View Full Paper
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ENVIRONMENTAL IMPACT of GRAVEL MINING in COMMUNITIES in OJI RIVER LOCAL GOVERNMENT AREA of ENUGU STATE 1Officha, M.C., 2Okolie, A.O and 3Onwuemesi, F.E
GSJ: Volume 6, Issue 11, November 2018 ISSN 2320-9186 63 GSJ: Volume 6, Issue 11, November 2018, Online: ISSN 2320-9186 www.globalscientificjournal.com ENVIRONMENTAL IMPACT OF GRAVEL MINING IN COMMUNITIES IN OJI RIVER LOCAL GOVERNMENT AREA OF ENUGU STATE 1Officha, M.C., 2Okolie, A.O and 3Onwuemesi, F.E. 1Department of Architecture, Nnamdi Azikiwe University, Awka 1Department of Architecture, Chuwkuemeka Odumegwu Ojukwu University Uli, Anambra State. 3Department of Environmental Management, Nnamdi Azikiwe University, Awka. e-mail: [email protected]. Tell: +2348036938575 Abstract Increase in demand for sand and gravel mining has recently increased due to its demand in the construction of dams, roads, and building. The environmental impact of sand and gravel mining in three communities in Inyi town in Oji River Local Government Area of Enugu State has been studied using survey design. The aim of the study is to evaluate the impact of sand and gravel mining in the selected communities. The objectives of the study include; to investigate the method used by the miners in mining sand and gravel in the study area and to ascertain the impact of sand and gravel mining on the environment of the study area. Data for the study was collected through questionnaire, field observations and interview. 120 copies of well- structured questionnaire were distributed to the communities. Statistical tool use in the analysis of the data was simple percentage. From the study, sand and gravel mining in the selected communities has resulted to loss/reduction of farm lands and grazing lands, loss of vegetation, loss of biodiversity and economically important tress, destruction of landscape and beauty, confrontations/conflicts amongst communities, dust, water and soil pollution. -

Enugu State, Nigeria Out-Of-School Children Survey Report
ENUGU STATE, NIGERIA OUT-OF-SCHOOLCHILDREN SURVEY REPORT October, 2014 PREFACE The challenge of school-aged children who for one reason or another did not enrol in school at all or enrolled and later dropped out for whatever reason has been a perennial challenge to education the world over. Nigeria alone is said to house over 10 million out of school children. This is in spite of the universal basic education programme which has been running in the country since 1999. For Enugu State, it is not clear what the state contributes to that national pool of children who are reported to be out of school. Given the effort of the State Government in implementing the universal basic education programme, it is easy to assume that all children in Enugu State are enrolled and are attending school. This kind of assumption might not give us the benefit of knowing the true state of things as they relate to out-of-school children in our State. This is even more so given the State’s development and approval of the Inclusive Education Policy, which has increased the challenge of ensuring that every child of school age, no matter his or her circumstance of birth or residence, has access to quality education; hence, the need to be concerned even for only one child that is out of school. It is, therefore, in a bid to ascertain the prevalence of the incidence of children who are outside the school system, whether public or private, that the Ministry of Education and Enugu State Universal Basic Education Board collaborated with DFID-ESSPIN and other stakeholders to conduct the out of school children’s survey. -
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021
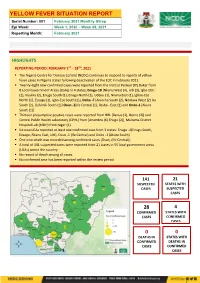
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021 HIGHLIGHTS REPORTING PERIOD: FEBRUARY 1ST – 28TH, 2021 ▪ The Nigeria Centre for Disease Control (NCDC) continues to respond to reports of yellow fever cases in Nigeria states following deactivation of the EOC in February 2021. ▪ Twenty -eight new confirmed cases were reported from the Institut Pasteur (IP) Dakar from 8 Local Government Areas (LGAs) in 4 states; Enugu-18 [Nkanu West (4), Udi (3), Igbo-Etiti (2), Nsukka (2), Enugu South (1), Enugu North (1), Udenu (1), Nkanu East (1), Igboe-Eze North (1), Ezeagu (1), Igbo-Eze South (1)], Delta -7 [Aniocha South (2), Ndokwa West (2) Ika South (2), Oshimili South (1)] Osun -2[Ife Central (1), Ilesha - East (1) and Ondo-1 [Akure South (1)] ▪ Thirteen presumptive positive cases were reported from NRL [Benue (2), Borno (2)] and Central Public Health Laboratory (CPHL) from [Anambra (6) Enugu (2)], Maitama District Hospital Lab (MDH) from Niger (1) ▪ Six new LGAs reported at least one confirmed case from 3 states: Enugu -4(Enugu South, Ezeagu, Nkanu East, Udi), Osun -1 (Ife Central) and Ondo -1 (Akure South) ▪ One new death was recorded among confirmed cases [Osun, (Ife Central)] ▪ A total of 141 suspected cases were reported from 21 states in 55 local government areas (LGAs) across the country ▪ No record of death among all cases. ▪ No confirmed case has been reported within the review period 141 21 SUSPECTED STATES WITH CASES SUSPECTED CASES 28 4 -

Evaluation of Rural Water Sources and Sustainable Approaches to Rural Water Resources Development in Ezeagu, Enugu, Eastern Nigeria
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Index Copernicus Value (2013): 6.14 | Impact Factor (2013): 4.438 Evaluation of Rural Water Sources and Sustainable Approaches to Rural Water Resources Development in Ezeagu, Enugu, Eastern Nigeria Nwagbara, A.O.1, Chijioke, E.O. 2 Faculty of Environmental Sciences, Enugu State University of Science and Technology, Agbani, Enugu, Nigeria Abstract: This study evaluated the water resources in Ezeagu and suggested sustainable approaches to water resources development in this area. Five towns were randomly selected from each of the three geographical zones and their water sources were evaluated. Direct observations, interviews and real time field survey were used to obtain reliable data on the state of water resources in the selected towns in Ezeagu Local Government Area. From the study, only three communities from the selected areas have big rivers that sustain their communities while others are water-stressed and depend on rain water harvesting, unprotected well, tanker-truck. It is obvious that nature has made the distribution of natural resources unequal. Tables 2 and 3 show that only Ozom Mgbagbu Owa, Olo and Umumba Ndiagu are the towns naturally endowed with big rivers that sustain them in Ezeagu Local Government Area. These rivers are the sources of water supply for the commercial water supply tanker drivers. Isigwu Umana, Aguobu Owa, Okpogho, Ihuonyia, Obeleagu Umana and Akama Oghe do not have reliable sources of water supply. Consequently they patronize the commercial tanker drivers. This study is significant as it will help the Local Government Authority in understanding the problems of Ezeagu Local Government Area with respect to availability of adequate and improved water supply. -

WOMEN and Elecnons in NIGERIA: SOME EMPIRICAL EVIDENCE from the DECEMBER 1991 Elecnons in ENUGU STATE
64 UFAHAMU WOMEN AND ELEcnONS IN NIGERIA: SOME EMPIRICAL EVIDENCE FROM THE DECEMBER 1991 ELEcnONS IN ENUGU STATE Okechukwu lbeanu Introduction Long before "modem" (Western) feminism became fashionable, the "woman question" had occupied the minds of social thinkers. In fact, this question dates as far back as the Judeo-Christian (Biblical) notion that the subordinate position of women in society is divinely ordained. • Since then, there have also been a number of biological and pseudo-scientific explanations that attribute the socio-economic and, therefore, political subordination of women to the menfolk, to women's physiological and spiritual inferiority to men. Writing in the 19th century, well over 1,800 years A. D., both Marx and Engels situate the differential social and political positions occupied by the two sexes in the relations of production. These relations find their highest expression of inequality in the capitalist society (Engels, 1978). The subordination of women is an integral part of more general unequal social (class) relations. For Marx, "the degree of emancipation of women is the natural measure of general emancipation" (Vogel, 1979: 42). Most writings on the "woman problematique" have generically been influenced by the above perspectives. However, more recent works commonly emphasized culture and socialization in explaining the social position of women. The general idea is that most cultures discriminate against women by socializing them into subordinate roles (Baldridge, 1975). The patriarchal character of power and opportunity structures in most cultures set the basis for the social, political and economic subordination of women. In consequence, many societies socialize their members into believing that public life is not for the female gender. -

Niger Delta Budget Monitoring Group Mapping
CAPACITY BUILDING TRAINING ON COMMUNITY NEEDS ASSESSMENT & SHADOW BUDGETING NIGER DELTA BUDGET MONITORING GROUP MAPPING OF 2016 CAPITAL PROJECTS IN THE 2016 FGN BUDGET FOR ENUGU STATE (Kebetkache Training Group Work on Needs Assessment Working Document) DOCUMENT PREPARED BY NDEBUMOG HEADQUARTERS www.nigerdeltabudget.org ENUGU STATE FEDERAL MINISTRY OF EDUCATION UNIVERSAL BASIC EDUCATION (UBE) COMMISSION S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Teaching and Learning 40,000,000 Enugu West South East New Materials in Selected Schools in Enugu West Senatorial District 2 Construction of a Block of 3 15,000,000 Udi Ezeagu/ Udi Enugu West South East New Classroom with VIP Office, Toilets and Furnishing at Community High School, Obioma, Udi LGA, Enugu State Total 55,000,000 FGGC ENUGU S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Construction of Road Network 34,264,125 Enugu- North Enugu North/ Enugu East South East New Enugu South 2 Construction of Storey 145,795,243 Enugu-North Enugu North/ Enugu East South East New Building of 18 Classroom, Enugu South Examination Hall, 2 No. Semi Detached Twin Buildings 3 Purchase of 1 Coastal Bus 13,000,000 Enugu-North Enugu North/ Enugu East South East Enugu South 4 Completion of an 8-Room 66,428,132 Enugu-North Enugu North/ Enugu East South East New Storey Building Girls Hostel Enugu South and Construction of a Storey Building of Prep Room and Furnishing 5 Construction of Perimeter 15,002,484 Enugu-North Enugu North/ Enugu East South East New Fencing Enugu South 6 Purchase of one Mercedes 18,656,000 Enugu-North Enugu North/ Enugu East South East New Water Tanker of 11,000 Litres Enugu South Capacity Total 293,145,984 FGGC LEJJA S/N PROJECT AMOUNT LGA FED. -

NIGERIAN AGRICULTURAL JOURNAL ISSN: 0300-368X Volume 49 Number 2, October 2018
NIGERIAN AGRICULTURAL JOURNAL ISSN: 0300-368X Volume 49 Number 2, October 2018. Pp. 242-247 Available online at: http://www.ajol.info/index.php/naj EFFECT OF RURAL-URBAN MIGRATION ON RICE PRODUCTION IN ENUGU STATE, NIGERIA 1Apu, U., 1Okore, H.O., 2Nnamerenwa, G.C. and 1Gbede, O.A. 1Department of Rural Sociology and Extension; 2Department of Agricultural Economics, Michael Okpara University of Agriculture, Umudike, Abia State Corresponding Authors’ email: [email protected] ABSTRACT This study assessed the effect of rural-urban migration on rice production in Enugu State, Nigeria. Multi-stage and Purposive sampling procedure was used to select 60 respondents which constituted the sample size of the study. Data were obtained through the use of a structured questionnaire. Descriptive statistics such as frequency counts and percentages, and inferential statistics such as correlation and z-test procedure were employed for analyses of data. Findings indicated that majority of the respondents (81.67%) were at their youthful age of 16 to 45 years old. The highest household size obtained was between 4 and 9 persons per household. Majority of the respondents in the study area (53.33%) were small scale farmers and had below 6 hectares of rice farm land. Poor living conditions, low influx of income and lack of employment were the most important reasons for rural-urban migration as confirmed by the respondents in Enugu State (65.00%). In the study area, 62.68% migrated to the urban areas. A larger proportion of the respondents (60.00%) indicated that between 4 and 9 household members participated in the rice production activities. -

The Impact of Supervised Agricultural Credit Scheme in Ezeagu Local Government Area of Enugu State, Nigeria
Botany Research International 6 (3): 74-80, 2013 ISSN 2221-3635 © IDOSI Publications, 2013 DOI: 10.5829/idosi.bri.2013.6.3.513 The Impact of Supervised Agricultural Credit Scheme in Ezeagu Local Government Area of Enugu State, Nigeria 12Miriam Mgbakor, Ugwu Jennifer Nkechi and 2G.N. Nenna 1Department of Agricultural Economics, Extension Enugu State University of Science and Technology (ESUT) Enugu, Nigeria 2Department of Agricultural Economics and Extension. Anambra State University, Igbariam Campus Abstract: This study investigated the impact of the Supervised Agricultural Credit Scheme on Small-scale farmers in Ezeagu Local Government Area of Enugu State of Nigeria. Three hundred and fifty farmers were randomly selected from the study area and interviewed by means of structured questionnaires. 300 questionnaires were later found to be analyzable. The findings indicate that the scheme had performed relatively well in the area of study and the repayment rates were high. Four innovations that had reached a high degree of adoption include: improved cassava; the supervised agricultural credit scheme (SACS); fertilizer and improved maize. Appropriate recommendations aimed at improving upon the functionality of the scheme in the study area have been made. Key words: Ezeagu Agricultural credit Small scale farming and Enugu INTRODUCTION Hitherto, shifting cultivation had been rife in some parts of the country. Traditional farming is plagued by The Problem: Agriculture plays a major role in the several constraints such as low capacity tools, very low economic development of many countries. Over 70 levels of production inputs, inadequate storage, percent of Nigeria’s adult population is engaged in the traditional land tenure system and heavy losses from agricultural sector and other related industries. -

Enugu State Nigeria Erosion and Watershed
RESETTLEMENT ACTION PLAN (RAP) Public Disclosure Authorized ENUGU STATE NIGERIA EROSION AND WATERSHED MANAGEMENT PROJECT (NEWMAP) Public Disclosure Authorized FOR THE 9TH MILE GULLY EROSION SUB-PROJECT INTERVENTION SITE Public Disclosure Authorized FINAL REPORT Public Disclosure Authorized RESETTLEMENT ACTION PLAN (RAP) ENUGU STATE NIGERIA EROSION AND WATERSHED MANAGEMENT PROJECT (NEWMAP) FOR THE 9TH MILE GULLY EROSION SUB-PROJECT INTERVENTION SITE FINAL REPORT Submitted to: State Project Management Unit Nigeria Erosion and Watershed Management Project (NEWMAP) Enugu State NIGERIA NOVEMBER 2014 Page | ii Resettlement Action Plan for 9th Mile Gully Erosion Site Enugu State- Final Report TABLE OF CONTENTS TABLE OF CONTENTS.................................................................................................................................................................... ii LIST OF FIGURES .................................................................................................................................................................... v LIST OF TABLES...................................................................................................................................................................... v LIST OF PLATES ...................................................................................................................................................................... v DEFINITIONS ....................................................................................................................................................................... -

Geoelectrical Sounding for the Determination of Groundwater Prospects in Awgu and Its Environs, Enugu State, Southeastern Nigeria
IOSR Journal of Applied Geology and Geophysics (IOSR-JAGG) e-ISSN: 2321–0990, p-ISSN: 2321–0982.Volume 5, Issue 1 Ver. I (Jan. - Feb. 2017), PP 14-22 www.iosrjournals.org Geoelectrical Sounding for The Determination Of Groundwater Prospects In Awgu And Its Environs, Enugu State, Southeastern Nigeria OKEKE J. P.1; EZEH C. C2. ; OKONKWO A. C3. 1,2,3(Department of Geology and Mining, Enugu state University of science and Technology, Enugu State, Nigeria. West Africa). [email protected] Abstract: Geoelectrical sounding to determine the groundwater prospect in Awgu and its environs has been carried out. The study area lies within longitudes 007025’E and 0070 35’E and latitudes 06002’N and 06017’N with an area extent of 513sqkm. The area is underlain by two lithostratigraphic units, Awgu Shale and Owelli Sandstone. A total of ninety five (95) Vertical Electrical Soundings (VES) was acquired employing the Schlumberger electrode array configuration, with a maximum electrode separation ranging from 700m to 800m. Data analysis was done using a computer program RESOUND to generate the layer apparent resistivity, thickness and depth. A maximum of eight (8) layer resistivity were generated in each sounding point with a depth range of 50m to 356m. From the interpreted VES data layer 6, 7, and 8 are possible target for prospective aquifer horizons. Interpreted geoelectric layers show a sequence of shale/sand – shale sand – sand. Various contour maps were constructed using surfer 10 contouring program- Iso resistivity, Isochore (depth), Isopach (thickness), Longitudinal conductance and transverse resistance to show variation of parameters in the study area. -
New Projects Inserted by Nass
NEW PROJECTS INSERTED BY NASS CODE MDA/PROJECT 2018 Proposed Budget 2018 Approved Budget FEDERAL MINISTRY OF AGRICULTURE AND RURAL SUPPLYFEDERAL AND MINISTRY INSTALLATION OF AGRICULTURE OF LIGHT AND UP COMMUNITYRURAL DEVELOPMENT (ALL-IN- ONE) HQTRS SOLAR 1 ERGP4145301 STREET LIGHTS WITH LITHIUM BATTERY 3000/5000 LUMENS WITH PIR FOR 0 100,000,000 2 ERGP4145302 PROVISIONCONSTRUCTION OF SOLAR AND INSTALLATION POWERED BOREHOLES OF SOLAR IN BORHEOLEOYO EAST HOSPITALFOR KOGI STATEROAD, 0 100,000,000 3 ERGP4145303 OYOCONSTRUCTION STATE OF 1.3KM ROAD, TOYIN SURVEYO B/SHOP, GBONGUDU, AKOBO 0 50,000,000 4 ERGP4145304 IBADAN,CONSTRUCTION OYO STATE OF BAGUDU WAZIRI ROAD (1.5KM) AND EFU MADAMI ROAD 0 50,000,000 5 ERGP4145305 CONSTRUCTION(1.7KM), NIGER STATEAND PROVISION OF BOREHOLES IN IDEATO NORTH/SOUTH 0 100,000,000 6 ERGP445000690 SUPPLYFEDERAL AND CONSTITUENCY, INSTALLATION IMO OF STATE SOLAR STREET LIGHTS IN NNEWI SOUTH LGA 0 30,000,000 7 ERGP445000691 TOPROVISION THE FOLLOWING OF SOLAR LOCATIONS: STREET LIGHTS ODIKPI IN GARKUWARI,(100M), AMAKOM SABON (100M), GARIN OKOFIAKANURI 0 400,000,000 8 ERGP21500101 SUPPLYNGURU, YOBEAND INSTALLATION STATE (UNDER OF RURAL SOLAR ACCESS STREET MOBILITY LIGHTS INPROJECT NNEWI (RAMP)SOUTH LGA 0 30,000,000 9 ERGP445000692 TOSUPPLY THE FOLLOWINGAND INSTALLATION LOCATIONS: OF SOLAR AKABO STREET (100M), LIGHTS UHUEBE IN AKOWAVILLAGE, (100M) UTUH 0 500,000,000 10 ERGP445000693 ANDEROSION ARONDIZUOGU CONTROL IN(100M), AMOSO IDEATO - NCHARA NORTH ROAD, LGA, ETITI IMO EDDA, STATE AKIPO SOUTH LGA 0 200,000,000 11 ERGP445000694 -

Spectral Analysis of Aeromagnetic Anomalies from Parts of Mmaku and Its Adjoining Areas in Southeastern, Nigeria
International Journal of Scientific and Research Publications, Volume 5, Issue 10, October 2015 1 ISSN 2250-3153 Spectral Analysis of Aeromagnetic Anomalies from Parts of Mmaku and its Adjoining Areas in Southeastern, Nigeria Ofoha C.C Department of physics, University of Port Harcourt, Rivers State, Nigeria Abstract- To estimate the depth to various magnetic sources transgression, regression and local tectonics (Petters, 1978). within the study area, an aeromagnetic map with sheet number Spectral depth analytical technique which describes the 301 published on a scale of 1:100000 was processed, analyzed frequency content of a signal based on a finite set of data (Igwesi and interpreted using spectral depth analytical technique with the and Umego, 2013) has proven to be apt for the determination of aid of Arc GIS, Ms Excel and Origin Pro Software’s. In this the depth to basement. Its advantage is that the spectral domain study, two layered source model, D1 and D2 were observed and expressions of the anomalies are generally simple as compared to proposed and also prospective areas were delineated using Surfer the expressions of the anomalies in the space domain (Igwesi and 10. The topographic map generated using Surfer 10 shows the Umego, 2013). The method averages over an area so that, if undulating nature of the basement surface. Depths to the deeper noise is a factor, the results will give a more accurate result than magnetic sources, D1 vary from 3.472 km to 6.972 km but with other methods that are commonly used (Ofoha, 2015). Finally, an average depth value of 5.010 km while the depth to shallower features with given direction in space domain are transformed magnetic sources, D2 vary from 1.177 km to 1.834 km but with into a feature with only one direction in the spectral domain an average depth of 1.047 km.