Qwertyuiopasdfghjklzxcvbnmqw
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
CAMPAIGN FINANCIAL REPORT TOTAL TOTAL CURRENT ACCOUNT BALANCE: $___I Certify That This Is a Full and True Statement
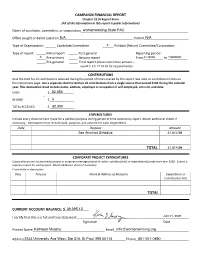
CAMPAIGN FINANCIAL REPORT Chapter 211A Report Form (All of the information in this report is public information) Name of candidate, committee, or corporation_______________________________womenwinning State PAC _____________________________ Office sought or ballot question ___N/A______________________________________ District_____N/A ____________________ Type of Organization: ______ Candidate Committee ______X Political (Action) Committee/Corporation Type of report: _____ Initial report _____ Post-general Reporting period: __X___ Pre-primary _____ January report From_1/1/2020__________ to ___________7/26/2020 _____ Pre-general _____ Final report (closes committee account – see M.S. Ch. 211A.03 for requirements) CONTRIBUTIONS Give the total for all contributions received during the period of time covered by this report. See note on contribution limits on the instructions page. Use a separate sheet to itemize all contributions from a single source that exceed $100 during the calendar year. This itemization must include name, address, employer or occupation if self-employed, amount, and date. CASH $_______________32,350 + IN-KIND $_______________0 = TOTAL RECEIVED $ _______________32,350 EXPENDITURES Include every disbursement made for a political purpose during period of time covered by report. Attach additional sheets if necessary. Itemization must include date, purpose, and amount for each expenditure. Date Purpose Amount See Attached Schedule 31,614.98 TOTAL 31,614.98 CORPORATE PROJECT EXPENDITURES Corporations must list any media project -

November 6, 2020
Metro Cities News November 6, 2020 Reminder: CRF Spending Reports Due November 10 The next Coronavirus Relief Fund (CRF) spending reports, for spending by local governments through October 31st, are due next Tuesday, November 10th. The deadline for cities to spend their CRF allocation is November 15th. Any funds returned to counties must be returned by November 20th. The Office of MN Management and Budget (MMB) FAQ document can be found here: https://mn.gov/mmb-stat/crao/faqs-for-local-governments-as-of-sept-25-411pm.pdf Please contact Patricia Nauman at 651-215-4002 or [email protected] with any questions. RSVP for November 19 Policy Adoption Meeting! Metro Cities’ policy adoption meeting will be held remotely on Thursday, November 19th at 4:00 p.m. at which time 2021 legislative policies will be adopted by the membership. Draft policies are available for review here. Protocols for policy adoption were emailed to city managers and administrators and additional details will be provided in advance of the meeting. Cities are asked to select delegates for voting purposes and attendance is open to all member city officials and staff. Your presence is important and appreciated. Metro Cities has invited Briana Bierschbach from the Star Tribune and Brian Bakst from Minnesota Public Radio (MPR) on the 19th to share their insights on the elections and upcoming legislative session. Please RSVP to [email protected] or 651-215-4000. We look forward to seeing you! Elections Shift Several Legislative Seats – Split Majorities Maintained This election cycle, in addition to the presidential and national elections, the 201 state legislative seats were up for election. -

Alzheimer's Disease Working Group
Impact of Alzheimer’s in Minnesota 91,000 people in Minnesota aged 65 and older living with Alzheimer’s, and more than 5 million nationwide Medicaid costs are set to skyrocket to $1 billion 249,000 Alzheimer’s caregivers by in Minnesota are providing 2025 as the baby 284 million hours of unpaid care valued at nearly boomers continue $3.5 billion to enter the age of greatest risk for Alzheimer’s 2015 Medicaid costs of caring for people in Minnesota with Alzheimer’s were estimated to be $767 million Alzheimer’s is the th 6 leading cause of death in Minnesota 17 RD Rally Day MN Handbook.indd 6 2/2/17 3:00 PM Impact of Alzheimer’s in Minnesota Alzheimer’s Disease Working Group Support the bill to reconvene the Alzheimer’s Disease Working Group Review and revise the recommendations to Legislature to ensure that Minnesota is prepared for Alzheimer’s. House File 262 - Senate File 120 Senate Authors: Carla Nelson, Sandra Pappas, Karin Housley, Paul T. Anderson, Patricia Torres Ray House Authors: Debra Kiel, Jeanne Poppe, Tim O’Driscoll, Jeff Howe, Erin Murphy Alzheimer’s is the most expensive disease in America and there is currently no means to slow, stop or prevent this disease. Alzheimer’s takes a significant toll on individuals, families and on our state budget. The State of Minnesota and our communities must be prepared to address Alzheimer’s. We can do that by reviewing and revising the recommendations by the 2009 Alzheimer’s Disease Working Group, which included 24 recommendations in seven different key areas. -

Edallies Legislative Scorecard Educational Excellence & Equity at the Capitol
EdAllies Legislative Scorecard Educational Excellence & Equity at the Capitol 2017–2018 TABLE OF CONTENTS EdAllies Legislative Scorecard Educational Excellence and Equity at the Capitol 2017-2018 Introduction 2 What’s in the Scorecard 3 Issues Diverse & Effective Educators 4 School Discipline 11 Data & Transparency 14 Welcoming & Accessible Schools 18 Parent Choice 22 Final Votes: The Omnibus Bills 26 Vote Tables House 29 Senate 40 EdAllies Legislative Scorecard 2017–2018 1 INTRODUCTION Dear partners, At EdAllies, we work to ensure that every young Minnesotan has access to a rigorous and engaging education—work we simply cannot do without empowered, informed advocates. Yet, too often, Minnesota’s confusing policymaking process makes it hard to understand what’s happening with education policy change at the Capitol. Given our state’s urgent need to address opportunity and achievement gaps, this is unacceptable. To accomplish more for Minnesota students, we need greater transparency around policy progress and setbacks. We made this legislative scorecard to help you understand education efforts over the last two years, also known as the legislative biennium. We recap key policies that legislators introduced, our position, and, when possible, the votes. Though our policymakers didn’t make as much progress for Minnesota students as we hoped during the 90th biennium, they made some notable changes. For example, our legislators reached across the aisle to: • open Minnesota’s doors to great out-of-state and alternatively prepared educators; • support new programs to recruit and retain teachers of color; • advance trailblazing legislation to disaggregate student achievement data, and more. Of course, there’s much more work to do to set up all Minnesota students for success. -

Senate District Reports by Institution
Alexandria Technical and Community College Credit Student Enrollment by Senate District Fiscal Year 2018-2019 Senator and District Enrollment District 12: Sen. Torrey Westrom 817 District 08: Sen. Bill Ingebrigtsen 727 District 01: Sen. Mark Johnson 298 District 09: Sen. Paul Gazelka 226 District 02: Sen. Paul Utke 185 District 17: Sen. Andrew Lang 132 District 04: Sen. Kent Eken 99 District 13: Sen. Jeff Howe 93 District 16: Sen. Gary Dahms 91 District 18: Sen. Scott Newman 61 District 14: Sen. Aric Putnam 60 District 05: Sen. Justin Eichorn 58 District 15: Sen. Andrew Mathews 56 District 21: Sen. Michael Goggin 55 District 29: Sen. Bruce Anderson 46 District 30: Sen. Mary Kiffmeyer 38 District 22: Sen. Bill Weber 35 District 31: Sen. Michelle Benson 28 District 10: Sen. Carrie Ruud 26 District 06: Sen. David Tomassoni 26 District 11: Sen. Jason Rarick 24 District 23: Sen. Julie Rosen 24 District 32: Sen. Mark Koran 22 District 24: Sen. John Jasinski 21 District 47: Sen. Julia Coleman 20 District 58: Sen. Zach Duckworth 20 District 28: Sen. Jeremy Miller 17 District 20: Sen. Rich Draheim 17 District 35: Sen. Jim Abeler 16 District 37: Sen. Jerry Newton 15 District 19: Sen. Nick Frentz 15 District 33: Sen. David Osmek 14 District 25: Sen. David Senjem 12 District 55: Sen. Eric Pratt 11 District 39: Sen. Karin Housley 11 District 34: Sen. Warren Limmer 11 District 03: Sen. Tom Bakk 10 District 40: Sen. Chris Eaton 9 District 42: Sen. Jason Isaacson 9 System Office Research, Academic and Student Affairs Division 11/19/2020 Alexandria Technical and Community College Credit Student Enrollment by Senate District Fiscal Year 2018-2019 Senator and District Enrollment District 56: Sen. -

House Legislature
VOLUME ONE JOURNAL OF THE HOUSE OF REPRESENTATIVES NINETIETH SESSION OF THE LEGISLATURE STATE OF MINNESOTA 2017 _____________ P UBLISHED BY THE CH IE F C LERK'S O FFICE M INNES OTA HOUSE OF REPRESENTATIVES 1ST DAY] TUESDAY, JANUARY 3, 2017 3 STATE OF MINNESOTA NINETIETH SESSION - 2017 _____________________ FIRST DAY SAINT PAUL, MINNESOTA, TUESDAY, JANUARY 3, 2017 In accordance with the Constitution and the Laws of the State of Minnesota, the members-elect of the House of Representatives assembled in the Chamber of the House of Representatives in the Capitol in Saint Paul on Tuesday, the third day of January 2017. At the hour of twelve o'clock noon and pursuant to Minnesota Statutes 2016, Section 3.05, the Honorable Steve Simon, Secretary of State, called the members-elect to order and appointed the Honorable Sondra Erickson from District 15A as Clerk pro tempore. Prayer was offered by Archbishop Bernard A. Hebda, Archdiocese of Saint Paul and Minneapolis, St. Paul, Minnesota. The members-elect of the House gave the pledge of allegiance to the flag of the United States of America. The Clerk pro tempore called the roll by legislative district in numerical order, and the following members-elect presented proof of their eligibility to be sworn in and seated as members of the House of Representatives: 1A ......................... Dan Fabian 10B ........................ Dale K. Lueck 1B .......................... Debra (Deb) Kiel 11A ....................... Mike Sundin 2A ......................... Matthew J. Grossell 11B ........................ Jason Rarick 2B .......................... Steve Green 12A ....................... Jeff Backer 3A ......................... Rob Ecklund 12B ........................ Paul Anderson 3B .......................... Mary Murphy 13A ....................... Jeff Howe 4A ......................... Ben Lien 13B ....................... -

ELECTION DIRECTORY for the 2021-2022 MINNESOTA LEGISLATURE
Preliminary 2020 ELECTION DIRECTORY for the 2021-2022 MINNESOTA LEGISLATURE Minnesota House of Representatives and Minnesota Senate Jan. 5, 2021 2021-2022 House Membership Statistics 70 DFL members 64 Republican members 51 members are women 83 members are men 13 Republican women 51 Republican men 38 DFL women 32 DFL men Newly elected members 23 newly elected members for 2021-22, includes two former members 12 newly elected DFL members 11 newly elected Republican members 17.2 percent of 2021-22 members did not serve last session 11 newly elected members are women 12 newly elected members are men 89 percent of incumbents on the ballot were re-elected 0 Republican incumbents lost 5 DFL incumbents lost 18 seats were open at the time of the election 4 races were uncontested (18A Dean Urdahl; 28A Gene Pelowski, Jr.; 49A Heather Edelson; 60B Mohamud Noor) New House DFL members Esther Agbaje ............................... 59B Emma Greenman ........................ 63B Kaela Berg ..................................... 56B Jessica Hanson .............................56A Liz Boldon .................................... 25B Athena Hollins ............................. 66B Sandra Feist .................................. 41B Heather Keeler ...............................4A Cedrick Frazier ............................45A Liz Reyer ....................................... 51B Luke Frederick ............................. 19B John Thompson ...........................67A New House Republican members Susan Akland ...............................19A Patricia -

Minnesota Legislative Scorecard Measuring Support for Education & Student Achievement in the 88Th Legislature
Minnesota legislative scorecard Measuring support for education & student achievement in the 88th Legislature A MINNCAN REPORT Minnesota legislative scorecard Measuring support for education & student achievement in the 88th Legislature This report was published in September MinnCAN: The Minnesota Campaign 2014 by MinnCAN: The Minnesota Campaign for Achievement Now for Achievement Now www.minncan.org To order copies of this report please contact Design & Layout MinnCAN: [email protected] house9design.ca A MINNCAN REPORT Table of contents Intro: Letter from Daniel Sellers 4 Education champions 6 Senate scorecard 7 House scorecard 13 Important policies 22 Disclamer This scorecard is for informational purposes only. When judging the qualifications of any candidate or incumbent, voters should consider matters such as performance on committees, constituent service, and positions on all matters in addition to those reflected on the scorecard. Introduction Dear friends, I am thrilled to release MinnCAN’s first legislative scorecard! In 2013 and 2014, during the 88th Legislature, we worked to find changing-the- odds public schools, share their stories at the Capitol and help their successes inform policy that will improve public schools across Minnesota. This scorecard showcases the tremendous progress we made to pass and implement such policies and to ensure that all kids have access to a great public school. During the 88th Legislature, our bipartisan allies: • invested nearly $45 million to help low-income 3- and 4-year-olds access quality pre-K • strengthened public charter school accountability • implemented well-rounded educator evaluations • made schools safer • allowed the state to recruit and retain the best teachers and leaders • increased college access, and more. -

2012 ELECTION DIRECTORY for the 2013-2014 MINNESOTA LEGISLATURE
2012 ELECTION DIRECTORY for the 2013-2014 MINNESOTA LEGISLATURE Minnesota House of Representatives and Minnesota Senate Jan. 31, 2013 2013-2014 House Membership Statistics Official list as of Jan. 9, 2013 72 DFL members 60 Republican members 88 members are men 44 members are women 44 DFL men 44 Republican men 28 DFL women 16 Republican women Newly elected members 42 newly elected members 27 newly elected DFL members 15 newly elected Republican members 31.3 percent of House members did not serve last session 31 newly elected members are men 11 newly elected members are women 91.1 percent of incumbents were re-elected 0 DFL incumbents lost 9 Republican incumbents lost 34 seats were open at the time of the election 3 House races were uncontested Reps. Steve Gottwalt (R-St. Cloud) and Terry Morrow (DFL-St. Peter) were elected to serve fourth terms; however, after accepting new employment, they chose not to be sworn in. Special elections to fill the two vacant House seats have been scheduled for Feb. 12. New House DFL members *Connie Bernardy .......................41A Jason Metsa..................................... 6B *David Bly .................................... 20B *Will Morgan ............................... 56B Raymond Dehn ............................ 59B *Jerry Newton ..............................37A Zachary Dorholt .......................... 14B Joe Radinovich ............................. 10B *Ron Erhardt ................................49A *Paul Rosenthal ............................ 49B Roger Erickson...............................2A -

Minnesota Charter Schools by Legislative District
Minnesota Charter Schools by Legislative District Senator Representative School 2 Paul Utke (R) 02B Steve Green (R) Naytahwaush Community School – Naytahwaush [email protected] [email protected] 3 Thomas (Tom) Bakk (DFL) 03A Rob Ecklund (DFL) Birch Grove Community School – Tofte http://www.senate.mn/senatorbakkemail [email protected] Great Expectations School - Grand Marais Vermillion Country School-Tower Oshki Ogimaag Charter School - Grand Portage 03B Mary Murphy (DFL) North Shore Community School – Duluth [email protected] Duluth Edison Charter School: North Star Academy - Duluth 5 Justin Eichorn (R) 05A Matt Bliss (R) Schoolcraft Learning Community – Bemidji [email protected] [email protected] TrekNorth High School - Bemidji Voyageurs Expeditionary High School - Bemidji 6 David J. Tomassoni (DFL) 06A Julie Sandstede (DFL) Northern Lights Community School – Warba [email protected] [email protected] 06B Jason Metsa (DFL) East Range Academy of Technology & Science (ERATS) - Eveleth [email protected] 7 Erik Simonson (DFL) 07B Liz Olson (DFL) Harbor City International School – Duluth [email protected] [email protected] Duluth Edison Charter School: Raleigh Academy - Duluth 9 Paul Gazelka (R) 09A John Poston (R) Pillager Area Charter School – Pillager [email protected] [email protected] 10 Carrie Ruud (R) 10A Joshua Heintzman (R) Discovery Woods Montessori School - Brainerd [email protected] [email protected] 10B Dale K. Lueck (R) Minisinaakwaang Leadership Academy - McGregor [email protected] Crosslake Community School - Crosslake 12 Torry Westrom (R) 12A Jeff Backer (R) Glacial Hills Elementary School - Starbuck [email protected] [email protected] 14 Jerry Relph 14A Tama Theis Athlos Academy of St. -

Governor Mark Dayton Chair Michelle Benson 130 State Capitol 3109 Minnesota Senate Bldg
Governor Mark Dayton Chair Michelle Benson 130 State Capitol 3109 Minnesota Senate Bldg. 75 Rev. Dr. Martin Luther King Jr. Blvd. 95 University Ave. W. St. Paul, MN 55155 St. Paul, MN 55155 Sen. Tony Lourey (Minority Lead) Chair Matt Dean 2211 Minnesota Senate Bldg. 401 State Office Building 95 University Ave. W. 100 Rev. Dr. Martin Luther King Jr. Blvd. St. Paul, MN 55155 St. Paul, MN 55155 Rep. Erin Murphy (Minority Lead) 331 State Office Building 100 Rev. Dr. Martin Luther King Jr. Blvd. St. Paul, MN 55155 June 8, 2018 Dear Governor Dayton and Chairs Benson and Dean and Minority Leads Lourey and Murphy for the Health and Human Services Finance Committees: We are writing to express our serious concerns regarding several time-sensitive legislative requests left unresolved by the 2018 session. We believe there is significant, unfinished work that state lawmakers must address before the 2019 legislative session to protect the state budget, ensure continued access to care for some of Minnesota’s most vulnerable residents, and avoid unnecessary risk to our Medicaid program. Ensuring state agencies with programs, like Medicaid, are able to comply with federal law is a core component of state governance. From time to time, this requires approving necessary state investments and statutory changes to authorize state agencies to implement the ever-changing rules and regulations surrounding these programs and their funding streams. During the 2018 session, there were several proposals aimed at federal compliance for the state’s Medicaid program. Overall, they received strong bipartisan support, even though some of them did not come to light until late in the session. -

2012 Election Analysis Revenge of the Amendments
2012 Election Analysis Revenge of the Amendments Steve Peterson Top of the Ticket in MN The Talking Heads The Other Winner Nate Silver & Math! Popular Vote Nate Silver & Math! • Electoral College Nate Silver & Math! • Chance to Win Amy! Amy! Amy! MN State Legislature • 11 DFL House seats – 5 Greater MN – 6 Metro • 9 DFL Senate Seats – 3 Greater – 6 Metro Turnout, Turnout, Turnout Voter Excitement? VOTE NO SD w/Higher No Votes, Higher Overall Turnout Yes Voters – No Increase in Turnout Suburban Turnout Driven by No Vote Greater MN Turnout Not Driven by Vote Yes Marriage Amendment Senate Metro Map Photo ID’s Surprise Defeat Survey USA Polling Photo ID Resistance Increased 50+ and Greater MN Huge DFL Vote Increase in Senate Senate Swap Senate History 2010 Senate Margin of Victory 2012 Senate Margin of Victory Metro Senate Map 2010 vs. 2012 Senate Map 2010 vs. 2012 Fewer Greater MN Seats GOP Senate Majority Caucus 2011 DFL Senate Majority Caucus 2013 Senate Leadership and Key Chairs • Majority Leader - Tom Bakk • Assistant Majority Leader – Katie Sebien • President – Sandra Pappas • Tax Chair – Rod Skoe • Finance Chair – Richard Cohen • Cap. Investment – LeRoy Stumpf (likely) GOP Senate Minority Caucus 2013 Minority Leadership • Minority Leader – David Hann • Asst. Minority Leader – Michelle Benson • Asst. Minority Leader – Roger Chamberlain • Asst. Minority Leader – Warren Limmer • Asst. Minority Leader – Dave Thompson Greater Minnesota Senate Delegation 2013 Large DFL Vote Increase House Swap House Party History 2010 House Margin of Victory 2012 House Margin of Victory GOP House Majority Caucus 2011 DFL House Majority Caucus 2013 House Leadership • Speaker - Paul Thissen • Majority Leader – Erin Murphy • Key Chairs? – Taxes – Ann Lenczewski – Cap.