A Case Study of Ramban District)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

English June.Indd
In this Issue... • Saving the Hangul • Cricket stadium in Srinagar being upgraded • Mongolia keen to tap potential of Leh Berry plant • Kani shawl gets Geographical Indication (GI) tag • Reaching out • Sufi shrine, a symbol of Kashmiriyat • Tourists beat the heat in Patnitop • Leh hosts a ʻGreenʼ Rally • A Kashmir success story Vol. 1, No. 10, July 2010 Saving the Hangul Hangul, the state animal of Jammu and Kashmir, is the only survivor of the Red Deer group in the Indian subcontinent and, its population has been declining over the years due to habitat destruction, overgrazing by domestic livestock and poaching. Alarmed by the fall in numbers of this rare red deer, known scientifically as Cervus Elaphus Hanglu, and locally known as “Hangul”, the Government of Jammu and Kashmir is doing everything possible to save it from extinction. Battling for its survival, the Hangul are now scattered within the Dachigam National Park, which is located under the Zabarwan mountain range on the outskirts of Srinagar. The Dachigam National Park is the natural habitat of the Hangul, though in the summers, some of them cross the boundaries of the national park to graze in the higher mountain reaches. The state government has prepared a plan for Hangul conservation with the help of the Dehradun-based Wildlife Institute of India at a cost of Rs.220 million. The five-year plan has been submitted to the Union Ministry of Environment and Forests for approval. As part of the plan, the state government will buy field equipment, satellite images, GIS hardware and software. It would also build carnivore-proof enclosures, guard huts, watch towers and take steps to stop poachers. -

Compendium-2019
INDEX S. Subject Reference to Reference to Page No. Notification/SRO/ Rule No. Govt. Order/ Circular/OM etc. 1 2 3 4 5 1. Clarification regarding O. M. No. A/ 1 exercise of option Clar(2018)-II-1110 under rule 5 of Dated 02-01-2019. SRO-193 of 2018 dated 24-04-2018. 2. Family Pension case in No. A/41(2009)-C-840 2 respect of Divorced Dated 02-01-2019. daughters. 3. Adoption case of Late No. A/33(2015)-811 3 Mohd Yousuf ex- Dated 03-01-2019. welder/authorization of family pension. 4. Advisory for strict Circular No. A/ 4-5 adherence to rules, 35(2017)-1123 regulation or orders Dated 03-01-2019. governing the receipt of money, its custody and payment by the Government servant. 5. In-situ promotion(s) No. A/31(97)-488 6 subsequent to Dated 07-01-2019. foregoing functional promotion-clari- fication thereof. 6. Amendment in the SRO-22 7 J&K Financial Code dated 10-01-2019. Vol. I. ( ii ) 1 2 3 4 5 7. Date of next O. M. No. A/PS/DGC/ 8 increment-Rule 10 of Gen/2018-1268 J&K Civil Service Dated 16-01-2019. (Revised) Pay Rules, 2018-classification thereof . 8. Grant of hardship Government Order 9 allowance on Revised 22-F of 2019 Dated Pay Scales in favour 16-01-2019. of Police Personnel. 9. Payment of arrears of Government Order 10 interim Relief to the No. 48-F of 2019 members of Jammu dated 22-01-2019. and Kashmir Subordinate Judicial Services/Pensioners/ Family Pensioners. -
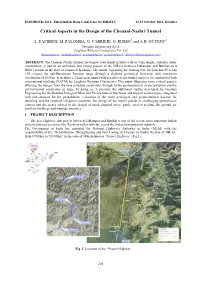
Critical Aspects in the Design of the Chenani-Nashri Tunnel
INDOROCK 2011: Third Indian Rock Conference by ISRMTT 13-15 October 2011, Roorkee Critical Aspects in the Design of the Chenani-Nashri Tunnel L. FACIBENI, M. PALOMBA, G. CARRIERI, G. RUSSO1 and A.H. GÜVENC2 1Geodata Engineering S.p.A. 2Leighton Welspun Contractors Pvt. Ltd. ([email protected]; [email protected]; [email protected]; [email protected]; [email protected]) ABSTRACT: The Chenani-Nashri Tunnel, the longest road tunnel in India with its 9 km length, currently under construction, is part of an ambitious four laning project of the NH-1A between Udhampur and Banihal on a DBFO pattern in the state of Jammu & Kashmir. The tunnel, bypassing the existing NH-1A from km 89 to km 130, crosses the sub-Himalayan Patnitop range through a flyshoid geological formation with maximum overburden of 1050 m. It includes a 2-lane main tunnel with parallel escape tunnel and is to be constructed with conventional methods (NATM) by Leighton Welspun Contractors. This paper illustrates some critical aspects affecting the design, from the time schedule constraints, through to the geomechanical characterization and the environmental constraints at large. In doing so, it presents the additional studies developed by Geodata Engineering for the Detailed Design of Main and Escape tunnels functional and support section types, integrated with risk analysis for the probabilistic evaluation of the main geological and geomechanical hazards for tunneling and the required mitigation measures, the design of the tunnel portals in challenging geotechnical context and the issues related to the design of muck disposal areas, partly used to reclaim flat ground for ancillary buildings and wayside amenities. -

B.A. 6Th Semester Unit IV Geography of Jammu and Kashmir
B.A. 6th Semester Unit IV Geography of Jammu and Kashmir Introduction The state of Jammu and Kashmir constitutes northern most extremity of India and is situated between 32o 17′ to 36o 58′ north latitude and 37o 26′ to 80o 30′ east longitude. It falls in the great northwestern complex of the Himalayan Ranges with marked relief variation, snow- capped summits, antecedent drainage, complex geological structure and rich temperate flora and fauna. The state is 640 km in length from north to south and 480 km from east to west. It consists of the territories of Jammu, Kashmir, Ladakh and Gilgit and is divided among three Asian sovereign states of India, Pakistan and China. The total area of the State is 222,236 km2 comprising 6.93 per cent of the total area of the Indian territory including 78,114 km2 under the occupation of Pakistan and 42,685 km2 under China. The cultural landscape of the state represents a zone of convergence and diffusion of mainly three religio-cultural realms namely Muslims, Hindus and Buddhists. The population of Hindus is predominant in Jammu division, Muslims are in majority in Kashmir division while Buddhists are in majority in Ladakh division. Jammu is the winter capital while Srinagar is the summer capital of the state for a period of six months each. The state constitutes 6.76 percent share of India's total geographical area and 41.83 per cent share of Indian Himalayan Region (Nandy, et al. 2001). It ranks 6th in area and 17th in population among states and union territories of India while it is the most populated state of Indian Himalayan Region constituting 25.33 per cent of its total population. -

NW-49 Final FSR Jhelum Report
FEASIBILITY REPORT ON DETAILED HYDROGRAPHIC SURVEY IN JHELUM RIVER (110.27 KM) FROM WULAR LAKE TO DANGPORA VILLAGE (REGION-I, NW- 49) Submitted To INLAND WATERWAYS AUTHORITY OF INDIA A-13, Sector-1, NOIDA DIST-Gautam Buddha Nagar UTTAR PRADESH PIN- 201 301(UP) Email: [email protected] Web: www.iwai.nic.in Submitted By TOJO VIKAS INTERNATIONAL PVT LTD Plot No.4, 1st Floor, Mehrauli Road New Delhi-110074, Tel: +91-11-46739200/217 Fax: +91-11-26852633 Email: [email protected] Web: www.tojovikas.com VOLUME – I MAIN REPORT First Survey: 9 Jan to 5 May 2017 Revised Survey: 2 Dec 2017 to 25 Dec 2017 ACKNOWLEDGEMENT Tojo Vikas International Pvt. Ltd. (TVIPL) express their gratitude to Mrs. Nutan Guha Biswas, IAS, Chairperson, for sparing their valuable time and guidance for completing this Project of "Detailed Hydrographic Survey in Ravi River." We would also like to thanks Shri Pravir Pandey, Vice-Chairman (IA&AS), Shri Alok Ranjan, Member (Finance) and Shri S.K.Gangwar, Member (Technical). TVIPL would also like to thank Irrigation & Flood control Department of Srinagar for providing the data utilised in this report. TVIPL wishes to express their gratitude to Shri S.V.K. Reddy Chief Engineer-I, Cdr. P.K. Srivastava, Ex-Hydrographic Chief, IWAI for his guidance and inspiration for this project. We would also like to thank Shri Rajiv Singhal, A.H.S. for invaluable support and suggestions provided throughout the survey period. TVIPL is pleased to place on record their sincere thanks to other staff and officers of IWAI for their excellent support and co-operation through out the survey period. -

District Disaster Management Plan Ramban 2020-21
Government of Jammu and Kashmir District Development Commissioner Ramban DISTRICT DISASTER MANAGEMENT PLAN RAMBAN 2020-21 © DDMA, Ramban Edition: First, 2019 Edition: Second 2020 Authors: Drafted By : Feyaiz Ahmed (Junior Assistant) Edited By: Nazim Zai Khan (KAS), Deputy Commissioner Ramban Published by: District Disaster Management Authority – Ramban Jammu & Kashmir, 182144 Preparation: This document has been prepared purely on the basis of information obtained from different authentic sources and the information received from concerned departments in the District. Disclaimer: This document may be freely reviewed, reproduced or translated, in part or whole, purely on non-profit basis for any non-commercial purpose aimed at training or education promotion as cause for disaster risk management and emergency response. The Authors welcome suggestions on its use in actual situations for improved future editions. The document can be downloaded from http://www.ramban.gov.in. For further queries and questions related to this Document please contact at: Email: [email protected] Phone: +91-1998-266789: Fax: +91-1998-266906 Main Source: - J&K State Disaster Management Plan & National Disaster Management Plan Page 2 of 76 MESSAGE I am happy to present the Disaster Management Plan for District Ramban (Jammu & Kashmir). The aim of the plan is to make Ramban a safe, adaptive and disaster-resilient District. It will help to maximise the ability of stakeholders to cope with disasters at all levels by integrating Disaster Risk Reduction (DRR) & Climate Change Adaptation (CCA) into developmental activities and by increasing the preparedness to respond to all kinds of disasters. This plan takes into account the trends that have been mentioned in J&K Disaster Management Policy and State Disaster Management Plan. -

Pir Panjal Regional Festival Integrating the Isolated Border Districts in J&K & Building Peace from Below*
No 142 IPCS ISSUE BRIEF No 142 APRIL 2010 APRIL 2010 Building Peace & Countering Radicalization Pir Panjal Regional Festival Integrating the Isolated Border Districts in J&K & Building Peace from Below* D. Suba Chandran Deputy Director, IPCS, New Delhi This essay focus on two districts in the Jammu sub region of J&K—Rajouri and Poonch, along the Pir Panjal range of the outer Himalayas. The primary objective is to highlight the conflict transformation (both positive and negative) in this region during the recent years; to explore the opportunities of an Pir Panjal festival bringing the various communities together and build peace from below; integrate the border districts with the national mainstream; and improve the physical and psychological connectivity of the Pir Panjal region with the rest and remove the feeling of physical isolation. Idea of using a festival to promote tourism in J&K is not a new one; those who have witnessed the Ladakh festival, in all its colorful glory and culturally rich historical past, would agree how it has brought the region, its people and culture to the limelight. Of course, there are other places – from Dal lake to Gulmarg and from Bhaderwah to Basohli, which can easily boast the same – in terms of their rich culture, colorful people and beautiful places. The irony of J&K, however has been - there are numerous such regions in J&K, unfortunately remaining in the periphery, physically isolated and psychologically looking inward. Ladakh festival, now celebrated during August every year, attracts global attention and tourists who visit the land of moon, as it is popularly referred, to enjoy the culture, people and places. -
Abdul Rashid NT, Mohd. Aslam Vijay Kumar
I I & Government of Jammu & Kashmir Office of the Financial Commissioner (Revenue) J&K, Jammu. Subject: Transfer/posting of Naib Tehsildars, llc Naib Tehsildars, LIA Naib Tehsildars. oRDER NO FC(A) lo ot 2019 Dated. 03 . 01 2019 ln the interest of administration, the following transfers/postings of Naib Tehsildars llc Naib Tehsildars, L/A Naib Tehsildars are hereby made with immediate effect.- S. Name of the Under orders trdnSfer New place of posting. No Official. to/ present place of S/Shri posting 1. Mohd. Shafi Sofi ll3 NT Tangmarg ll? NT Diyalgam, District District Kulgam Anantnag against available vacancy. 2. Abdul Rashid NT, Pahalgam NT Collector Defence Bhat Anantnag Budgam against available vacancy. 3. Mohd. Aslam LA NT Nowshera Distt. NT Panzgam, Kupwara Khatana Baramulla against available vacancy. 4. Gh. Nabi Ganaie LA NT Khayar Distt. NT Ashpora Kupwara Baramulla against available vacancy. 5. Mohd. Ashraf Niabat Bounjwah ARA to DC, Doda. Kishtwar 6. Mohd. Rasheed LA NT Karool Distt. LA NT Gulpur District Kishtwar Poonch against available vacancy. 7. Vijay Kumar LA NT Gool District Retained in the office of Gupta Ramban DC, Udhampur. 8. Manzoor Ahmad llc NT Lammar Blanil Retained at Achabal Choda Kulgam Anantnag (due to health grounds) 9. Gh. Mohammad un-adjusted llc NT Tangmarg District Itoo Kulgam vice Shri Mohd. Shafi Sofi (S.No.1) 10. Mohd. Sharief LA NT Hari Marhote LA NT Kainthi District Distt. Poonch Reasi against available vacancy. 11, Mohd, lsmail LA NT Ramban District LA NT Mansar Tehsil Ramban. Majhalta Distt. UdhamPur against available vacancY. 12. Mohd. lqbal Mir NT Hajan Distt. -

RAMBAN © DDMA, Ramban Edition: First, 2019 Authors: -Parvaiz Naik, (KAS), Tehsildar HQA Ramban Drafted & Assist By: Feyaiz Ahmed (Junior Assistant)
Page 1 of 75 DISTRICT DISASTER MANAGEMENT PLAN RAMBAN © DDMA, Ramban Edition: First, 2019 Authors: -Parvaiz Naik, (KAS), Tehsildar HQA Ramban Drafted & Assist by: Feyaiz Ahmed (Junior Assistant) Published by: District Disaster Management Authority – Ramban Jammu & Kashmir, 182144 Preparation: This document has been prepared purely on the basis of information obtained from different authentic sources and the information received from concerned departments in the District. Disclaimer: This document may be freely reviewed, reproduced or translated, in part or whole, purely on non-profit basis for any non-commercial purpose aimed at training or education promotion as cause for disaster risk management and emergency response. Authors welcome suggestions on its use in actual situations for improved future editions. The document can be downloaded from http://www.ramban.gov.in. Email: [email protected]: Phone No. 01998-266789: FAX No. 01998-266906 Main Source: - J&K State Disaster Management Plan & National Disaster Management Plan Page 2 of 75 Page 3 of 75 Deputy Commissioner Ramban MESSAGE I am happy to present the Disaster Management Plan for District Ramban (Jammu & Kashmir). The aim of the plan is to make Ramban a safe, adaptive and disaster-resilient District. It will help to maximize the ability of stakeholders to cope with disasters at all levels by integrating Disaster Risk Reduction (DRR) & Climate Change Adaptation (CCA) into developmental activities and by increasing the preparedness to respond to all kinds of disasters. This plan takes into account the trends that have been mentioned in J&K State Disaster Management Policy and State Disaster Management Plan. Implementation of the plan requires sincere cooperation from all the stakeholders especially the active participation of civil society, community based organizations and Government. -

Jammu & Kashmir Reorganisation Act 2019
jftLVªh lañ Mhñ ,yñ—(,u)04@0007@2003—19 REGISTERED NO. DL—(N)04/0007/2003—19 vlk/kkj.k EXTRAORDINARY Hkkx II — [k.M 1 PART II — Section 1 izkf/kdkj ls izdkf'kr PUBLISHED BY AUTHORITY lañ 53] ubZ fnYyh] 'kqØokj] vxLr 9] [email protected] 18] 1941 ¼'kd½ No. 53] NEW DELHI, FRIDAY, AUGUST 9, 2019/SHRAVANA 18, 1941 (SAKA) bl Hkkx esa fHkUu i`"B la[;k nh tkrh gS ftlls fd ;g vyx ladyu ds :i esa j[kk tk ldsA Separate paging is given to this Part in order that it may be filed as a separate compilation. MINISTRY OF LAW AND JUSTICE (Legislative Department) New Delhi, the 9th August, 2019/Shravana 18, 1941 (Saka) The following Act of Parliament received the assent of the President on the 9th August, 2019, and is hereby published for general information:— THE JAMMU AND KASHMIR REORGANISATION ACT, 2019 NO. 34 OF 2019 [9th August, 2019.] An Act to provide for the reorganisation of the existing State of Jammu and Kashmir and for matters connected therewith or incidental thereto. BE it enacted by Parliament in the Seventieth Year of the Republic of India as follows:— PART-I PRELIMINARY 1. This Act may be called the Jammu and Kashmir Reorganisation Act, 2019. Short title. 2. In this Act, unless the context otherwise requires,— Definitions. (a) “appointed day” means the day which the Central Government may, by notification in the Official Gazette, appoint; (b) “article” means an article of the Constitution; (c) “assembly constituency” and “parliamentary constituency” have the same 43 of 1950. -
Provisional List of Candidates Who Have Applied for Admission to 2
Provisional List of candidates who have applied for admission to 2-Year B.Ed.Programme session-2020 offered through Directorate of Distance Education, University of Kashmir. Any candidate having discrepancy in his/her particulars can approach the Directorate of Admissions & Competitive Examinations, University of Kashmir alongwith the documentary proof by or before 31-07-2021, after that no claim whatsoever shall be considered. However, those of the candidates who have mentioned their Qualifying Examination as Masters only are directed to submit the details of the Graduation by approaching personally alongwith all the relevant documnts to the Directorate of Admission and Competitive Examinaitons, University of Kashmir or email to [email protected] by or before 31-07-2021 Sr. Roll No. Name Parentage Address District Cat. Graduation MM MO %age MASTERS MM MO %age SHARIQ RAUOF 1 20610004 AHMAD MALIK ABDUL AHAD MALIK QASBA KHULL KULGAM RBA BSC 10 6.08 60.80 VPO HOTTAR TEHSILE BILLAWAR DISTRICT 2 20610005 SAHIL SINGH BISHAN SINGH KATHUA KATHUA RBA BSC 3600 2119 58.86 BAGHDAD COLONY, TANZEELA DAWOOD BRIDGE, 3 20610006 RASSOL GH RASSOL LONE KHANYAR, SRINAGAR SRINAGAR OM BCOMHONS 2400 1567 65.29 KHAWAJA BAGH 4 20610008 ISHRAT FAROOQ FAROOQ AHMAD DAR BARAMULLA BARAMULLA OM BSC 1800 912 50.67 MOHAMMAD SHAFI 5 20610009 ARJUMAND JOHN WANI PANDACH GANDERBAL GANDERBAL OM BSC 1800 899 49.94 MASTERS 700 581 83.00 SHAKAR CHINTAN 6 20610010 KHADIM HUSSAIN MOHD MUSSA KARGIL KARGIL ST BSC 1650 939 56.91 7 20610011 TSERING DISKIT TSERING MORUP -

Ground Response and Support Measures for Pir Panjal Tunnel in the Himalayas
GroundIGC 2009 Response, Guntur, and INDIA Support Measures for Pir Panjal Tunnel in the Himalayas GROUND RESPONSE AND SUPPORT MEASURES FOR PIR PANJAL TUNNEL IN THE HIMALAYAS K.S. Rao Professor, Department of Civil Engineering, Indian Institute of Technology Delhi, Hauz Khas, New Delhi–110 016, India. E-mail: [email protected] ABSTRACT: The Pir Panjal tunnel linking between Banihal and Qazigund stations is the important tunnel in the railway line from Udhampur to Baramula in the Himalayas. The Pir Panjal ranges are having complex geological set up with major folds and faults. More than six major lithological units are traled along the 11 km length of the tunnel with very high overburden at many sections. The phenomena of squeezing is studied using the limit equilibrium and FLAC methods for this tunnel. A detailed stress and displacement assessment has been attempted in this study, in order to stabilise the tunnel sections with suitable support measures. 1. INTRODUCTION Sequence of rock mass behaviour leading to regional failure is explained schematically by Szwedzicki (2003) as shown in A large number of power and transport tunnel projects are being Figure 1. Accordingly, there will be several indicators and constructed in the tectonically active and young Himalayan precursors which will lead to local damage and subsequently mountains. The main areas of concern regarding tunnel stability regional failure. An indicator is defined as a sign, a state or a are the existence of weak, highly deformable and anisotropic contributing factor that points out or suggest that the rock rock mass and high degree of weathering and fracturing.