Bridging the Gap: a Practitioner's Guide to Harm Reduction in Drug
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Harm Reduction Interventions in Substance Abuse Treatment
Prepared by: Karissa Hughes April 2018 Harm Reduction Interventions in Substance Abuse Treatment 1 Philosophy/Overview ● Harm reduction is a client-centered philosophy that engages clients in the process of behavior change even if they are not motivated to pursue abstinence from substance 2 use or refrain from engaging in other risk-taking behaviors as a treatment goal. ● Harm reduction challenges the traditional notion of abstinence as a universal treatment goal for problem substance use. It focuses on reducing the harm of drug use to the user and society (health, social, and economic consequences) for people unable or unwilling to stop using drugs rather than requiring abstinence as a condition of treatment. o Harm reduction strategies are community-based, user-driven, non-judgmental and address systems that isolate and marginalize individuals. o Harm reduction acknowledges that clients often seek out substance abuse treatment services to address risky injection practices and sexual risk-taking behavior, even when they are not interested in changing substance use patterns. ● Many people who use drugs prefer to use informal and non-clinical methods to reduce their drug consumption or reduce the risks associated with their drug use. Thus, harm reduction is a public health philosophy and service delivery model to reduce the risks of drug use while respecting the dignity and autonomy of individuals. o Harm reduction policies and practices emphasize the human right for the highest attainable standard for health of people who use drugs. o The approach is based on the belief that it is in both the user's and society's best interest to minimize the adverse consequences of drug use when the person is unable or unwilling to discontinue using. -

2017 Global Drug Survey
Prepared by the GDS Core Research Team Dr Adam Winstock, Dr Monica Barratt, Dr Jason Ferris & Dr Larissa Maier Global overview and highlights N > 115,000 Global Drug Survey GDS2017 © Not to be reproduced without authors permission Hi everyone On behalf of the GDS Core Research Team and everyone of our amazing international network partners and supportive media organisations we’d like to share our headline report deck. I know it won’t have everything that everyone wants but we are hopeful it will give people an idea of how the world of drugs is changing and highlight some of the key things that we think people can better engage with to keep themselves and those they care for safe. Once we cleaned the data from 150,000 people we chose to use data from just under 120,000 people this year for these reports. We have data reports addressing 18 different areas for over 25 countries. We can only share a fraction of what we have here on the site. However, we are very open to sharing the other findings we have and would ask researchers and public health groups to contact us so we can discuss funding and collaboration. We have almost completed designing GDS2018 so that we can start piloting early and give countries where we have not yet found friends to reach out to us. We particularly want to hear from people in Japan, Eastern Europe, Africa and the Middle East. Dr Adam R Winstock Founder and CEO Global Drug Survey Consultant Psychiatrist and Addiction Medicine Specialist Global Drug Survey GDS2017 © Not to be reproduced without authors permission We think this will be interesting. -

Talking Tobacco Harm Reduction
TALKING TOBACCO HARM REDUCTION // WHAT’S HARM REDUCTION? Harm reduction is a range of Do they make sunbathing or pragmatic policies, regulations driving 100% risk-free? and actions. Reducing health risks by providing less harmful forms No – but they do make them of products or substances, less harmful by reducing the or by encouraging less risky risk of illness or injury. behaviours. Sun cream and seat belts are We believe non-combustible nicotine Next Generation Products everyday examples of harm (NGPs) are also an effective form of reduction in action. harm reduction for adult smokers who wish to continue using nicotine – relative to conventional cigarettes. // INTRODUCING TOBACCO HARM REDUCTION Science demonstrates smoking a For adult smokers, the greatest risk of cigarette is the most harmful way to disease stems from burning tobacco and consume nicotine. inhaling the smoke. // WHAT IS THR? Tobacco smoke contains over 7000 The undisputed best action adult chemicals – nicotine is one of them. smokers can take to improve their Around 100 are classified by public health is to stop all tobacco and health experts as causes or potential nicotine use entirely, but many are not causes of smoking-related disease. interested or willing to take this step. Numerous public health bodies1 While the science suggests nicotine is believe transitioning to nicotine addictive and not risk-free, it’s neither products that are substantially less carcinogenic nor the primary cause of harmful than inhaled tobacco smoke smoking-related diseases. is their next best option – we agree. Contains 7000+ Contains chemicals, 100 significantly of them harmful fewer and lower or potentially levels of harmful harmful. -

Harm Reduction and Currently Illegal Drugs Implications for Nursing Policy, Practice, Education and Research
Harm Reduction and Currently Illegal Drugs Implications for Nursing Policy, Practice, Education and Research Discussion Paper This paper has been prepared by the Canadian Nurses Association (CNA) to stimulate dialogue on a particular topic or topics. The views and opinions expressed in this paper do not necessarily reflect the views of the CNA board of directors. CNA is the national professional voice of registered nurses in Canada. A federation of 11 provincial and territorial nursing associations and colleges representing 143,843 registered nurses, CNA advances the practice and profession of nursing to improve health outcomes and strengthen Canada’s publicly funded, not-for-profit health system. All rights reserved. No part of this document may be reproduced, stored in a retrieval system, or transcribed, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without written permission of the publisher. © Canadian Nurses Association 50 Driveway Ottawa, ON K2P 1E2 Tel.: 613-237-2133 or 1-800-361-8404 Fax: 613-237-3520 Website: www.cna-aiic.ca ISBN 978-1-55119-349-6 March 2011 TABLE OF CONTENTS Executive Summary ................................................................................................................. 3 Introduction ............................................................................................................................. 5 I. Illegal Drug Use in Canada .................................................................................................. 7 Health -

Evaluation of a Drug Checking Service at a Large Scale Electronic Music Festival in Portugal
International Journal of Drug Policy 73 (2019) 88–95 Contents lists available at ScienceDirect International Journal of Drug Policy journal homepage: www.elsevier.com/locate/drugpo Research Paper Evaluation of a drug checking service at a large scale electronic music festival in Portugal T ⁎ Helena Valentea,b,c, , Daniel Martinsb,d, Helena Carvalhoe,f, Cristiana Vale Piresb,g,h, Maria Carmo Carvalhob,h, Marta Pintoa,c,i, Monica J. Barrattj,k a Faculty of Psychology and Educational Sciences of the Porto University, Portugal b Kosmicare Association, Portugal c CINTESIS. Centre for Health Technology and Services Research, Portugal d CIQUP. Department of Chemistry and Biochemistry, Faculty of Sciences of the Porto Univsersity of Porto, Portugal e CPUP. Centre for Psychology of the University of Porto, Portugal f inED. Centre for Research and Innovation in Education, Portugal g Faculty of Education and Psychology of the Portuguese Catholic University, Portugal h CRIA. Centre for Research in Anthropology, Portugal i Faculty of Medicine of the Porto University, Portugal j Social and Global Studies Centre, RMIT University, Australia k National Drug and Alcohol Research Centre, Australia ARTICLE INFO ABSTRACT Keywords: Background: Drug checking services are being implemented in recreational settings across the world, however Harm reduction these projects are frequently accused of a lack of evidence concerning their impact on people who use drugs. This Program evaluation paper describes the implementation of a drug checking service at the Boom Festival 2016 and explores the Drug checking impact of this service on its users’ behavioural intentions. Boom festival Methods: 753 drug samples were submitted to the drug checking service for chemical analysis. -

2.3 Harm Reduction – What Is It and Why Is It Useful?
SENSIBLE CANNABIS EDUCATION A Toolkit for Educating Youth 2.3 HARM REDUCTION – WHAT IS IT AND WHY IS IT USEFUL? By the end of this section, you will: 1. Understand what harm reduction is 2. Understand practical ways to reduce the harms associated with cannabis use, through both abstinence and the reduction of risky behaviours for youth who are already using cannabis WHAT IS HARM REDUCTION? “Taking a pragmatic approach to this generally understood phenomenon, harm reduction avoids taking a uniform stance that substance use is bad, but instead focuses on getting accurate and unbiased information on the harm of use to potential users, in order to help them make informed decisions about whether to use, and if they choose to use, what precautions to take to minimize their risk.”277 Harm reduction is a philosophy that underpins public health approaches to drugs and drug use, and attempts to reduce the harms of drug use without necessarily reducing drug use itself. Harm reduction acknowledges that there are inherent risks involved with a range of behaviours and that there are ways to reduce those risks. Harm reduction can also be understood in the context of a range of activities other than drug use, as simple as wearing sunscreen or wearing a helmet. REDUCING CANNABIS-RELATED HARMS In order to ensure cannabis education is suitable for all young people, discussing strategies to reduce the harms of cannabis use is of critical importance to supporting responsible and safe use among those youth who may choose to use cannabis. In 2017, the Canadian Research Initiative in Substance Misuse (CRISM) released an evidence- based guide on how to improve health and minimize risk for Canadians who use cannabis.278 The following discussion relies on CRISM’s “Lower-Risk Cannabis Use Guidelines” (LRCUG), however, it is tailored to youth based on feedback from our content committee and contributors. -

Year End Report 2019 Year End Report 2019
Vancouver Island Drug Checking Project Year End Report 2019 Year End Report 2019 The Vancouver Island Drug Checking Project delivers drug checking services in Victoria, BC. We currently operate at SOLID Outreach, AVI Health and Community Services, and Lantern Services as well as festivals and community events. This free and confidential service provides information on composition of substances and harm reduction infor- mation. We employ five instruments as follows: Fentanyl Strip Tests Fourier Transformed Infrared Spectroscopy (FTIR) Raman Spectroscopy 935 Surface Enhanced Raman Spectroscopy (SERS) Samples Tested Gas Chromatography – Mass Spectrometry (GC-MS) in 2019 What were people bringing to be tested? We asked people what drug they were bringing to be tested. The majority of substances were expected to be heroin or fentanyl (362), a stimulant (234), or a psychedelic (139). Further, many brought unknown samples for testing (73) or did not provide information (56). This may be due in part to people testing for others and bringing multiple samples or hav- ing found substances. The remaining substances were expected to be dissociatives (31), benzodiazepines (16) or other depressants (5), other opioids (5), polysubstance (3) or other (11). Opioid-Down: heroin and/or Stimulant: methampheta- Psychedelic: LSD, MDMA, 362362 fentanyl 234234 mine, cocaine HCl, cocaine base 139139 MDA, 2CB, DMT Unknown Missing Dissociative: ketamine, DXM, 7373 5656 3131 methoxetamine, PCP Depressant- Other Depressant-Other: GHB, 1616 Benzodiazepines 1111 5 GBL, barbiturates, methaqualone, phenibut Opioid-Other: morphine, phar- Polysubstance 55 maceutical opioids 33 Data are not finalized and subject to change. There were missing data for some samples. Vancouver Island Drug Checking Project Year End Report 2019 How many samples tested positive for fentanyl? We tested all samples using Fentanyl Test Strips to determine whether they contained fentanyl. -

Reducing Cannabis Harms: a Guide for Ontario Campuses
Reducing cannabis harms: A guide for Ontario campuses About This Guide This guide explores issues related to cannabis use and provides readers with an overview of health approaches that can reduce the harms and risks associated with it. Any campus professional — whether faculty, academic advisor, counsellor, or student services professional — working with students who use cannabis will be able to refer to the guide for information. The first section will give you a better understanding of cannabis, the Ontario context, the substance use spectrum, as well as substance use disorders and problematic substance use. Section 2 looks at the reasons why students use or don’t use cannabis, the effects of cannabis use on the brain in adolescents and young adults, the link between cannabis use and mental health, the effects of language and stigma, and strategies that campus professionals can use to reduce harms when directly engaging with students. The final section provides concrete steps for developing a campus-wide cannabis-use framework to reduce harm. While the focus of this guide is on cannabis use by students, not campus staff or faculty, this is in no way meant to minimize the need to address the broader scope of mental health, substance use, and well- being on campuses, including among faculty and staff. Each post-secondary institution has unique strengths, circumstances, and needs. For this reason, while the broad areas addressed in this guide are relevant to all institutions, it is not meant to be prescriptive or to serve as legal advice pertaining to cannabis use legislation. As of its writing, the information in this guide is accurate and reflects current research and legislation. -

Harm Reduction / Drug Policy Reform Notes
Questions and answers on the issue of a regulated market for currently illegal drugs Mark Haden Vancouver Coastal Health Draft: February 2012 For the past decade I have been involved with public presentations which explore the failures of drug prohibition. In these presentations I recommend a public health, human rights model of drug control which brings all currently illegal drugs into a regulatory framework. The following is a list of the most common challenges I experience: Q1: Are you saying that you want to legalize all drugs? A: No: Legalization is often interpreted to mean that the current capitalist free market system would be used to advertise and distribute currently illegal drugs. The goal of the free market is to increase consumption. The concept of a regulated market is instead guided by Public Health which has the goal to reduce the health and social problems associated with drugs. Q2: What do you mean by a regulated market for illegal drugs? A: A regulated market would actively control drugs based on the principles of public health and human rights. Prohibition paradoxically stimulates a illegal market that makes concentrated and sometimes toxic, drugs widely available. The goal is to greatly reduce or shut down the illegal market and regulate drugs in a way that reduces harm to individuals, families and our society as a whole. Seeing drug use as primarily a health and social issue rather than a criminal issue allows us to explore a wide range of tools to manage the problems associated with drugs in a more effective way. Q3: Are you saying “yes” to drugs? A: No – but we are saying “yes” to using more effective ways of controlling drugs and their problems. -
Treatment, Prevention and Harm Reduction Interventions for Different Forms of ATS Use
Correlation European Harm Reduction C Network Briefing Paper Treatment, prevention and harm reduction interventions for different forms of ATS use Correlation European Harm Reduction C Network 1 Correlation European Harm Reduction C Network Colophon This C-EHRN Briefing Paper was developed by Rafalea Rigoni, Nienke Liebregts and Katrin Schiffer and is based on the results and findings of the ATTUNE study and other relevant literature. More info via: wwww.correlation-net.org https://www.correlation-net.org/attune/ Authors: Rafaela Rigoni Nienke Liebregts Katrin Schiffer Review: Graham Shaw Copyright ©2021 Coyright remains with the publisher. Publisher: De Regenboog Groep/ Correlation-European Harm Reduction Network Stadhouderskade 159 1074BC Amsterdam Netherlands Correlation European Harm Reduction C Network Correlation-European Harm Reduction Network is co-funded by the European Commission This project has been made possible by 2 Correlation European Harm Reduction C Network List of Acronyms 4-FA 4-Fluoroamphetamine (C9H12FN), also known as para-fluoroamphetamine (PFA) 4-MA 4-Methylamphetamine (C10H15N) ADHD Attention Deficit Hyperactivity Disorder ATS Amphetamine Type Stimulants ATTUNE study Understanding Pathways to Stimulant Use: a mixed-methods ex- amination of the individual, social and cultural factors shaping illicit stimulant use across Europe CDU Currently Dependent User CNU Non-dependent Current frequent User EMCDDA The European Monitoring Centre for Drugs and Drug Addiction EU European Union FDU Formerly Dependent User FFU -

Regulation of Drug Checking Services
IN CONFIDENCE In Confidence Office of the Minister of Health Cabinet Social Wellbeing Committee Regulation of drug checking services Proposal 1 This paper seeks agreement to amend the Misuse of Drugs Act 1975 and the Psychoactive Substances Act 2013 to enable a permanent system of regulation for drug checking service providers. Relation to government priorities 2 This proposal does not relate to a Government priority. Executive Summary 3 Drug checking services check the composition of illicit drugs and provide harm reduction advice to help individuals make informed decisions about drug use. Where a drug is not as presumed, the individual can make the potentially life-saving decision not to consume it. 4 Drug checking is currently regulated under amendmentsreleased made by the Drug and Substance Checking Legislation Act 2020 (the Drug Checking Act) to the Misuse of Drugs Act and the Psychoactive Substances Act. These amendments allow appointed drug checking service providers to operate with legal certainty. 5 The Drug Checking Act was always intended to be temporary legislation to allow time for a permanent licensing system to be developed. The Drug Checking Act includes mechanisms which will repeal the amendments to the Misuse of Drugs Act and the Psychoactive Substances Act in December 2021. 6 If a permanent system is not in place when the Drug Checking Act repeal provisions take effect, drug checking will revert to a legal grey area. This would impede service provision and make it more difficult to prevent harm from dangerous substances such as synthetic cathinones (sometimes known as “bath salts”). Regulation is required to enable good quality services and to prevent low-quality service providers from operating. -
Drug Checking Static Pilot Results
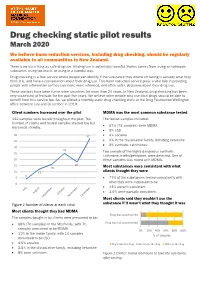
Drug checking static pilot results March 2020 We believe harm reduction services, including drug checking, should be regularly available to all communities in New Zealand. There is no such thing as safe drug use. All drug use is potentially harmful. Harms comes from using an unknown substance, using too much, or using in a harmful way. Drug checking is a free service where people can identify if the substance they intend on taking is actually what they think it is, and have a conversation about their drug use. This harm reduction service plays a vital role in providing people with information so they can make more informed, and often safer, decisions about their drug use. These services have been run in other countries for more than 20 years. In New Zealand, drug checking has been very successful at festivals for the past five years. We believe other people who use illicit drugs should be able to benefit from this service too. So, we piloted a monthly static drug checking clinic at the Drug Foundation Wellington office between July and December in 2019. Client numbers increased over the pilot MDMA was the most common substance tested 112 samples were tested throughout the pilot. The The tested samples included: number of clients and tested samples started low but 67% (75 samples) were MDMA increased steadily. • • 9% LSD 40 37 • 4% cocaine 35 • 4% in the dissociative family, including ketamine • 3% synthetic cathinones. 30 25 Two sample of the highly dangerous synthetic 25 cathinone, n-ethylpentylone, were detected. One of 20 these samples was mixed with MDMA.