Lapponia 2015 Intro FMID
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
TENSILE FABRIC ARCHITECTURE: the Process the Characteristics of a Tensile Fabric Structure Are Very Different Than Traditional Building Components
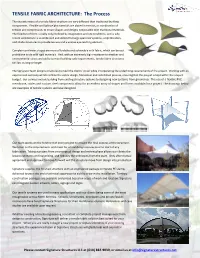
TENSILE FABRIC ARCHITECTURE: The Process The characteristics of a tensile fabric structure are very different than traditional building components. Flexible and lightweight materials are placed in tension, or combination of tension and compression, to create shapes and designs not possible with traditional materials. The freedom of form is really only confined by imagination and site conditions; and is why tensile architecture is so embraced and utilized for large span roof systems, amphitheaters, and shade structures to provide texture and a unique eye catching element.. Complex curvilinear shapes are more affordable and achievable with fabric, which can be cost prohibitive to do with rigid materials. And, with an extremely high resistance to weather and environmental stress and ability to meet building code requirements, tensile fabric structures can last as long or longer. The Signature Team designs structures to meet the clients’ vision while incorporating the underlining requirements of the project. Working with an experienced company will streamline the entire design, fabrication and installation process, ensuring that the project is kept within the project budget. Our services include building from existing structure systems to designing new systems from ground up. The use of a flexible PVC membrane, cables and custom steel components allow for an endless array of shapes and forms available for a project. The drawings below are examples of tensile systems we have designed. Our team works on the forefront of every project to ensure the final success of the structure. We listen to the requirements and meet for a final design review prior to start of any fabrication. Taking a project from a conceptual design and review phase allows our clients the lowest estimates on final pricing, and reduces the unknowns from the start. -

Computational Methods for Tension-Loaded Structures
Arch. Comput. Meth. Engng. Vol. 11, 2, 143-186 (2004) Archives of Computational Methods in Engineering State of the art reviews Computational Methods for Tension-Loaded Structures Thouraya Nouri-Baranger Centre de M´ecanique Universit´e Claude Bernard Lyon 1, France E-mail: [email protected] Summary This paper deals with tension loaded structures made of coated woven fabric, cables and rigid frames such as mats and hoops. It describes in details a general framework for modelling and numerical simulation of their mechanical behavior. Several methods, developped in these last decades, are presented and compared. The principal particularity of these structures is that they derive their stiffness and their stability from the surface geometry and tensile stress field coupling. This particularity is combined with nonlinearities which can be due to possible large deflections, material law behavior and local instabilities due to wrinkling effects. In addition, a great number of design parameters must be taken into account in order to optimize the mechanical behavior of the structure. Therefore, the design and the analysis of such structure are complex and involve extensive computational costs. The principal steps of the analysis process are: form-finding, structural response of the structure to loads, cutting pattern and optimization. In this work, after a short description of the methods developed in this field as well as a critical comparison, new approaches are proposed. 1INTRODUCTION A growing number of architectural structures are today protected by fabrics that are ten- sioned over structures such as plywood, concrete and metal. The most significant membrane structures include the Haj Terminal at Jeddah (Saudia Arabia) whose roof extends over a 430000 m2 surface, the arenas of Nˆımes (France) and Zaragoza (Spain) and the Mil- lennium dome− in Greenwich (United Kingtom). -

Shape Finding Or Form Finding?
Proceedings of the IASS-SLTE 2014 Symposium “Shells, Membranes and Spatial Structures: Footprints” 15 to 19 September 2014, Brasilia, Brazil Reyolando M.L.R.F. BRASIL and Ruy M.O. PAULETTI (eds.) Shape Finding or Form Finding? By Nicholas S. GOLDSMITH, FAIA LEED AP FTL Design Engineering Studio 44 East 32nd Street New York, NY 10016 [email protected] Abstract This lecture will discuss the differences in the design process between a shape finding and a form finding approach. It will examine historical traditions of both approaches and look at these methods in today’s design world. Examples of the work of FTL will be used as descriptive case studies to illustrate the different aspects of membrane envelopes including ETFE foil cushions, tensile membranes, and cable nets. Keywords: building membranes, acoustics, environmental, soap films, biomimetics, form-finding, shape finding, lighting, ETFE foil, PTFE glass, Frei Otto In the 18th century, naturalists started a movement which arose from a desire to understand the "universal laws of form" in order to explain observed forms of living organisms. Although it didn’t have much traction at the time, during the early 20th century pioneers such as D’Arcy Wentworth Thompson expanded these notions to create a modern understanding that there are universal laws which arise from fundamental math and physics and that reflect the growth and form in biological systems. Thompson worked on the correlation between natural forms and mathematical models and showed similarities between such things as jellyfish forms and drops of liquid. His book, On Growth and Form became an important way finder in the study of nature and the instrumental in the later emergence of the field of biomimetics1. -

Copyrighted Material
COPYRIGHTED MATERIAL c01.indd 12 12/9/2014 9:51:11 AM Building with hyperbolic lattice structures 14 The development of building with iron in the 19th century 14 The work of Vladimir G. Shukhov, pioneer of lightweight construction 15 The hyperbolic lattice towers of Vladimir G. Shukhov 19 Hyperbolic structures after Shukhov 23 Geometry and form of hyperbolic lattice structures 24 Principles and classification 24 Geometry of hyperbolic lattice structures 28 Structural analysis and calculation methods 32 The problem of inextensional bending 32 Principal structural behaviour 32 Theoretical principles for determining ultimate load capacity 38 Parametric studies on differently meshed hyperboloids 45 Principles of the parametric studies 45 Relationships between form and structural behaviour 50 Comparison of circular cylindrical shells and hyperboloids of rotation 50 Mesh variant 1: Intermediate rings at intersection points 50 Mesh variant 2: Construction used by Vladimir G. Shukhov 52 Mesh variant 3: Discretisation of reticulated shells 57 Summary and comparison of the results 59 Structural analysis of selected towers built by Vladimir G. Shukhov 60 Design and analysis of Shukhov’s towers 66 The development of steel water tanks and water towers 66 The water towers of Vladimir G. Shukhov 69 Development of structural analysis and engineering design methods in the 19th century 70 Calculations for Vladimir G. Shukhov’s lattice towers 70 Evaluation of the historical calculations 84 The design process adopted by Vladimir G. Shukhov 89 13 c01.indd 13 12/9/2014 9:51:11 AM Building with hyperbolic lattice structures Building with hyperbolic lattice structures began with the Russian the flow of conventional skilled craftsmen’s operations on site. -
Tensegrity Structures and Their Application to Architecture
Tensegrity Structures and their Application to Architecture Valentín Gómez Jáuregui Tensegrity Structures and their Application to Architecture “Tandis que les physiciens en sont déjà aux espaces de plusieurs millions de dimensions, l’architecture en est à une figure topologiquement planaire et de plus, éminemment instable –le cube.” D. G. Emmerich “All structures, properly understood, from the solar system to the atom, are tensegrity structures. Universe is omnitensional integrity.” R.B. Fuller “I want to build a universe” K. Snelson School of Architecture Queen’s University Belfast Tensegrity Structures and their Application to Architecture Valentín Gómez Jáuregui Submitted to the School of Architecture, Queen’s University, Belfast, in partial fulfilment of the requirements for the MSc in Architecture. Date of submission: September 2004. Tensegrity Structures and their Application to Architecture I. Acknowledgments I. Acknowledgements In the month of September of 1918, more or less 86 years ago, James Joyce wrote in a letter: “Writing in English is the most ingenious torture ever devised for sins committed in previous lives.” I really do not know what would be his opinion if English was not his mother tongue, which is my case. In writing this dissertation, I have crossed through diverse difficulties, and the idiomatic problem was just one more. When I was in trouble or when I needed something that I could not achieve by my own, I have been helped and encouraged by several people, and this is the moment to say ‘thank you’ to all of them. When writing the chapters on the applications and I was looking for detailed information related to real constructions, I was helped by Nick Jay, from Sidell Gibson Partnership Architects, Danielle Dickinson and Elspeth Wales from Buro Happold and Santiago Guerra from Arenas y Asociados. -

Modelling and Control of Tensegrity Structures
Modelling and Control of Tensegrity Structures Anders Sunde Wroldsen A Dissertation Submitted in Partial Fulfillment of the Requirements for the Degree of PHILOSOPHIAE DOCTOR Department of Marine Technology Norwegian University of Science and Technology 2007 NTNU Norwegian University of Science and Technology Thesis for the degree of philosophiae doctor Faculty of Engineering Science & Technology Department of Marine Technology c Anders Sunde Wroldsen ISBN 978-82-471-4185-4 (printed ver.) ISBN 978-82-471-4199-1 (electronic ver.) ISSN 1503-8181 Doctoral Thesis at NTNU, 2007:190 Printed at Tapir Uttrykk Abstract This thesis contains new results with respect to several aspects within tensegrity research. Tensegrity structures are prestressable mechanical truss structures with simple dedicated elements, that is rods in compression and strings in tension. The study of tensegrity structures is a new field of research at the Norwegian University of Science and Technology (NTNU), and our alliance with the strong research community on tensegrity structures at the University of California at San Diego (UCSD) has been necessary to make the scientific progress presented in this thesis. Our motivation for starting tensegrity research was initially the need for new structural concepts within aquaculture having the potential of being wave com- pliant. Also the potential benefits from controlling geometry of large and/or interconnected structures with respect to environmental loading and fish welfare were foreseen. When initiating research on this relatively young discipline we discovered several aspects that deserved closer examination. In order to evaluate the potential of these structures in our engineering applications, we entered into modelling and control, and found several interesting and challenging topics for research. -

Adaption of Tensile Architecture in Tropical Monsoon Climate
International Journal of Applied and Physical Sciences volume 5 issue 1 pp. 08-19 doi: https://dx.doi.org/10.20469/ijaps.5.50002-1 Adaption of Tensile Architecture in Tropical Monsoon Climate Latifa Sultana ∗ Nazmun Nahar Architecture Department, Monad Architects, Dhaka, Bangladesh Southeast University, Dhaka, Bangladesh Abstract: This paper will thoroughly investigate the use and opportunities of tensile architecture, which can be applied in rain, wind, heat, daylight issues in the architecture of Bangladesh. As Bangladesh laid on Intertropical Convergence Zone (ITCZ), the built form of this region prefers an open-type structure. Humidity and temperature always become an issue in this region due to the tropical monsoon climate of Bangladesh. These issues of environment follow the traditional Bengal architecture pattern. Furthermore, the contemporary architecture of Bangladesh respectively follows these significant characteristics of tropical monsoon climate. On the other side, Tensile Membrane Structure (TMS) has qualities to hold large spans, lightweight, translucency, aesthetic value, and flexibility. TMS and the traditional hut system of Bengal can be said as complementary to each other in this tropical monsoon climate of Bangladesh. Tensile membrane structure can be that element of contemporary architecture that can be adopted in this climate by satisfying all the primary issues of the tropical monsoon climate of Bangladesh. Tensile structure can be designed as lightweight roof shade, which is more similar with “Bengal hut” pattern of Bangladesh. Keywords: Climate, hut pattern, tensile structure, fabric Received: 06 November 2018; Accepted: 12 February 2019; Published: 08 March 2019 I. INTRODUCTION Moreover, Bangladesh is the deltaic pavilion of Southeast A. Background Asia. -
The Obverse/Reverse Pavilion: an Example of a Form-Finding Design of Temporary, Low-Cost, and Eco-Friendly Structure
buildings Article The Obverse/Reverse Pavilion: An Example of a Form-Finding Design of Temporary, Low-Cost, and Eco-Friendly Structure Jerzy F. Ł ˛atka 1,* and Michał Swi˛eciak´ 2 1 Department of Architecture and Visual Arts, Faculty of Architecture, Wroclaw University of Science and Technology, 50-317 Wroclaw, Poland 2 Super Architektura Michał Swi˛eciak,86-300´ Grudzi ˛adz,Poland; [email protected] * Correspondence: [email protected] Abstract: Temporary pavilions play an important role as experimental fields for architects, designers, and engineers, in addition to providing exhibition spaces. Novel structural and formal solutions applied in pavilions also can give them an unusual appearance that attracts the eyesight of spectators. In this article, the authors explore the possibility of combining structural novelty, visual attractiveness, and low cost in the design and construction of a temporary pavilion. For that purpose, an innovative structural system and design approach was applied, i.e., a membrane structure was designed in Rhino and Grasshopper environments with the use of the Kiwi!3D IsoGeometric analysis tool. The designed pavilion, named Obverse/Reverse, was built in Opole, Poland, for the occasion of World Architecture Day in July 2019. The design and the construction were performed by the authors in cooperation with students belonging to the Humanization of Urban Environment organization from the Faculty of Architecture Wroclaw University of Science and Technology. The resultant pavilion proved the potential of obtaining a low-budget but visually attractive architectural solution with the adaption of parametrical design tools and some scientific background with innovative structural systems. Citation: Ł ˛atka,J.F.; Swi˛eciak,M.´ The Obverse/Reverse Pavilion: An Keywords: parametric design; paper in architecture; temporary architecture; pop-up structures; Example of a Form-Finding Design of membrane structures; isogeometric analysis; fabrication Temporary, Low-Cost, and Eco-Friendly Structure. -

A Deployable Mast for Adaptable Architecture
A Deployable Mast for Adaptable Architecture N. De Temmerman1, M. Mollaert1, L. De Laet1, C. Henrotay1, A. Paduart1, L. Guldentops1, T. Van Mele1, W. Debacker1 Æ-lab (Research Group for Architectural Engineering), Department of Architectonic Engineering Sciences, Vrije Universiteit Brussel Pleinlaan 2, 1050 Brussels – Belgium Abstract Proposed here is a concept for a deployable mast with angulated scissor units, for use in adaptable temporary architectural constructions. The adaptable structure serves as a tower or truss-like mast for a temporary tensile surface structure and doubles up as an active element during the erection process. The mast consists of scissor-like elements (SLE’s) which are an effective way of introducing a single D.O.F.(degree of freedom) mechanism into a structure, providing it with the necessary kinematic properties for transforming from a compact state to a larger, expanded state. The scissor units used here are not comprised of straight bars, but rather consist of angulated elements, i.e. bars having a kink angle. Although primarily intended for radially deployable closed loop structures, it is shown in this paper that angulated elements can also prove valuable for use in a linear three-dimensional scissor geometry. Keywords: Deployable structures, transformable structures, adaptable architecture, angulated scissor elements, kinetic architecture for additional lifting equipment. After connections between 1 INTRODUCTION the membrane elements and the mast have been made, An innovative concept for a deployable hyperboloid mast the mechanism is deployed until the required height is with angulated scissor elements is presented. The scissor reached and the membrane elements become tensioned. structure is a central vertical linear element, used to hold The mast could be deployed to such an extent that a up several anticlastic membrane canopies at their high sufficient amount of pre-tension is introduced in the points. -

Horst Berger First, and Later with a Pair of Draft Horses, at Stuttgart, Horst Considered Changing His One Elderly and the Other Pregnant
GREAT ACHIEVEMENTS notable structural engineers But the tranquility of life in the country Engineering & Architecture was soon shattered by political turmoil and World War II. Education ® In 1944, his high school class was drafted In 1949, a rare opportunity presented itself into service manning anti-aircraft guns to for Horst to continue his studies. He was defend the industrial city of Mannheim one of 124 individuals selected from 32,000 from allied air attacks. Horst saw Mannheim applicants for a program that allowed German reduced to rubble from behind the sights of students to study in the United States. He an 88 mm gun as the city was pounded by traveled to New York on a troop transport over 130 strategic bombing raids during a ship along with 4,000 returning service men. period of 13 months. Horst went to Iowa State College where At the end of the war, 16 year old Horst, he studied architecture and psychology. war wearyCopyright and glad to be alive, hiked for Unleashed from the restrictive postwar two weeks back to his hometown amidst the environment that he had left at home, Horst chaos of the retreating German army. When enjoyed the free atmosphere of the U.S. He he arrived home he found a scared landscape traveled whenever possible. While attending with no government, no schools, no order an International Student Seminar sponsored and no opportunities for a young man. by the Quakers in Massachusetts, he met With barely enough food available to stay Gay, the woman who would later become his alive, Horst was able to sustain himself wife. -
Combine It for the Better! the First Composite Material, Two Or More Materials Combined to Make an Even Better Material, Was Made in 1500 BC by the Egyptians
May the Force Be With You You’re late for school! You react by jumping up, plunking your coffee mug down on the kitchen counter and running out the door. You probably didn’t give it any thought but there were many forces acting on you in those few seconds. They range from the forces used to hold that daily cup of coffee, to the forces that our feet exert against the ground to get us moving and of course, the force of gravity. Forces are applied everywhere all the time! Background Information Forces A force is a push or pull on an object. Forces have direction and magnitude and depending on these two factors, it can cause an object to change its speed, direction, shape or pressure within. Engineers use arrows called vectors to represent direction and magnitude of force, the larger the arrow, the larger the force. Newtons (N) are used to measure force. One Newton is equal to the force required to cause a mass of 1 kilogram to accelerate at a rate of 1 meter per second per second (m/s2) in the absence of other force-producing effects. Sir Isaac Newton’s laws of motion lay the foundation for the interaction of forces and motion. Newton’s first law is that an object will remain at rest or move at the same speed unless an unbalanced force acts on it. For example, if two people apply an equal force on a ball in opposite directions then the ball will not move and it is considered to be in equilibrium. -

Tension Arch Structure
Transportation Research Record 982 l Tension Arch Structure SAM G. BONASSO and LYLE K. MOULTON ABSTRACT costly to build initially and that contain features that make continued maintenance difficult and expen sive. The Tension Arch structure is introduced and For example, in the design of conventional high explained. The Tension Arch principle, when way bridge systems, the cost savings that can be incorporated in an innovative bridge struc achieved by making the superstructure continuous ture, has the potential for solving many of over the piers has long been recognized. In fact, in the problems that have plagued conventional many states, a relatively large percentage of the bridge designs over the years. It offers multispan bridges are designed for partial or total more efficient use of mateiialsi can be used continuity. However, in recognition of the fact with a variety of materials, including that these continuous bridges may be more sensitive steel, concrete, and timberi can achieve to differential settlements than simp.ly supportea lower construction costs through reduced de bridges, the majority of states found these struc sign cost, mass production of compressive tures on piles, or other deep foundations, unless and tensile components, minimum shop and rook or some other hard foundation material is lo field custom fabrication, and reduced erec cated close to the proposed foundation level ( 10) • tion time and erection equipment costs; and In many instances, the cost of these deep founda provides a geometry that is relatively in tions may be substantially greater than the savings sensitive to a variety of support movements achieved by making the superstructure continuous.