed the records of all children who underwent a pharyngeal flap performed by the senior author (J.B.M.) between 1981 and 2008. The authors evaluated age of repair, perceptual speech outcome, need for a secondary operation, and complications. Success was defined as normal or borderline sufficient velopharyngeal function. Failure was defined as borderline insufficiency or severe velopharyngeal insufficiency with recommendation for another procedure. Results: The authors identified 104 nonsyndromic patients who required a pharyngeal flap following cleft palate repair. The mean age at pharyngeal flap surgery was 8.6 Ϯ 4.9 years. Postoperative speech results were available for 79 patients. Operative success with normal or borderline sufficient velopharyngeal function was achieved in 77 patients (97 percent). Obstructive sleep apnea was documented in two patients. Conclusion: The tailored superiorly based pharyngeal flap is highly successful in correcting velopharyngeal insufficiency, with a low risk of complication, in non- syndromic patients with repaired cleft palate.