Freedom from Hunger Learning Journey
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dear Friend of Freedom from Hunger, As a Public Health Researcher
Dear Friend of Freedom from Hunger, As a public health researcher and program planner, I have spent much of my career focused on efforts to reduce maternal and child malnutrition. I have been fortunate to work for many excellent organizations from international agencies to small nonprofits. That is how I could recognize what is so potentially effective about the Freedom from Hunger approach. But let me back up. After almost three decades of international work I was discouraged by the magnitude of the problem of child malnutrition. Many approaches to ending hunger were narrowly focused and overly politicized. When I was first introduced to Freedom from Hunger, it was refreshing and exciting to see that they focus on increasing women’s financial access as well as their health and nutrition knowledge. From my work in the field, I know that women play a key role in eliminating malnutrition. Extremely poor, rural women are an untapped resource, but they are as hardworking as any others, with both determination and dreams for their children. On a trip to Burkina Faso with Freedom from Hunger, I met a woman whose small food stand sat under a tarp she had set up. She was busy selling rice and sauces – what I call West African fast food – to passersby. She told me that before she joined her women’s association she could only buy small, more expensive bags of rice. Worse still, sometimes the rice ran out before the day was over. This meant lost business and less money for her family. Thanks to Freedom from Hunger, she could now purchase 50-kilo bags of rice, making each serving of rice less expensive. -

Freedom from Hunger-Integrating Health and Microfinance, UNC Gillings School of Global Public Health, University of North Carolina
Freedom from Hunger-Integrating Health and Microfinance, UNC Gillings School of Global Public Health, University of North Carolina Role: Research Intern to be based in Chapel Hill, North Carolina and Davis, CA Project Lead: Freedom from Hunger Research and Evaluation Specialist Project Stipend: $2,500 from UNC Gillings School of Global Public Health. Student is responsible for his/her own transportation to/from Davis, California and living expenses in Davis. Project Period: Approximately 10-12 weeks between May and August 2013, exact dates negotiable. At least two weeks at Freedom from Hunger International Center, Davis, California. Background: Freedom from Hunger is a forerunner in integrating health protection services and products onto the platform of microfinance in order to reach the rural poor with a sustainable, affordable, reliable and effective mechanism to provide services that will help protect them against financial and health shocks. In 2005–2010, under the first Bill & Melinda Gates Foundation microfinance funding, Freedom from Hunger partnered with 5 MFIs in 5 countries to develop and sustainably offer a package of health protection services that included combinations of health education, health savings, health loans, linkages to health providers and products, and health micro-insurance to improve the health and financial stability of their clients while also contributing to the sustainability of the institutions themselves. Impact research and cost-benefit analyses from the MAHP pilot initiative showed clear and compelling -

No. 34 the Right to Adequate Food
UNITED NATIONS The Right to Adequate Food Human Rights Human Rights Fact Sheet No. 34 The Right to Adequate Food Fact Sheet No. 34 NOTE The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations or the Food and Agriculture Organization of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. Material contained in this publication may be freely quoted or reprinted, provided credit is given and a copy of the publication containing the reprinted material is sent to the Office of the United Nations High Commissioner for Human Rights, Palais des Nations, 8–14 avenue de la Paix, CH–1211 Geneva 10, Switzerland. ii CONTENTS Page Abbreviations . iv Introduction . 1 I. WHAT IS THE RIGHT TO FOOD? . 2 A. Key aspects of the right to food . 2 B. Common misconceptions about the right to food. 3 C. The link between the right to food and other human rights . 5 D. The right to food in international law. 7 II. HOW DOES THE RIGHT TO FOOD APPLY TO SPECIFIC GROUPS?. 9 A. The rural and urban poor . 10 B. Indigenous peoples. 12 C. Women . 14 D. Children. 16 III. WHAT ARE THE OBLIGATIONS ON STATES AND THE RESPONSIBILITIES OF OTHERS? . 17 A. Three types of obligations. 17 B. Progressive and immediate obligations . 19 C. Obligations with international dimensions . 22 D. The responsibilities of others. -
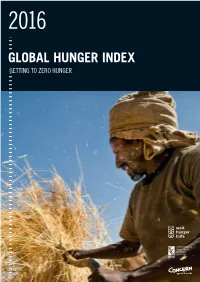
2016 Global Hunger Index Hunger 2016 Global Global Hunger Index Getting to Zero Hunger
2016 2016 GLOBAL2016 HUNGER INDEX GLOBAL HUNGER INDEX GETTING TO ZERO HUNGER INTERNATIONAL FOOD POLICY RESEARCH INSTITUTE IFPRI 2016 GLOBAL HUNGER INDEX GETTING TO ZERO HUNGER International Food Policy Research Institute: Klaus von Grebmer, Jill Bernstein, Nilam Prasai, Shazia Amin, Yisehac Yohannes Concern Worldwide: Olive Towey, Jennifer Thompson Welthungerhilfe: Andrea Sonntag, Fraser Patterson United Nations: David Nabarro Washington, DC/Dublin/Bonn October 2016 INTERNATIONAL FOOD POLICY RESEARCH INSTITUTE A Peer-Reviewed Publication IFPRI Ten-year-old Adeu, from the village of Khaysone in southern Laos, shows off his catch. Laos continues to face serious challenges in undernutrition and hunger. FOREWORD Only one year ago the world united and made history: in hunger, by reaching the most vulnerable first, by prioritizing human September 2015, global leaders pledged themselves to the 2030 rights and empowering women, and by tackling the adverse impacts Agenda for Sustainable Development, a political manifesto that com- of climate change. mits us all to ending poverty and hunger forever. This new Agenda At the heart of the Sustainable Development Goals (SDGs) is a is universal: addressing issues of sustainable development for all renewed commitment to end hunger and global poverty by 2030. countries, while recognizing that each nation will adapt and prior- Through Goal 2, which is a call “to end hunger, achieve food secu- itize the goals in accordance with its own needs and policies. It is rity and improved nutrition, and promote sustainable agriculture,” transformative: proposing action to end poverty and hunger once and and in the other 16 SDGs, the Agenda shows how actions can con- for all, while safeguarding the planet. -
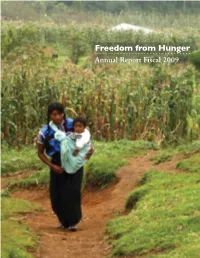
Annual Report Fiscal 2009 Table of Contents
Freedom from Hunger Annual Report Fiscal 2009 Table of Contents Letter from the President. 3 Get Informed. Be Inspired . 3 Progress Report. 4 Meeting the Challenge: How We Made a Difference in FY09 Credit with Education . 5 Microfinance and Health Protection (MAHP). 5 Saving for Change. 5 HealthKeepers . 6 Training, Collaboration and Influence. 6 Proof of Better Health, Better Business. 6 Financial Highlights. 7-10 Donor Spotlight. 8-12 Leadership. 12 Ambassadors Council. 13 2 n the world’s poorest countries, women Get informed. Be Inspired. living in poverty face staggering challenges and heartbreaking choices. As the primary This annual report is just the beginning of the caretakers of young children, they must earn story we have to tell you this year. Explore www.freedomfromhunger.org to get more detail about Imoney to pay for food, medicine and school the accomplishments that are ending hunger for good for fees. These hardworking women shouldn’t be millions of people. further challenged because they are overlooked by microfinance programs that view them as too poor, too rural and too vulnerable to illness. That’s why Freedom from Hunger has rededicated itself to ensuring not only that microfinance reaches the world’s poorest women, but also responds to the realities of their lives by providing more than access to loans and savings accounts. In this past fiscal year, Freedom from Hunger increased the number of women it serves to nearly 1.5 million and further demonstrated Before, when my son had diarrhea, I that microfinance can better meet the needs ‘‘ didn’t know that I should give him plenty of poor women and their families with health of clean water. -

Freedom from Hunger As a Freestanding Right
Yigzaw Final.doc (Do Not Delete) 5/18/14 12:22 AM HUNGER AND THE LAW: FREEDOM FROM HUNGER AS A FREESTANDING RIGHT Destaw A. Yigzaw* I. INTRODUCTION .................................................................. 656 II. WHAT IS HUNGER? ............................................................ 657 A. The Scope of Global Hunger ...................................... 659 B. Manifestations of Hunger .......................................... 660 C. Controversy: Causes of Hunger .................................. 662 D. Consensus: A World without Hunger ........................ 671 III. THE RIGHT TO FOOD AND THE POLITICS OF HUNGER ....... 677 A. Human Rights in Overcoming Hunger ..................... 678 B. Hunger is a Human Right Violation ......................... 682 C. Justiciability of the Right to Food ............................. 688 IV. REINTERPRETING THE RIGHT TO FOOD ............................. 692 A. Interpreting Human Rights ....................................... 693 V. TWO DISTINCT RIGHTS ...................................................... 695 A. Different Roots ............................................................ 698 B. Different Normative Content ..................................... 701 C. Different Beneficiaries ................................................ 708 D. Different Obligations .................................................. 710 VI. CONCLUSION ...................................................................... 712 * Adjunct Faculty, Duquesne University. I would like to thank professors -

State of the Microcredit Summit Campaign Report 2004
State of the Microcredit Summit Campaign Report 2004 Written by: Sam Daley-Harris Microcredit Summit Campaign Director Compiled by: Lisa Laegreid Sherine Mahmoud Brian McConnell D.S.K. Rao With Assistance from: Nelson Agyemang Anna Awimbo Alyssa Boxhill Jess Collier David Dresner Anjum Khalidi Jonathan Kivell Mawuna Lawson Alyson Rogers TABLE OF CONTENTS Introduction………………………………………………………………………………………..3 The Faces Behind the Statistics……………………………………………………………………4 A Revolution in Banking Begets a Revolution in International Development……………………5 Removing the Most Difficult Barriers and the Most Pernicious Myths…………………………...7 A New Law and New Hope………………………………………………………………………..8 The World Bank and CGAP Respond to the Parliamentarians…………………………………..10 A Focus that Extends Far Beyond Just Reaching the Poorest……………………………………18 Survey Methodology……………………………………………………………………………...20 Clients Reached…………………………………………………………………………………..22 Growth Resulting from Institutions Reporting for the First Time and an Expanded Definition of Poorest……………………………………………………………………………………………22 Women Clients Reached………………………………………………………………………….25 The Use of Poverty Measurement Tools…………………………………………………………25 Regional Data……………………………………………………………………………………..26 Should the Microcredit Summit Campaign be Extended to 2015?……………………………….27 Determining a New Goal If the Campaign Is Extended to 2015…………………………………28 The First Measurement Challenge: Finding Cost-Effective Poverty Measurement Tools…….…28 A New Measurement Challenge: Finding Tools That Cost-Effectively Measure Movement Above -

Health Protection Innovations Demonstrated by Freedom from Hunger and Partners
MICROFINANCE AND HEALTH PROTECTION Many microfinance institutions—particularly those serving the very poor—have witnessed the significant impact that all-too-common health shocks can have on their clients’ ability to repay, save and flourish in their microenterprise endeavors. These institutions seek sustainable approaches that help safeguard their clients’ health while also protecting the institutional bottom line. Freedom from Hunger, a recognized expert in integrated financial and nonfinancial services for the poor, launched the Microfinance and Health Protection (MAHP) initiative in January 2006 with funding from the Bill & Melinda Gates Foundation. The initiative aims to develop and test integrated microfinance and health- protection products and services that positively impact clients’ lives while being practical and sustainable for microfinance institutions (MFIs). Today, integrated microfinance and health protection services are benefiting nearly 2.3 million microfinance clients in ten countries. Health Protection Innovations Demonstrated by Freedom from Hunger and Partners Freedom from Hunger initially collaborated with five MFIs in Africa, Asia and Latin America to conduct market research and to design and test an array of health-protection products and services. Each MFI developed a “package” that combined several of the following elements to meet the specific needs of their clientele in a cohesive, efficient and effective manner. Health education . Interactive education sessions on topics such as prenatal health, malaria, dengue fever, common childhood illnesses, HIV/AIDS and water and sanitation . Training on coping with health-related financial shocks, planning ahead to face common health expenses and getting the most out of local healthcare services Health financing and micro-insurance . Health loans . -

Freedom from Hunger and Recent Developments at PADME in Benin
Freedom from Hunger and recent developments at PADME in Benin Davis, California. Freedom from Hunger expresses deep concern about recent developments at Association PADME, one of its partner microfinance institutions in Benin. We believe that the governance of a private organization such as PADME should not be assumed by the government for the reasons that have been officially stated. Freedom from Hunger has been working with PADME since 2006 through our global Microfinance and Health Protection initiative, aimed at developing, testing, and documenting the impact of innovative services that combine microfinance and health protection. PADME has been instrumental in implementing high-impact innovations that are making a difference in the lives of thousands of poor families in rural Benin. At the same time, PADME has been our primary partner in carefully controlled research to examine the impact of such services on the performance of the microfinance institution itself. These activities have been successful over the past two years because of the strong commitment and aptitude of PADME’s leadership, from both the Board of Directors and management. We understand that important issues have been raised about PADME’s institutional performance and we know that René Azokli and his team have been working to address them with the assistance of PADME’s partner organizations. (We note that such questions are not unique to PADME or Benin and that sincere attention to the financial performance of such institutions is appropriate.) Freedom from Hunger is prepared to collaborate with PADME and other key stakeholders in the Beninois microfinance sector to overcome any critical pending issues in order to expedite PADME’s return to its status as an independent financial institution operating in Benin. -

Mali Poverty Outreach Study of the Kafo Jiginew and Nyèsigiso Credit and Savings with Education Programs
F REED O M F RO M HUNGER RESEARCH PAPER NO. 7 Mali Poverty Outreach Study of the Kafo Jiginew and Nyèsigiso Credit and Savings with Education Programs Anastase Nteziyaremye and Barbara MkNelly May 2001 Contents Executive Summary ....................1 Introduction................................5 1.0 Clients’ Relative Poverty by Financial Product: Basic Needs Survey..................................7 2.0 Wealth-Ranking Exercise: Relative Food Security of the Current and Ex- Members of Credit Freedom from and Savings with Hunger’s Mission Education (CEE) ..............29 3.0 Poor Women’s Founded in 1946, Freedom Perceptions: from Hunger promotes “Self- Constraints and Help for a Hungry World.” Opportunities of Joining Freedom from Hunger brings and Participating in the innovative and sustainable CEE Program ....................49 self-help solutions to the fight Résumé Analytique ...................65 against chronic hunger and Resumen Executivo ...................68 poverty. Together with local partners, we equip families Bibliography .............................71 with resources they need to Index of Tables and build futures of health, hope Figures ...............................73 and dignity. Appendices ..............................75 ©2001 Freedom from Hunger Portions of this document may be reproduced with due acknowledgment Credits of the authors and title. Design Michael Curry/ Donna Justice 1644 DAVINCI COURT DAVIS, CA 95617 (530) 758-6200 FAX (530) 758-6241 [email protected] MALI POVERTY OUTREACH STUDY OF THE KAFO JIGINEW -
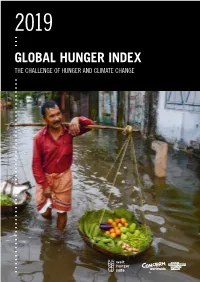
2019 Global Hunger Index: the Challenge of Hunger and Climate Change
2019 GLOBAL HUNGER INDEX THE CHALLENGE OF HUNGER AND CLIMATE CHANGE 2019 GLOBAL2019 HUNGER INDEX 2019 GLOBAL HUNGER INDEX THE CHALLENGE OF HUNGER AND CLIMATE CHANGE Klaus von Grebmer, Jill Bernstein, Fraser Patterson, Miriam Wiemers, Réiseal Ní Chéilleachair, Connell Foley, Seth Gitter, Kierstin Ekstrom, and Heidi Fritschel Guest Author Rupa Mukerji, Helvetas Dublin / Bonn October 2019 A Peer-Reviewed Publication Rupa Chaudari waters seedlings in a riverbed in Nepal. Women, who carry out a large share of agricultural labor worldwide, are often particularly vulnerable to the impacts of climate change. Their knowledge and roles in communities are key to developing adaptation strategies. CLIMATE JUSTICE: A NEW NARRATIVE FOR ACTION Mary Robinson Adjunct Professor of Climate Justice, Trinity College Dublin Former UN High Commissioner for Human Rights and Former President of Ireland t is a terrible global indictment that after decades of sustained stemming from the different social roles of women and men in many progress in reducing global hunger, climate change and conflict areas, there is a need for women’s leadership on climate justice. Iare now undermining food security in the world’s most vulnera- Climate justice is a transformative concept. It insists on a shift ble regions. from a discourse on greenhouse gases and melting icecaps into a civil With the number of hungry people rising from 785 million in rights movement with the people and communities most vulnerable to 2015 to 822 million in 2018, we can no longer afford to regard the climate impacts at its heart. It gives us a practical, grounded avenue 2030 Agenda and the Paris Climate Agreement as voluntary and a through which our outrage can be channeled into action. -
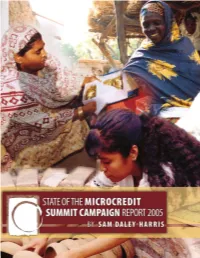
State of the Microcredit Summit Campaign Report 2005
MICROCREDIT SUmmIT CAMPAIGN HONORARY CO-CHAIRS Her Majesty, Queen Sofia of Spain Former Prime Minister of Japan, Tsutomu Hata COUNCIL CO-CHAIRS COUNCIL OF HEADS OF STATE AND GOVERNMENT * H.E. Vicente Fox, President of Mexico COUNCIL OF ADVOCATES * Chief Bisi Ogunleye, Chair, Country Women’s Association of Nigeria COUNCIL OF BANKS AND COMMERCIAL FINANCE INSTITUTIONS Eugene Ludwig, Managing General Partner, Promontory Financial, USA Andrew Krieger, CEO, Northbridge Capital Management, USA COUNCIL OF CORPORATIONS * Brett Begemann, Executive Vice President and International Commercial Lead, Monsanto, USA COUNCIL OF EDUCATIONAL INSTITUTIONS Ned Hill, Dean, Marriott School of Management, Brigham Young University James Gustave Speth, Dean, Yale University COUNCIL OF FOUNDATIONS AND PHILANTHROPISTS * George Soros, Chairman, Open Society Institute COUNCIL OF INTERNATIONAL FINANCIAL INSTITUTIONS * Lennart Båge, President, International Fund for Agricultural Development (IFAD) COUNCIL OF NON-GOVERNMENTAL ORGANIZATIONS Margaret Catley-Carlson, Chair ICARDA & Global Water Partnership Mazide Ndiaye, President and CEO, FAVDO COUNCIL OF PARLIAMENTARIANS Wakako Hironaka, Member of the House of Councillors, Japan * Sharad Pawar, Minister of Food and Agriculture, India * Michel Rocard, Chairman, Committee on Development and Cooperation, European Parliament COUNCIL OF PRACTITIONERS Nancy Barry, President, Women’s World Banking Ela Bhatt, General Secretary, Self Employed Women’s Association * Connie Evans, President, Women’s Self-Employment Program * John