IND-Enabling Studies for a Clinical Trial to Genetically Program a Persistent Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supplemental Figures
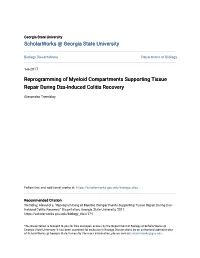
A Spleen Liver MLN B 750 Spleen MLN Liver/Tumor s cell 6 500 Control CFU-GM 10 BFU-E per CFU-GEMM 250 U-C CF 0 l l r er ro pa ro pa v ve or nt nt li li He He l tum Co Co ro pa pa nt He He Hepa Co ) C 3 D 2 5 * E 4 10 *** 10 ) * ** 4 Control CFU-GM (g 2 C( 8 e BFU-E 2 * 2 3 Hepa-2wk * Hepa-3wk 6 CFU-GEMM eight 2 CFU- hang 2 c Hepa-4wk ic * rw 1 4 1 ld 2 en Fo 2 0 pl 2 ls Tumo 0 2 -1 0 LSKLK Tota l wk wk wk ro wk wk wk 2 3 4 nt 2 3 4 pa pa pa Co pa pa pa He He He He He He ) 7 *** *** F 0.6 8 5 G 2 ) *** 6 *** 10 Control 2 Control (g 4 5 e 0.5 y( Hepa 2 Hepa it 4 ght i *** 2 ar 3 3LL 3LL 3 0.4 hang ul we 2 ll B16-F10 c B16-F10 0.2 2 2 ld 2 ce TRAMP TRAMP 2 1 Min/+ Fo Min/+ 0.1 1 Apc 0 Apc Spleen 2 -1 0.0 Spleen 0 2 LSKLK H I before sorting Fresh 12 hr Day 1 Day 2 Day 4 Day 6 Day 8 gated in CD45+lin- gated in CD45+lin- LK:31.0 LSK:3.7 GMP: 35.6 LK:1.7 LSK:98.3 LK:15.9 LSK:84.1 LK:34.4 LSK:65.6 LK:67.8 LSK:32.2 LK:90.1 LSK:9.9 LK:93.5 LSK:6.5 LK:97.0 LSK:3.0 BM c-Kit Sca-1 GMP: 3.2 GMP: 12.5 GMP: 77.8 GMP: 5.6 GMP: 43.4 GMP: 62.6 LK:14.7 LSK:1.6 GMP: 17.1 BM LSK CMP: 12.6 CMP: 28.8 CMP: 54.1 CMP: 18.1 CMP: 39.6 CMP: 30.0 CD34 Spleen CD16/CD32 c-Kit CD34 Sca-1 CD16/CD32 gated in CD45+lin- after sorting LK:1.2 LSK:98.8 LK:21.8 LSK:78.2 LK:33.6 LSK:66.4 LK:62.1 LSK:37.9 LK:89.3 LSK:10.7 LK:90.2 LSK:9.8 LK:96.3 LSK:3.7 LSK: 98.3 c-Kit BM GMP: 98.6 Sca-1 GMP: 3.1 GMP: 14.8 GMP: 67.5 GMP: 7.2 GMP: 27.7 GMP: 49.8 Splenic LSK CMP: 18.3 CMP: 25.7 CMP: 46.7 CMP: 28.0 CMP: 28.0 CMP: 39.4 CD34 LSK: 97.5 CD16/CD32 GMP: 94.9 Spleen c-Kit CD34 Sca-1 CD16/CD32 Supplemental Figure 1. -

Hematopoietic Reconstitution After Lethal Irradiation and Bone
Bone Marrow Transplantation (2000) 25, 427–433 2000 Macmillan Publishers Ltd All rights reserved 0268–3369/00 $15.00 www.nature.com/bmt Hematopoietic reconstitution after lethal irradiation and bone marrow transplantation: effects of different hematopoietic cytokines on the recovery of thymus, spleen and blood cells D Frasca1, F Guidi1, M Arbitrio1, C Pioli1, F Poccia2, R Cicconi2 and G Doria2 1Laboratory of Immunology, AMB-PRO-TOSS, ENEA CR Casaccia, Rome; and 2Department of Biology, University of Rome ‘Tor Vergata’, Rome, Italy Summary: ative treatments of the recipient has been used to reconsti- tute hematopoiesis. The HPC capable of long-term reconsti- Lethally irradiated mice were grafted with syngeneic tution are quiescent and slowly cycling bone marrow cells bone marrow cells or left ungrafted. Mice of each group that form multiple colonies of mixed lineages only in the were injected with different hematopoietic cytokines presence of bone marrow stromal cell-derived cytokines.6 for 5 consecutive days starting immediately after Thus, the use of hematopoietic cytokines together with irradiation or left uninjected. The recovery of lymphoid bone marrow transplantation has been shown to hasten neu- tissues induced by hematopoietic cytokines 7 days after trophil and platelet recovery, suggesting that appropriate irradiation and bone marrow cell transplantation was combinations of these factors may be used to promote full comparable to that observed at days 21–28 in reconstitution of the hematopoietic compartment.7–9 irradiated, bone marrow-grafted, but cytokine-unin- In the present work, we have compared the effects of jected mice. IL-11 or IL-6, in combination with IL-3, hematopoietic cytokines, such as IL-3, IL-11, SCF, IL-6 was able to hasten thymus, spleen and blood cell num- and the IL-6 super-agonist K-7/D-6, on the repopulation of bers and functions. -

Cd47-Sirpα Interaction and IL-10 Constrain Inflammation-Induced Macrophage Phagocytosis of Healthy Self-Cells
Cd47-Sirpα interaction and IL-10 constrain inflammation-induced macrophage phagocytosis of healthy self-cells Zhen Biana,b, Lei Shia, Ya-Lan Guoa, Zhiyuan Lva, Cong Tanga, Shuo Niua, Alexandra Tremblaya, Mahathi Venkataramania, Courtney Culpeppera, Limin Lib, Zhen Zhoub, Ahmed Mansoura, Yongliang Zhangc, Andrew Gewirtzd, Koby Kiddera,e, Ke Zenb, and Yuan Liua,d,1 aProgram of Immunology and Cell Biology, Department of Biology, Center for Diagnostics & Therapeutics, Georgia State University, Atlanta, GA 30302; bState Key Laboratory of Pharmaceutical Biotechnology, Nanjing Advanced Institute for Life Sciences, Nanjing University, Nanjing, Jiangsu 210093, China; cDepartment of Microbiology and Immunology, Yong Loo Lin School of Medicine, Life Science Institute (LSI) Immunology Programme, National University of Singapore, Singapore 117456; dCenter for Inflammation, Immunity and Infection, Georgia State University, Atlanta, GA 30303; and eDepartment of Cell Biology, Rutgers University, New Brunswick, NJ 08901 Edited by Jason G. Cyster, University of California, San Francisco, CA, and approved July 11, 2016 (received for review October 28, 2015) − − Rapid clearance of adoptively transferred Cd47-null (Cd47 / ) cells in The CD47-SIRPα mechanism was first reported by Oldenborg congeneic WT mice suggests a critical self-recognition mechanism, et al. (1), who had demonstrated in red blood cell (RBC) in which CD47 is the ubiquitous marker of self, and its interaction transfusion experiments that WT mice rapidly eliminate syngeneic − with macrophage signal regulatory protein α (SIRPα) triggers inhib- Cd47-null (Cd47 ) RBCs through erythrophagocytosis in the itory signaling through SIRPα cytoplasmic immunoreceptor tyrosine- spleen and that the lack of tyrosine phosphorylation in SIRPα based inhibition motifs and tyrosine phosphatase SHP-1/2. -

Deficiency of Transcription Factor Relb Perturbs Myeloid and DC Development by Hematopoietic- Extrinsic Mechanisms
Deficiency of transcription factor RelB perturbs myeloid and DC development by hematopoietic- extrinsic mechanisms Carlos G. Briseñoa, Marco Gargaroa, Vivek Duraia, Jesse T. Davidsona, Derek J. Theisena, David A. Anderson IIIa, Deborah V. Novacka,b, Theresa L. Murphya, and Kenneth M. Murphya,c,1 aDepartment of Pathology and Immunology, School of Medicine, Washington University in St. Louis, St. Louis, MO 63110; bMusculoskeletal Research Center, Division of Bone and Mineral Diseases, Department of Medicine, Washington University School of Medicine, St. Louis, MO 63110; and cHoward Hughes Medical Institute, School of Medicine, Washington University in St. Louis, St. Louis, MO 63110 Contributed by Kenneth M. Murphy, February 21, 2017 (sent for review December 2, 2016; reviewed by Jason G. Cyster and Federica Sallusto) RelB is an NF-κB family transcription factor activated in the noncanon- do show a cell-intrinsic impairment in proliferation in vitro in re- ical pathway downstream of NF-κB–inducing kinase (NIK) and TNF sponse to CD40 stimulation, but secretion of IgM is normal and receptor family members including lymphotoxin-β receptor (LTβR) in vitro switching to all non-IgM non-IgD isotypes is intact (10). and CD40. Early analysis suggested that RelB is required for classical These results imply that the observed in vivo requirement for RelB dendritic cell (cDC) development based on a severe reduction of cDCs in class switching is B-cell–extrinsic. − − in Relb / mice associated with profound myeloid expansion and The actions of RelB in DC development and function, also re- perturbations in B and T cells. Subsequent analysis of radiation chimeras main incompletely defined. -

Innate IFN-Γ Ameliorates Experimental Autoimmune Encephalomyelitis
www.nature.com/scientificreports OPEN Innate IFN-γ ameliorates experimental autoimmune encephalomyelitis and promotes Received: 29 August 2017 Accepted: 13 December 2017 myeloid expansion and PDL-1 Published: xx xx xxxx expression Madeleine P. J. White1, Gill Webster2, Faith Leonard1,2 & Anne Camille La Flamme 1,3 The innate immune system plays a central role in the immune-mediated pathology of multiple sclerosis, and is a therapeutic target for progressive disease. Recently, it has been demonstrated that MIS416, a novel immunomodulatory microparticle that activates NOD-2 and TLR-9-signaling, has disease- modifying activity in multiple sclerosis models. This activity is dependent on innate IFN-γ; however, the precise immune regulatory mechanisms amplifed by MIS416 have not previously been determined. Using the experimental autoimmune encephalomyelitis model, MIS416 treatment was associated with IFN-γ–dependant expansion of Treg number and increased suppressive function; however, these cells did not account for disease reduction. Additionally, MIS416 treatment stimulated increased nitric oxide production that was IFN-γ–dependant but dispensable for protection. Finally, MIS416-mediated protection was shown to correlate with IFN-γ–dependant expansion of PDL-1-expressing peripheral myeloid cells, a subset of which was found to be selectively recruited to the brain. This central nervous system trafcking was independent of neuro-infammatory signals as it occurred in MIS416-treated healthy mice. Together, these fndings provide insight into regulatory myeloid cell activities amplifed by MIS416-mediated NOD-2 and TLR-9 signalling and highlight the potential importance of these cells in accessing the brain where they may act locally and contribute to the control of neuroinfammation. -

P38α Controls Erythroblast Enucleation and Rb Signaling in Stress Erythropoiesis
Cell Research (2012) 22:539-550. © 2012 IBCB, SIBS, CAS All rights reserved 1001-0602/12 $ 32.00 npg ORIGINAL ARTICLE www.nature.com/cr p38α controls erythroblast enucleation and Rb signaling in stress erythropoiesis Simon M Schultze1, Andreas Mairhofer1, Dan Li2, Jin Cen2, Hartmut Beug1, 4, Erwin F Wagner3, Lijian Hui2 1Research Institute of Molecular Pathology (IMP), Dr. Bohr-Gasse 7, A-1030, Vienna, Austria; 2Laboratory of Molecular Cell Biol- ogy, Institute of Biochemistry and Cell Biology, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences, Yueyang Road 320, Shanghai 200031, China; 3F-BBVA-CNIO Cancer Cell Biology Programme, Spanish National Cancer Research Centre, Melchor Fernández Almagro 3, E-28029, Madrid, Spain Enucleation of erythroblasts during terminal differentiation is unique to mammals. Although erythroid enuclea- tion has been extensively studied, only a few genes, including retinoblastoma protein (Rb), have been identified to regulate nuclear extrusion. It remains largely undefined by which signaling molecules, the extrinsic stimuli, such as erythropoietin (Epo), are transduced to induce enucleation. Here, we show that p38α, a mitogen-activated protein ki- nase (MAPK), is required for erythroid enucleation. In an ex vivo differentiation system that contains high Epo levels and mimics stress erythropoiesis, p38α is activated during erythroid differentiation. Loss of p38α completely blocks enucleation of primary erythroblasts. Moreover, p38α regulates erythroblast enucleation in a cell-autonomous man- ner in vivo during fetal and anemic stress erythropoiesis. Markedly, loss of p38α leads to downregulation of p21, and decreased activation of the p21 target Rb, both of which are important regulators of erythroblast enucleation. This study demonstrates that p38α is a key signaling molecule for erythroblast enucleation during stress erythropoiesis. -
Reprogramming of Myeloid Compartments Supporting Tissue Repair During Dss-Induced Colitis Recovery
Georgia State University ScholarWorks @ Georgia State University Biology Dissertations Department of Biology 1-6-2017 Reprogramming of Myeloid Compartments Supporting Tissue Repair During Dss-Induced Colitis Recovery Alexandra Tremblay Follow this and additional works at: https://scholarworks.gsu.edu/biology_diss Recommended Citation Tremblay, Alexandra, "Reprogramming of Myeloid Compartments Supporting Tissue Repair During Dss- Induced Colitis Recovery." Dissertation, Georgia State University, 2017. https://scholarworks.gsu.edu/biology_diss/174 This Dissertation is brought to you for free and open access by the Department of Biology at ScholarWorks @ Georgia State University. It has been accepted for inclusion in Biology Dissertations by an authorized administrator of ScholarWorks @ Georgia State University. For more information, please contact [email protected]. REPROGRAMMING OF MYELOID COMPARTMENTS SUPPORTING TISSUE REPAIR DURING DSS-INDUCED COLITIS RECOVERY by ALEXANDRA V. TREMBLAY Under the Direction of Yuan Liu MD, PhD ABSTRACT Myeloid-derived suppressor cells (MDSC), emerging during tumor growth or chronic inflammation play a critical role in regulating T cell function. However, mechanisms governing the generation of these cells remain unclear, and need to be further defined. Using a DSS- induced colitis and recovery model, we characterized the dynamic changes within myeloid compartments and the emergence of MDSC during active and resolution phases of inflammation. We show that the immature myeloid compartment expands in bone marrow (BM) specifically at the resolution phase of inflammation during colitis transition to recovery. Additionally, we found enhanced levels of IL-17 in the serum of colitis mice tightly correlates with expansion of the IMC compartment, and is likely the factor responsible for expansion of these cells. -

Original Article
Chinese Medical Journal 2014;127 (3) 475 Original article Allogeneic compact bone-derived mesenchymal stem cell transplantation increases survival of mice exposed to lethal total body irradiation: a potential immunological mechanism Qiao Shukai, Ren Hanyun, Shi Yongjin and Liu Wei Keywords: mesenchymal stem cells; transplantation; total body irradiation; colony-forming unit granulocyte/macrophage; immunological mechanism Background Radiation-induced injury after accidental or therapeutic total body exposure to ionizing radiation has serious pathophysiological consequences, and currently no effective therapy exists. This study was designed to investigate whether transplantation of allogeneic murine compact bone derived-mesenchymal stem cells (CB-MSCs) could improve the survival of mice exposed to lethal dosage total body irradiation (TBI), and to explore the potential immunoprotective role of MSCs. Methods BALB/c mice were treated with 8 Gy TBI, and then some were administered CB-MSCs isolated from C57BL/6 mice. Survival rates and body weight were analyzed for 14 days post-irradiation. At three days post-irradiation, we evaluated IFN-γ and IL-4 concentrations; CD4+CD25+Foxp3+ regulatory T cell (Treg) percentage; CXCR3, CCR5, and CCR7 expressions on CD3+ T cells; and splenocyte T-bet and GATA-3 mRNA levels. CB-MSC effects on bone marrow hemopoiesis were assessed via colony-forming unit granulocyte/macrophage (CFU-GM) assay. Results After lethal TBI, compared to non-transplanted mice, CB-MSC-transplanted mice exhibited significantly increased survival, body weight, and CFU-GM counts of bone marrow cells (P<0.05), as well as higher Treg percentages, reduced IFN-γ, CXCR3 and CCR5 down-regulation, and CCR7 up-regulation. -

Method for in Vivo Evaluation of Cytokines of an Alternate, Novel
IL-17 Stimulates Granulopoiesis in Mice: Use of an Alternate, Novel Gene Therapy-Derived Method for In Vivo Evaluation of Cytokines This information is current as Paul Schwarzenberger, Vincent La Russa, Allan Miller, Peng of September 28, 2021. Ye, Weitao Huang, Arthur Zieske, Steve Nelson, Gregory J. Bagby, David Stoltz, Randall L. Mynatt, Melanie Spriggs and Jay K. Kolls J Immunol 1998; 161:6383-6389; ; http://www.jimmunol.org/content/161/11/6383 Downloaded from References This article cites 20 articles, 11 of which you can access for free at: http://www.jimmunol.org/content/161/11/6383.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 28, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 1998 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. IL-17 Stimulates Granulopoiesis in Mice: Use of an Alternate, Novel Gene Therapy-Derived Method for In Vivo Evaluation of Cytokines1 Paul Schwarzenberger,2*† Vincent La Russa,| Allan Miller,| Peng Ye,*† Weitao Huang,*† Arthur Zieske,§ Steve Nelson,*† Gregory J. -

T Cells with Dendritic Cell Properties
ARTICLE Received 20 Aug 2012 | Accepted 22 Oct 2012 | Published 27 Nov 2012 DOI: 10.1038/ncomms2223 Identification and characterization of polyclonal ab-T cells with dendritic cell properties Mirela Kuka1, Ivana Munitic1 & Jonathan D. Ashwell1 An efficient immune response requires coordination between innate and adaptive immunity, which act through cells different in origin and function. Here we report the identification of thymus-derived ab-T-cell receptor þ cells that express CD11c and major histocompatibility complex class II, and require FLT3 ligand for development (TDC). TDC express genes here- tofore found uniquely in T cells or dendritic cells, as well as a distinctive signature of cyto- toxicity-related genes. Unlike other innate T-cell subsets, TDC have a polyclonal T-cell receptor repertoire and respond to cognate antigens. However, they differ from conventional T cells in that they do not require help from antigen-presenting cells, respond to Toll-like receptor-mediated stimulation by producing interleukin-12 and process and present antigen. The physiological relevance of TDC, found in mice and humans, is still under investigation, but the fact that they combine key features of T and dendritic cells suggests that they provide a bridge between the innate and adaptive immune systems. 1 Laboratory of Immune Cell Biology, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892, USA. Correspondence and requests for materials should be addressed to J.D.A. (email: [email protected]). NATURE COMMUNICATIONS | 3:1223 | DOI: 10.1038/ncomms2223 | www.nature.com/naturecommunications 1 & 2012 Macmillan Publishers Limited. All rights reserved. -

Analysis of Spleen Histopathology, Splenocyte Composition And
bioRxiv preprint doi: https://doi.org/10.1101/2021.01.22.427878; this version posted January 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Analysis of Spleen Histopathology, Splenocyte 2 composition and Hematological Parameters in Mice 3 Infected with Plasmodium berghei K173 4 5 Huajing Wang a,b,Shuo Li a,b, Zhao Cui a, Tingting Qin a,b, Hang Shi a, Ji Ma a,b, 6 Lanfang Li a, Guihua Yu, Tingliang Jiang a,b and Canghai Li a* 7 8 a Tang Center for Herbal Medicine Research, China Academy of Traditional Chinese 9 Medical Sciences, Beijing, China 10 b Artemisinin Research Center and Institute of Chinese Meteria Medica, China 11 Academy of Traditional Chinese Medical Sciences, Beijing, China 12 * Correspondence to: Dr. Canghai Li, Tang Center for Herbal Medicine Research, 13 Institute of Chinese Materia Medica, China Academy of Chinese Medical Sciences, 14 No. 16 Dongzhimen Nanxiaojie, Dongcheng District, Beijing 100700, China. Tel: 15 (+86) 10-6404-1008, Fax: (+86) 10-6404-1008, E-mail: [email protected] 16 17 ABSTRACT Malaria is a fatal disease that presents clinically as a continuum of 18 symptoms and severity, which are determined by complex host-parasite interactions. 19 Clearance of infection is believed to be accomplished by the spleen and mononuclear 20 phagocytic system (MPS), both in the presence and absence of artemisinin treatment. -

Enhanced Transduction of Mouse Bone Marrow
Gene Therapy (2006) 13, 29–39 & 2006 Nature Publishing Group All rights reserved 0969-7128/06 $30.00 www.nature.com/gt ORIGINAL ARTICLE Enhanced transduction of mouse bone marrow- derived dendritic cells by repetitive infection with self- complementary adeno-associated virus 6 combined with immunostimulatory ligands WA Aldrich1,2, C Ren3, AF White3, S-Z Zhou4, S Kumar3, CB Jenkins1,2, DR Shaw1,2, TV Strong1,2, PL Triozzi1,2 and S Ponnazhagan2,3 1Department of Medicine, The University of Alabama at Birmingham, Birmingham, AL, USA; 2The Comprehensive Cancer Center, The University of Alabama at Birmingham, Birmingham, AL, USA; 3Department of Pathology, The University of Alabama at Birmingham, Birmingham, AL, USA and 4Avigen Inc., Alameda, CA, USA The potential of adeno-associated virus (AAV)-based vectors of sc rAAV6-transduced DC were comparable to nontrans- in human gene therapy is being explored for several duced DC. Efficiency of vector transduction and transgene diseases. Although sustained transgene expression and expression were confirmed by immunostaining and real-time low vector-associated cellular immunity are attractive fea- PCR. Microarray analysis of RNA from CpG ODN and CD40 tures of recombinant (r) AAV, the wider application of rAAV antibody stimulated sc AAV6-transduced DC revealed vectors encapsidated in serotype 2 capsid is hampered by upregulation of transcription factors and cytokines involved poor transduction efficiency in many target tissues. These in immune activation and downregulation of inhibitory factors, include ex vivo-generated dendritic cells (DC), which have suggesting a possible role of transcriptional activation in demonstrated promising immunotherapeutic activity. We the observed effect. The adoptive transfer into syngeneic report here that efficient transduction of mouse bone mice of the ex vivo-transduced and activated DC resulted marrow-derived DC can be achieved with self-complemen- in the development of CEA-specific antibody and T-helper tary (sc) rAAV encapsidated in serotype 6 capsid.