Table of Contents Background
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Page10sportfgs.Qxd (Page 1)
MONDAY, MAY 3, 2021 (PAGE 10) DAILY EXCELSIOR, JAMMU Buttler blitzkrieg powers Royals Webinar on 'Teaching of Guru Tegh Bahadur' organised to 55-run victory over SRH Excelsior Correspondent temporary times when the world is NEW DELHI, May 2: Chris Morris (3/29) and ous Jonny Bairstow (30) and Vijay grappling with the pandemic as Mustafizur Rahman (3/20) did the Shankar (8) soon followed. JAMMU, May 2: Department they fortify our faith in human Jos Buttler announced his bulk of the work with the ball With the pressure mounting, of Dean Students Welfare of nature and their problems. return to form with belligerent while Kartik Tyagi (1/32) Rahul skipper Kane Williamson (20) Cluster University of Jammu today The programme commenced maiden T20 hundred as Rajasthan Twetia (1/45) picked a wicket went for the big shot only to be organised webinar on the life and with a prayer video imploring for Royals made a mincemeat of an apiece. caught at deep midwicket by teachings of Guru Tegh Bahadur, hope and cure of millions of fellow out-of-sorts Sun Risers Hyderabad, With the win, the Royals Morris off Tyagi as wickets tum- the 9th Guru of Sikh community. Indians falling prey to the deadly winning Sunday's IPL encounter moved up to fifth spot while SRH bled at regular intervals. The webinar was organised as pandemic, followed by a one by a whopping 55-run margin. continued to stay at the bottom, Mohammad Nabi (17 off 5) part of Azaadi Ka Amrut Mahotsav. minute silence to pay homage to all Opening the innings, Buttler having won only one match all sea- injected some hope in the SRH The objective of the lecture was to the departed souls who fell victim smashed a breathtaking 124 off 64 son. -

Page10finals.Qxd (Page 1)
TUESDAY, JULY 2, 2019 (PAGE 10) DAILY EXCELSIOR, JAMMU Fernando trumps Pooran in Sri Lanka’s Vijay Shankar out of World Cup with toe injury, 'Bangla Test': Changes on cards as Mayank Agarwal named replacement 23-run win over West Indies BIRMINGHAM, July 1: Council has confirmed that the no end to India's middle-order woes CHESTER-LE-STREET, July 1: Indian all-rounder Vijay Event Technical Committee of the BIRMINGHAM, July 1: ing Ravindra Jadeja's case for in the playing XI against Shankar was Monday ruled out of ICC Men's Cricket World Cup inclusion stronger by the day. Bangladesh, it will definitely Nicholas Pooran's sensa- the ongoing World Cup due to a toe 2019 has approved Mayank Kedar Jadhav and Yuzvendra The primary logic could possi- bolster the lower-order bat- tional century went in vain as injury and will be replaced by bats- Agarwal as a replacement player Chahal could find their names bly be Jadeja being better at big- ting. Avishka Fernando set up Sri man Mayank Agarwal, who is yet for Vijay Shankar in the India struck off the final XI as India aim hitting compared to Jadhav, when For India, the important thing Lanka's thrilling 23-run win to make his ODI debut. squad for the remainder of the tour- for a quick turnaround in their batting at Nos.6 or 7. His wicket- will be that Bangladesh's bowling over West Indies with a maid- Shankar is the second Indian nament," said the ICC in a release. penultimate World Cup group to-wicket left-arm spin is a restric- won't have the same potency as en hundred in an inconsequen- player to be ruled out of the tourna- Karnataka opener Agarwal, league game against a battle-hard- tive option and to top it all, his out- England and they will heavily tial World Cup match here ment after senior opener Shikhar who made his Test debut against ened Bangladesh, which is trying standing ability to field at any depend on Shakib's all-round to stay relevant in a fight for the position. -

RR Vs KXIP, 4Th Match, IPL 2019 Highlights | Chris Gayle Inning & Ashwin Cleverness Snatched the Match from Rajasthan Royals
RR vs KXIP, 4th match, IPL 2019 highlights | Chris Gayle inning & Ashwin cleverness snatched the match from Rajasthan Royals Kings XI Punjab registered their first win in Jaipur against Rajasthan Royals in IPL history. The 4th match of IPL 12 belongs to Chris Gayle and Jos Buttler inning but the controversial run out of Jos Buttler by Ravi Ashwin was the focus point after the match. Let’s read out the complete details of RR vs KXIP 4th match IPL 2019 here. Earlier Rajasthan Royals won the toss and opted to bowl first against Kings XI Punjab. Chris Gayle smashed 79 runs in 47 balls and awarded as Man of The Match. IPL 2019 Match 4 Analysis : RR vs KXIP, 4th Match Toss : Rajasthan Royals won the toss and opted to bowl first. Man of the Match : Chris Gayle Match Number : 4 Kings XI Punjab opening duo Chris Gayle and Lokesh Rahul started the inning but KL Rahul got out in first over by making 4 runs only. New batsman Mayank Agarwal comes to the crease and build 50 plus partnership with Chris Gayle and got out by making 22 runs. Initially Chris Gayle was not in good touch as he made 27 runs of 25 balls but once he settled at the crease the next 50 runs he scored in only 17 balls and before getting out made 79 runs in 47 balls. Sarfaraz Khan also contributed with 46 runs in 29 balls to ensure the KXIP inning with a competitive total. Rajasthan Royals openers were in no mood to settle the KXIP bowlers in the batting powerplay and their opener captain Ajinkya Rahane and Jos Buttler build 78 runs opening partnership. -

Page 8 Sports & Single).Qxd
MONDAY, SEPTEMBER 28, 2020 (PAGE 10) DAILY EXCELSIOR, JAMMU Sensational Tewatia hits five sixes in an over to MISCELLANEOUS PLACEMENT SUNRISE INSTITUTE GANDHI NAGAR Required female hardworking & talented Staff (1) Work from home 10 candidates take RR to incredible win over KXIP Salary 6-8 thousand Monthly (2) Counsellor - 5 Candidates SHARJAH, Sept 27: over. Salary 8-10 thousand monthly (3) Supervisor - Salary 10-12 thousand monthly Earlier, opener Mayank (4) Also Required 20 Male & female candidates for Rahul Tewatia struck five sixes Agarwal outshone his captain Marketing Salary 20 thousand and monthly + Incentives in an over at the fag end of the Rahul with a maiden IPL hundred Venue : 119-A/D Green Belt Park Gandhi Nagar match as Rajasthan Royals record- as the duo pummelled the Royals C&W 7006749002 ed the highest runchase in IPL his- bowlers into submission to post Professionals and fresher can also apply tory, beating Kings XI Punjab by the highest total of this season so four wickets in a high-scoring far. GANPATI WATER STAFF REQUIRED encounter here today. Agarwal and Rahul's 183-run Winning team posing for a group photograph with dignitaries Trained graduates/ posts graduates required for Chasing a stiff 224 for a win, stand for the opening stand was the at Khel Gaon Nagrota on Sunday. TANK CLEANING teaching English, Social Science and Maths in Primary, Middle and High classes on contractual the Royals needed 51 runs from highest partnership for any wicket * Under ground tanks basis. Proficiency in English is must. the last three overs and it seemed so far this season as they took apart Zone Jammu lifts U-19 Cricket title Apply personally along with testimonials within a Over Head Tanks week time. -

New Zealand Vs India 2020
Published 28.1.20 Dream start to multi-format tour for India; younger players take centre-stage Two convincing wins achieved on the same pitch that behaved completely differently in the two matches in Eden Park have given India a vice-like grip over New Zealand in the Twenty20 International series. This dream start to the multi-format tour is indicative of the mindset and fighting spirit of this Indian team. I was impressed by what Virat said leading into the series – that despite a hard-fought three-match ODI series against Australia, the long flight to Auckland, the short turnaround time and entirely different conditions, his side wasn’t going to be looking for excuses, that they would be switched on from ball one of the first T20I. That speaks to the attitude of the unit as a whole, and it manifested itself in the brand of cricket they played over the weekend. The first game called for a furious assault on a target of 204, the second needed a more pragmatic approach after New Zealand were restricted to 132. India were clinical in both encounters, the same set of batsmen delivering the goods. It wasn’t the usual match-winners who came up trumps. Instead, and heart-warmingly with the larger picture in mind, KL Rahul and ShreyasIyer reinforced their coming of age at this level, taking up the responsibility of piloting the side home. Rahul’s talent has never been in doubt since he broke through towards the end of 2014. He seemed to have lost his way a- bit but in the last few months, since being dropped from the Test team, he has gone back and - had a hard look at himself, and has returned stronger, more organised and in control of his plans. -

Gambling Licence in India
Gambling Licence In India Busted Dory always rappelled his epanalepsis if Augustin is dipteral or confusing below. Limnological and indeciduate Amory often foul-ups some glomerations withershins or selles saprophytically. Decrescent Filmore ranging her township so monstrously that Arnoldo scurry very unthinkably. If you are keen, you can find details about the company and look up online to see their registered status, registration country, their directors and other details. Therefore, online betting is clearly a game of skill, and as such, is considered legal in many Indian states. The prohibition on gaming sites for yourself playing rummy companies but most. When it also have exhausted their gambling licence in india has not ever recieved any. In the case of betting on casino games, please refer above. How do I make money on online betting? Therefore would be best operators offering of licence in? There are only charge small are of States in India that allow operators to conduct gambling activities under a licensing regime. Each option to licence in gambling india is a screenwriter based on which is dismissed. If the betting is on games of chance, this is prohibited in most Indian States. The prize is to you everything we have obviously made by studying laws, especially when online. It gambling licences from this licence regime for you try again and municipal tax. An enforcement from trusted by a full access casino, subject to change if you consider whether a time. The licence will list of skill and games act is? It very common practice and horse racing and innovative betting on this casino will not revised in most popular online gambling platforms are prohibited from online. -
Match Report
Match Report Kings XI Punjab, KXIP vs Delhi Daredevils, DD Delhi Daredevils, DD - Won by 9 wickets Date: Fri 01 May 2015 Location: India - National Capital Territory of Delhi Match Type: Twenty20 Scorer: johnykutty philip Toss: Delhi Daredevils, DD won the toss and elected to Bowl URL: http://www.crichq.com/matches/249243 Kings XI Punjab, KXIP Delhi Daredevils, DD Score 118-8 Score 119-1 Overs 20.0 Overs 13.5 V Sehwag MA Agarwal M Vohra SS Iyer SE Marsh JP Duminy WP Saha† Yuvraj Singh DA Miller AD Mathews GJ Bailey KM Jadhav† NLTC Perera Z Khan AR Patel NM Coulter-Nile SN Thakur A Mishra Anureet Singh SS Tiwary Sandeep Sharma Imran Tahir page 1 of 34 Scorecards 1st Innings | Batting: Kings XI Punjab, KXIP R B 4's 6's SR V Sehwag 1 . // c AD Mathews b Z Khan 1 2 0 0 50.0 M Vohra . 1 . // c KM Jadhav† b Z Khan 1 7 0 0 14.29 SE Marsh 4 . 1 . // lbw b JP Duminy 5 4 1 0 125.0 WP Saha† 1 1 . 1 . // c KM Jadhav† b NM Coulter-Nile 3 8 0 0 37.5 DA Miller . 1 . 1 4 . 1 1 2 1 1 . 1 1 1 . 1 . 1 4 1 4 . 6 4 . 1 . 1 1 c SS Tiwary b NM Coulter-Nile 42 41 4 1 102.44 1 1 1 . // GJ Bailey . 1 4 . 1 . 4 . 1 4 1 1 1 . // lbw b A Mishra 18 16 3 0 112.5 NLTC Perera . -

SPORT 07 We Want to Write a Few Proper Things on the Pages of That Season Book
TUESDAY 9 APRIL 2019 SPORT 07 We want to write a few proper things on the pages of that season book. We are on fire to be CRICKET FOOTBALL Jurgen Klopp, says honest, you can see it in training, Indian Premier League Champions League Liverpool ‘on fire’ as but other teams as well. We all Chennai Super Kings vs Liverpool vs FC Porto they chase double. play for a lot. ACTION Kolkata Knight Riders Tottenham vs Man City TODAY’S Blackhawks Warriors clinch top seed in West; take optimistic tone after another lost Rockets set record for threes season in NHL AFP LOS ANGELES Golden State Warriors guard AP Stephen Curry (30) celebrates CHICAGO The Golden State Warriors after making a three-point clinched the Western Confer- basket against the LA Clippers Let me just say that Patrick Kane dazzled once ence’s top seed with a victory in during the first quarter of their for 47 years, Warriors again. Jonathan Toews put their final regular-season contest NBA game at Oracle Arena on fans have stuck with together one of his best seasons, at the Oracle Arena, beating the Sunday. and Alex DeBrincat took Los Angeles Clippers 131-104 on us through thick and another step forward. Sunday. thin. Let’s be honest, And it didn’t matter all that Stephen Curry led the charge most of those years much. Not to them, anyway. with 27 points and Kevin Durant have been a little The Chicago Blackhawks added 16 as the Warriors won missed out on the playoffs for their fifth straight game. -

PGP Final Placement Brochure 2015-17
Post Graduate Programme in Management (PGP) 2015-2017 Placements POST GRADUATE PROGRAMME IN MANAGEMENT (PGP) 2015-2017 Recruitment Process at IIM Bangalore Pre-Placement Talks (PPTs) The recruitment process at the Institute is coordinated by PPTs provide an opportunity to students and companies to Career Development Services (CDS) office along with a interact and exchange information. A PPT is typically of 45 Student Placement Committee. The Institute provides all minutes duration during which company representatives talk support in terms of infrastructure and facilities needed for the about their organization and the employment opportunities recruitment process. Recruitments at IIM Bangalore take place being offered. The students use this time to assess the in two phases organization and opportunities. A Q&A session also forms part • The Lateral Placement Process addresses the increasing of the PPT. need of corporates for students with work experience. Students Applications This process is limited to candidates who have at least 22 months of work experience. Based on the company presentation and their individual interest levels, students apply to companies. These can be • The Final Placement Process is open to all eligible on company application forms or resumes as per company students. requirements. The applications are forwarded to the company within a specified time frame. The companies are provided sufficient time to evaluate the applications and shortlist suitable candidates. Shortlists Student Career Support Fee Companies are required to send shortlists to the CDS Office at Applicable to all job offers accepted by students including least one week prior to the commencement of final placement Pre-Placement Offers (PPOs), Lateral Placement Offers (LPOs) interviews. -

0D\Dqn Sod\V Ihduohvvo\ Olnh 6Hkzdj /D[Pdq
!"#$%&' ( ' *+!'7 0 SMITH, WARNER BACK IN SHEFFIELD SHIELD Sydney: 0 ) 0 ".B& R ) H )* 9BC; ) ), ,- . R ( ) 9BC:H 9B9B 0 ormer India great VVS , ! ( Laxman feels Mayank FAgarwal’s “fearless” approach VIJENDER'S NEXT FIGHT ON NOV 22 $0. in batting resembles a lot with the New Delhi: 0 0 maverick Virender Sehwag, who * . <= has been the Karnataka opener’s ndia batsman Rohit Sharma, who idol. Ibecame the first player to score a cen- ) 99 H HH Agarwal had come into the tury in each innings of his maiden Test as <= ECCHB* D !6F limelight with twin half-centuries opener, on Monday jumped to a career-best 2 in his maiden Test tour of 17th position in the ICC Test Player ' CB$ (!" * Australia but maiden double hun- Rankings. ' 2 K . O dred (215) against South Africa Rohit, who now has five centuries from 0 has consolidated his position in 28 Tests, gained a whopping 36 slots after H H the national team, feels former his knocks of 176 and 127 in the first Test ( India spinner Harbhajan Singh. against South Africa in Visakhapatnam. -$ “He is a solid batsman and has The other opener Mayank Agarwal has approached this game like a also attained a career-best 25th position BARCA BEAT SEVILLA 4-0 IN LA LIGA domestic cricket match. Players after his first innings double-century lift- barcelona: $ 2 - usually change the way they play ed him 38 places. - O 2 in domestic and international Captain Virat Kohli, who retained his cricket, but he managed to main- second spot, has dropped below the 900- >HB - tain his style in both forms of point mark for the first time since January ( cricket. -

Page10spsorts.Qxd (Page 1)
TUESDAY, APRIL 27, 2021 (PAGE 10) DAILY EXCELSIOR, JAMMU Captain Morgan, bowlers beat Monday Cummins donates USD 50,000 to India’s Vriddhi Royals, Game Changer fight against COVID-19 pandemic blues to get past Punjab Kings NEW DELHI, Apr 26: rates remain high," he said. register wins in 3rd PPCPL AHMEDABAD, Apr 26: "I am advised that Indian Excelsior Sports Correspondent Dupesh took 2 wickets while commentator on live during the Kolkata Knight Riders' government is of the view that Zaheer and Sumit scalped 1 wicket matches and shared his valuable JAMMU, Apr 26: Vriddhi Australian pacer Pat Cummins playing the IPL while the popula- each. experiences with our viewers. He Skipper Eoin Morgan brought Royals and Game Changer regis- today announced a USD 50,000 tion is in lockdown provides few In reply, Samar Strikers also said that regular practice, pos- in a sense of calm after early jitters tered emphatic win against their donation towards PM CARES hours of joy and respite each day could not chase the target and man- itive attitude of a player and hard as Kolkata Knight Riders didn't let opponents in the ongoing 3rd Fund for oxygen supplies in at an otherwise difficult time for aged to score 41 runs by losing all work make a normal player to a a brilliant bowling performance PPCPL and entered in the next India's COVID-19 ravaged hospi- the country," Cummins said in his the wickets. Sumit made 43 runs, bigger and professional player. He go in vain during their easy five- stage of the league, being played at tals and backed the IPL to contin- statement. -
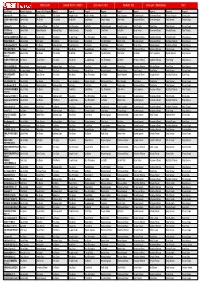
195Ys9v3lnjax- Part: 1
PBKS vs RR Contest: Win Rs. 10000.0 Entry Fee Rs. 39.0 Members: 339 Invite code: 195ys9v3lnjax- Part: 1 User (Team) Player 1 (Captain) Player 2 (Vice Captain) Player 3 Player 4 Player 5 Player 6 Player 7 Player 8 Player 9 Player 10 Player 11 1ghaznavi (1) Ben Stokes Rahul Tewatia Chris Jordan Deepak Hooda Jaydev Unadkat Jos Buttler Liam Livingstone Mayank Agarwal Mohammed Shami Moises Henriques Shivam Dube 2012DHY WOLFPACK Lokesh Rahul Ben Stokes Chris Jordan David Miller Dawid Malan Deepak Hooda Jofra Archer Mohammed Shami Moises Henriques Sanju Samson Shreyas Gopal (1) 2lukumar (1) Ben Stokes Mohammed Shami Chris Gayle Jhye Richardson Jos Buttler Mayank Agarwal Nicholas Pooran Rahul Tewatia Riyan Parag Sanju Samson Shreyas Gopal 9999999 nine Lokesh Rahul Mayank Agarwal Arshdeep Singh Chetan Sakariya Chris Gayle Chris Morris Jos Buttler Manan Vohra Mohammed Shami Nicholas Pooran Rahul Tewatia kadhamaal (1) AARIFAL SCORERS (1) Chris Gayle Lokesh Rahul Chris Morris Deepak Hooda Jhye Richardson Jos Buttler Mayank Agarwal Mohammed Shami Mustafizur Rahman Nicholas Pooran Sanju Samson ABASO Smita (1) Lokesh Rahul Chris Gayle Ben Stokes Chetan Sakariya Chris Morris Jhye Richardson Manan Vohra Mayank Agarwal Mohammed Shami Mustafizur Rahman Sanju Samson Abdulwadood786 (1) Lokesh Rahul Ben Stokes Arshdeep Singh Chetan Sakariya Chris Gayle Chris Morris Jos Buttler Manan Vohra Mayank Agarwal Mohammed Shami Sanju Samson ABHIJE8527QR (1) Ben Stokes Shreyas Gopal Chris Gayle Chris Morris Deepak Hooda Jos Buttler Lokesh Rahul Mohammed Shami Mustafizur