Electrocardiographic Passing Phenomenon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Myocarditis in the Athlete: Arrhythmogenic Substrates, Clinical Manifestations, Management, and Eligibility Decisions
Journal of Cardiovascular Translational Research https://doi.org/10.1007/s12265-020-09996-1 REVIEW ARTICLE Myocarditis in the Athlete: Arrhythmogenic Substrates, Clinical Manifestations, Management, and Eligibility Decisions Riccardo Vio1 & Alessandro Zorzi1 & Domenico Corrado1 Received: 3 October 2019 /Accepted: 24 March 2020 # Springer Science+Business Media, LLC, part of Springer Nature 2020 Abstract Myocarditis is as an important cause of sudden cardiac death (SCD) among athletes. The incidence of SCD ascribed to myocarditis did not change after the introduction of pre-participation screening in Italy, due to the transient nature of the disease and problems in the differential diagnosis with the athlete’s heart. The arrhythmic burden and the underlying mechanisms differ between the acute and chronic setting, depending on the relative impact of acute inflammation versus post-inflammatory myocardial fibrosis. In the acute phase, ventricular arrhythmias vary from isolated ventricular ectopic beats to complex tachy- cardias that can lead to SCD. Atrioventricular blocks are typical of specific forms of myocarditis, and supraventricular arrhyth- mias may be observed in case of atrial inflammation. Athletes with acute myocarditis should be temporarily restricted from physical exercise, until complete recovery. However, ventricular tachycardia may also occur in the chronic phase in the context of post-inflammatory myocardial scar. Keywords Myocarditis . Athletes . Sport . Ventricular ARVC Arrhythmogenic right ventricular cardiomyopathy tachycardia . Ventricular fibrillation . Atrial fibrillation . Atrioventricular block . Sudden death Introduction Abbreviations Myocarditis is an inflammatory disease of the heart muscle AM Acute myocarditis most often caused by infectious agents (infective myocar- SCD Sudden cardiac death ditis), autoimmune conditions, or pharmacological and en- EMB Endomyocardial biopsy vironmental toxins (non-infective myocarditis) [1]. -

Severe Arrhythmias in Coxsackievirus B3 Myopericarditis
Arch Dis Child: first published as 10.1136/adc.53.2.174 on 1 February 1978. Downloaded from 174 Short reports Oh, W., and Karecki, H. (1972). Phototherapy and insensible Table Results of clinical chemistry water loss in the newborn infant. American Journal of Diseases of Children, 124, 230-232. Oh, W., Yao, A. C., Hanson, J. S., and Lind, J. (1973). Date: September Peripheral circulatory response to phototherapy in Investigation newborn infants. Acta Paediatrica Scandinavica, 62, 49-54. (normal max) 6 7 9 10 14 23 Smales, 0. R. C. (1978). Simple method for measuring Blood urea 13-2 18-6 23-0 11-2 9*5 3-9 oxygen consumption in babies. Archives of Disease in (2*7-7 5 mmol/l) Childhood, 53, 53-57. Alananine Wilcoxon, F. (1945). The signed ranks test. Biometrics aminotransferase 2562 4987 7185 Bulletin, 1, 80. (100-500 nkat/1) Wu, P. Y. K., and Berdahl, M. (1974). Irradiance in incubators Aspartate aminotransferase 8000 7935 6000 under phototherapy lamps. Journal of Pediatrics, 84, (75-400 nkat/1) 754-755. Glutamin oxalotransferase 226 68 10 (9-19 IU/1) 0. R. C. SMALES Glutamic Department of Child Health, University Hospital and phosphorotransferase 687 207 16 (5-17 IU/1) Medical School, Nottingham NG7 2UH. Creatine kinase 133 11 12 (0-1 17 IU/1) Lactic dehydrogenase 1368 691 217 (115-457 IU/1) Severe arrhythmias in Alkaline phosphatase 75 100 117 (25-103 IU/1) Coxsackievirus B3 myopericarditis Bilirubin 7 13 18 (0-22 ,umol/l) Proven viral myopericarditis onlyrarely presents with Conversion: SI to traditional units-Blood urea: 1 mmol/l 6 02 life-threatening arrhythmias. -

An Unusual Case of Idiopathic Hypereosinophilic Syndrome Presenting with Myopericarditis and a Polypoid Cardiac Mass
Türk Kardiyol Dern Arş - Arch Turk Soc Cardiol 2014;42(3):281-284 doi: 10.5543/tkda.2014.83284 281 An unusual case of idiopathic hypereosinophilic syndrome presenting with myopericarditis and a polypoid cardiac mass Miyoperikardit ve polipoid kardiyak kitle ile ortaya çıkan nadir bir idiyopatik hipereozinofilik sendromlu olgu Özgül Uçar Elalmış, M.D., Candan Mansuroğlu, M.D., Hülya Çiçekçioğlu, M.D., Ahmet Karagöz, M.D.# Department of Cardiology, Ankara Numune Training and Research Hospital, Ankara; #Department of Cardiology, Giresun Professor Doctor Atilla İlhan Özdemir State Hospital, Giresun Summary– Idiopathic hypereosinophilic syndrome (IHES) is Özet– İdiyopatik hipereozinofilik sendrom (İHES), çoklu a rare systemic disorder with blood eosinophilia and multiple sistem tutulumu ve eozinofili ile seyreden nadir sistemik bir system involvement. Commonly, there is endocardial fibro- hastalıktır. Genellikle altta yatan mural trombüs ile birlikte sis with overlying mural thrombus, and mitral and tricuspid endokartta fibröz mevcut olup mitral ve triküspit kapaklar valves can be involved concomitantly. Outflow tracts near eş zamanlı olarak etkilenebilir. Aort ve pulmoner kapak çı- the aortic and pulmonary valves are generally protected. We kış yolları genellikle korunmuştur. Biz burada steroit tedavi- herein describe an atypical case of IHES with a mass on the si ile regresyon gösteren sol ventrikül çıkış yolunda (LVOT) left ventricular outflow tract (LVOT), which showed regres- bir kitle ile birlikte seyreden, atipik bir idiyopatik hipereozi- sion under steroid therapy. There are two features that make nofilik sendromlu olguyu sunduk. Bu olgunun sunulmasını our case worthy of reporting: First, the mitral and tricuspid değerli kılan iki özellik vardır: Birincisi, İHES’de mitral ve valves are expected to be involved in IHES, and outflow triküspit kapak tutulumu beklenir ve aort ve pulmoner ka- tracts near the aortic and pulmonary valves are generally pak çıkış yollarında etkilenme son derece nadirdir. -

The Spectrum of COVID-19-Associated Myocarditis: a Patient-Tailored Multidisciplinary Approach
Journal of Clinical Medicine Article The Spectrum of COVID-19-Associated Myocarditis: A Patient-Tailored Multidisciplinary Approach Giovanni Peretto 1,2,3,*, Andrea Villatore 3 , Stefania Rizzo 4, Antonio Esposito 2,3,5, Giacomo De Luca 2,6, Anna Palmisano 2,5, Davide Vignale 2,5, Alberto Maria Cappelletti 7, Moreno Tresoldi 8,9, Corrado Campochiaro 2,6 , Silvia Sartorelli 2,6, Marco Ripa 9,10 , Monica De Gaspari 4 , Elena Busnardo 2,11, Paola Ferro 11, Maria Grazia Calabrò 12, Evgeny Fominskiy 12 , Fabrizio Monaco 12 , Giulio Cavalli 6, Luigi Gianolli 11, Francesco De Cobelli 3,5 , Alberto Margonato 7, Lorenzo Dagna 3,6, Mara Scandroglio 12, Paolo Guido Camici 3, Patrizio Mazzone 1, Paolo Della Bella 1, Cristina Basso 4 and Simone Sala 1,2 1 Department of Cardiac Electrophysiology and Arrhythmology, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy; [email protected] (P.M.); [email protected] (P.D.B.); [email protected] (S.S.) 2 Myocarditis Disease Unit, IRCCS San Raffaele Scientific Institute, 20132 Milan, Italy; [email protected] (A.E.); [email protected] (G.D.L.); [email protected] (A.P.); [email protected] (D.V.); [email protected] (C.C.); [email protected] (S.S.); [email protected] (E.B.) 3 School of Medicine, San Raffaele Vita-Salute University, 20132 Milan, Italy; [email protected] (A.V.); [email protected] (F.D.C.); [email protected] (L.D.); [email protected] (P.G.C.) 4 Department of Cardiac Thoracic Vascular Sciences and Public Health, -

Sinus Node Ischemia—A Unique Presentation
International Journal of Clinical Medicine, 2015, 6, 50-54 Published Online January 2015 in SciRes. http://www.scirp.org/journal/ijcm http://dx.doi.org/10.4236/ijcm.2015.61007 Sinus Node Ischemia—A Unique Presentation Jwalit Morakhia1, Padmakumar Ramachandran1, Naveen Chandra Ganiga Sanjeeva1, Harikrishna Damodaran2, Shivani Kothari3, Ashok Thakkar3 1Department of Cardiology, Kasturba Medical College & Hospital, Karnataka, India 2Department of Cardiology, Pariyaram Medical College, Kerala, India 3Department of Clinical Trials, Sahajanand Medical Technologies Pvt. Ltd., Gujarat, India Email: [email protected] Received 27 December 2014; accepted 13 January 2015; published 20 January 2015 Copyright © 2015 by authors and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract Sinus node dysfunction, as the sole manifestation of an acute coronary syndrome, is rare. We re- port a case of ischemic dysfunction of the sinus node in a patient who had previously undergone coronary artery bypass grafting for triple vessel disease. Intermittent rest angina with a junctional rhythm was noted in spite of patent grafts to all three vessels, which resolved after percutaneous revascularization of the right coronary artery. Keywords Sinus Node, Angina, Acute Coronary Syndrome, Thrombus Aspiration 1. Introduction Patients presenting with acute coronary syndromes, with atypical symptoms, are frequently misdiagnosed and under-treated. Embolic phenomena are sometimes overlooked by interventionalists as percutaneous coronary intervention is a specialty which primarily focuses on stenosis and occlusions [1]. We report a case of reversible sinus node dysfunction in the unique setting of post-coronary artery bypass grafting (CABG) status with patent grafts. -

An Extremely Rare Cause of Wolff-Parkinson
108 Erciyes Med J 2019; 41(1): 108–10 • DOI: 10.14744/etd.2018.18165 An Extremely Rare Cause of Wolff-Parkinson-White Syndrome: Rhabdomyoma in Association With Tuberous Sclerosis CASE REPORT Özlem Elkıran , Cemşit Karakurt , Damla İnce ABSTRACT Rhabdomyomas are the most common primary cardiac tumors in infants and children. They are usually associated with tuberous sclerosis (TS). As the tumors tend to regress spontaneously, surgical intervention is not usually performed unless they become obstructive or cause incessant arrhythmias. We report an extremely rare case of rhabdomyoma serving as a substrate for Wolff-Parkinson-White (WPW) syndrome and intractable supraventricular tachycardia accompanied by TS. Our case is particularly interesting because it was diagnosed prenatally. The signs of WPW syndrome disappeared from the elec- trocardiogram with the regression of the tumor. Keywords: Wolff-Parkinson-White Syndrome, child, rhabdomyoma INTRODUCTION Rhabdomyomas are the most common cardiac tumors in infants and children, and they are closely related with tuberous sclerosis (TS). A significant part of rhabdomyomas is asymptomatic, and they regress on follow-up. However, symptoms of cardiac failure, arrhythmias, and obstruction can be observed depending on their location in the heart. They require urgent medical or surgical treatment (1, 2). Cite this article as: Elkıran Ö, Karakurt C, İnce D. An Extremely Rhabdomyoma-related arrhythmias are reported as premature atrial and ventricular contractions, supraventricular Rare Cause of and ventricular tachycardia, sinus node dysfunction, atrioventricular block, and Wolff-Parkinson-White (WPW) Wolff-Parkinson-White syndrome (1, 3, 4). There are only a few studies of WPW syndrome occurring in association with TS, with and Syndrome: Rhabdomyoma in Association With without rhabdomyoma. -

A Case of Myopericarditis.Indd 294 30/05/12 16:14 BRAZ J INFECT DIS
BRAZ J INFECT DIS. 2012;16(3):294-296 The Brazilian Journal of INFECTIOUS DISEASES www.elsevier.com/locate/bjid Case Report A case of myopericarditis associated to Campylobacter jejuni infection in the Southern Hemisphere Alberto Ficaa,*, Daniela Seelmannb, Lorena Portec, Daniela Eugenind, Ricardo Gallardoe aHead of the Infectious Diseases Unit, Hospital Militar de Santiago; Associate Professor, Universidad de Chile and Universidad de los Andes, Chile bDepartment of Medicine, Hospital Militar de Santiago, Chile cMicrobiology Unit, Clinical Laboratory, Hospital Militar de Santiago, Chile dCritical Care Unit, Hospital Militar de Santiago, Chile eCardiovascular Diseases Department, Hospital Militar de Santiago, Chile ARTICLE INFO ABSTRACT Article history: Myopericarditis is an infrequent complication of acute diarrheal illness due to Campylobacter Received 27 November 2011 jejuni, and it has been mainly reported in developed nations. The first case detected in Chile – an Accepted 17 February 2012 upper-middle income country –, that is coincidental with the increasing importance of acute gastroenteritis associated to this pathogen, is described. Recognition of this agent in stools Keywords: requires special laboratory techniques not widely available, and it was suspected when a young Campylobacter jejuni patient presented with acute diarrhea, fever, and chest pain combined with electrocardiogram Myocarditis (EKG) abnormalities and elevated myocardial enzymes. C. jejuni myopericarditis can easily be Infectious diarrheal disease suspected but its detection requires dedicated laboratory techniques. © 2012 Elsevier Editora Ltda. All rights reserved. Introduction Case presentation Viral infections are the leading cause of myocarditis and A 17-year-old adolescent male was admitted to the Hospital pericarditis in developed countries.1 On the other hand, parasitic Militar de Santiago, in September 2011, with a history of two diseases such as acute Chagas disease and endemic viruses days of upper abdominal pain, fever (38.5oC), and dysentery. -
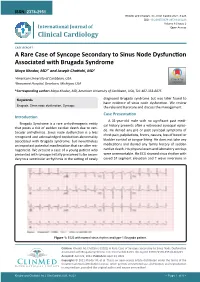
A Rare Case of Syncope Secondary to Sinus Node Dysfunction Associated with Brugada Syndrome Maya Khodor, MD1* and Joseph Chattahi, MD2
ISSN: 2378-2951 Khodor and Chattahi. Int J Clin Cardiol 2021, 8:223 DOI: 10.23937/2378-2951/1410223 Volume 8 | Issue 2 International Journal of Open Access Clinical Cardiology CASE REPORT A Rare Case of Syncope Secondary to Sinus Node Dysfunction Associated with Brugada Syndrome Maya Khodor, MD1* and Joseph Chattahi, MD2 1 American University of Caribbean, USA Check for 2Beaumont Hospital, Dearborn, Michigan, USA updates *Corresponding author: Maya Khodor, MD, American University of Caribbean, USA, Tel: 407-353-8875 diagnosed Brugada syndrome but was later found to Keywords have evidence of sinus node dysfunction. We review Brugada, Sinus node dysfunction, Syncope the relevant literature and discuss the management. Case Presentation Introduction A 31-year-old male with no significant past medi- Brugada Syndrome is a rare arrhythmogenic entity cal history presents after a witnessed syncopal episo- that poses a risk of sudden cardiac death due to ven- de. He denied any pre or post syncopal symptoms of tricular arrhythmias. Sinus node dysfunction is a less chest pain, palpitations, fevers, nausea, loss of bowel or recognized and acknowledged conduction abnormality associated with Brugada syndrome, but nevertheless bladder control or tongue biting. He does not take any an important potential manifestation that can alter ma- medications and denied any family history of sudden nagement. We present a case of a young patient who cardiac death. His physical exam and laboratory workup presented with syncope initially presumed to be secon- were unremarkable. His ECG showed sinus rhythm with dary to a ventricular arrhythmia in the setting of newly coved ST segment elevation and T wave inversions in Figure 1: ECG with normal sinus rhythm and type-1 Brugada pattern. -

Sick Sinus Syndrome After the Maze Procedure Performed
ORIGINAL RESEARCH Sick Sinus Syndrome After the Maze Procedure Performed Concomitantly With Mitral Valve Surgery Min Soo Cho, MD; Ran Heo, MD; Xin Jin, MD; Jung-Bok Lee, PhD; Sahmin Lee, MD, PhD; Dae-Hee Kim, MD, PhD; Joon Bum Kim, MD, PhD; Jun Kim, MD, PhD; Sung-Ho Jung, MD, PhD; Suk Jung Choo, MD, PhD; Jong-Min Song, MD, PhD; Gi-Byoung Nam, MD, PhD; Kee-Joon Choi, MD, PhD; Duk-Hyun Kang, MD, PhD; Cheol Hyun Chung, MD, PhD; Jae Won Lee, MD, PhD; You-Ho Kim, MD, PhD; Jae-Kwan Song, MD, PhD Background-—To characterize the development of sick sinus syndrome (SSS) after the additive maze procedure (MP) during mitral valve surgery. Methods and Results-—Follow-up data (median, 3.6 years) of 750 patients with a prevalence of rheumatic cause of 57.6% were analyzed. SSS occurred in 35 patients with a time-dependent increase: the incidence rates at 1, 2, and 4 years after surgery were 2.9%, 3.7%, and 4.3%, respectively. The additive MP showed higher risks of SSS development (hazard ratio, 7.44; 95% confidence interval, 3.45–16.05; P<0.001) and pacemaker implantation (hazard ratio, 3.61; 95% confidence interval, 1.95–6.67; P<0.001). Patients who developed SSS showed higher 4-year rates of clinical events (death, stroke, and hospital admission) (67.5Æ8.5% versus 33.0Æ1.9%; P<0.001). After adjustment for age and preoperative peak systolic pulmonary artery pressure, the lesion extent (biatrial versus left atrial MP), not the underlying cause (rheumatic versus nonrheumatic), was independently associated with SSS development (hazard ratio, 3.58; 95% confidence interval, 1.08–11.86; P=0.037). -

Management of Asymptomatic Arrhythmias
Europace (2019) 0, 1–32 EHRA POSITION PAPER doi:10.1093/europace/euz046 Downloaded from https://academic.oup.com/europace/advance-article-abstract/doi/10.1093/europace/euz046/5382236 by PPD Development LP user on 25 April 2019 Management of asymptomatic arrhythmias: a European Heart Rhythm Association (EHRA) consensus document, endorsed by the Heart Failure Association (HFA), Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), Cardiac Arrhythmia Society of Southern Africa (CASSA), and Latin America Heart Rhythm Society (LAHRS) David O. Arnar (Iceland, Chair)1*, Georges H. Mairesse (Belgium, Co-Chair)2, Giuseppe Boriani (Italy)3, Hugh Calkins (USA, HRS representative)4, Ashley Chin (South Africa, CASSA representative)5, Andrew Coats (United Kingdom, HFA representative)6, Jean-Claude Deharo (France)7, Jesper Hastrup Svendsen (Denmark)8,9, Hein Heidbu¨chel (Belgium)10, Rodrigo Isa (Chile, LAHRS representative)11, Jonathan M. Kalman (Australia, APHRS representative)12,13, Deirdre A. Lane (United Kingdom)14,15, Ruan Louw (South Africa, CASSA representative)16, Gregory Y. H. Lip (United Kingdom, Denmark)14,15, Philippe Maury (France)17, Tatjana Potpara (Serbia)18, Frederic Sacher (France)19, Prashanthan Sanders (Australia, APHRS representative)20, Niraj Varma (USA, HRS representative)21, and Laurent Fauchier (France)22 ESC Scientific Document Group: Kristina Haugaa23,24, Peter Schwartz25, Andrea Sarkozy26, Sanjay Sharma27, Erik Kongsga˚rd28, Anneli Svensson29, Radoslaw Lenarczyk30, Maurizio Volterrani31, Mintu Turakhia32, -

Sinus Node Dysfunction in Acute Myocardial Infarction
Br Heart J: first published as 10.1136/hrt.38.1.93 on 1 January 1976. Downloaded from British Heart Journal, 1976, 38, 93-96. Sinus node dysfunction in acute myocardial infarction R. Parameswaran, Tohru Ohe, and Harry Goldberg From the Cardiology Department and WLMR Laboratories, Albert Einstein Medical Center, Philadelphia, Pa., U.S.A. Thefrequency, clinical course, and prognosis of sinus node dysfunction in 431 patients with acute myocardial infarction admitted to the coronary care unit were studied. Sinus node dysfunction occurred in 20 patients. In 13, the principal manifestation consisted of severe sinus bradjvcardia. In the remaining 7, periods of bradycardia alternating with episodes of supraventricular tachycardia were noted. Though several of the patients with sinus bradycardia required intravenous atropine or temporary pacing, normal sinus rhythm returned in virtually all during follow-up. The clinical course of patients with both bradycardia and tachycardia was less benign, during the acute phase and during follow-up; 5 of the 6 survivors required continued antiarrhythmic therapy or permanent pacing. The differences in the clinical course between these two groups ofpatients may reflect distinct underlying pathological changes. Thefindings in this study suggest that in contrast to sinus bradycardia, the occurrence of bradycardia-tachycardia syndrome during the acute phase of myocardial infarction may have important prognostic implications. Sinus node dysfunction is being increasingly institution dictates the exclusion of patients with severe http://heart.bmj.com/ recognized as a cause of serious cardiac arrhythmias congestive failure and cardiogenic shock, the patients and frequently presents difficult problems in diag- included in this study were free from these major Characteristic manifestations complications of myocardial infarction at the time of nosis and therapy. -

A Case of Myopericarditis Caused by Neisseria Meningitidis W135
Clinical Medicine 2018 Vol 18, No 3: 253–5 ACUTE MEDICAL CARE A c a s e o f m y o p e r i c a r d i t i s c a u s e d b y Neisseria meningitidis W135 serogroup with protracted infl ammatory syndrome A u t h o r s : A l e x J K e e l e y , A D a n i e l H a m m e r s l e y B a n d S u k h b i r S D h a m r a i t C Meningococcal pericarditis is classically divided into three separate entities: isolated meningococcal pericarditis, dissemi- nated meningococcal disease with pericarditis, and reactive (immunopathic) meningococcal pericarditis. We present the case of a 74-year-old woman with meningococcal septicaemia ABSTRACT with meningococcal myopericarditis, which demonstrates crossover features. Case presentation A 74-year-old caucasian woman with no history of immunosuppression or rheumatological disease, but with a history of paroxysmal atrial fibrillation (AF) for which she was taking flecainide but no anticoagulation, was admitted following a Baltic cruise holiday. She had fever, rigors, chest pain radiating Fig 1. 12-lead electrocardiogram showing atrial fi brillation with a rapid to the back and neck, and progressive breathlessness of several ventricular response, with subtle widespread ST segment elevation days onset. On initial examination, she was in respiratory distress with ST segment depression in leads aVR and V1. with a respiratory rate of 24 breaths/minute, oxygen saturations of 92% on 28% oxygen, tachycardia of 146 beats/minute, blood pressure of 133/73 mmHg and a temperature of 37.5°C.