Female Genital Mutilation: Perspectives, Risks, and C Omplications
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

Clitoridectomy, Excision, Infibulation- Female Circumcision Ritual and Its Consequences for Women's Health
Rogala Dorota, Kornowska Joanna, Ziółkowska Mirosława. Clitoridectomy, excision, infibulation- female circumcision ritual and its consequences for women's health. Journal of Education, Health and Sport. 2018;8(11):583-593. eISNN 2391-8306. DOI http://dx.doi.org/10.5281/zenodo.2533136 http://ojs.ukw.edu.pl/index.php/johs/article/view/6451 https://pbn.nauka.gov.pl/sedno-webapp/works/896357 The journal has had 7 points in Ministry of Science and Higher Education parametric evaluation. Part B item 1223 (26/01/2017). 1223 Journal of Education, Health and Sport eISSN 2391-8306 7 © The Authors 2018; This article is published with open access at Licensee Open Journal Systems of Kazimierz Wielki University in Bydgoszcz, Poland Open Access. This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author (s) and source are credited. This is an open access article licensed under the terms of the Creative Commons Attribution Non commercial license Share alike. (http://creativecommons.org/licenses/by-nc-sa/4.0/) which permits unrestricted, non commercial use, distribution and reproduction in any medium, provided the work is properly cited. The authors declare that there is no conflict of interests regarding the publication of this paper. Received: 26.11.2018. Revised: 30.11.2018. Accepted: 30.11.2018. Clitoridectomy, excision, infibulation- female circumcision ritual and its consequences for women's health Dorota Rogala ¹, Joanna Kornowska 2, Mirosława Ziółkowska3 1 Department of Oncology, Radiotherapy and Gynecologic Oncology, Faculty of Health Sciences, Collegium Medicum, Nicolaus Copernicus University, Toruń, Poland. -

Status of the Crusade to Eradicate Female Genital Mutilation: a Comparative Analysis of Laws and Programs in the United States and Egypt, the Elizabeth A
Penn State International Law Review Volume 22 Article 11 Number 4 Penn State International Law Review 5-1-2004 Status of the Crusade to Eradicate Female Genital Mutilation: A Comparative Analysis of Laws and Programs in the United States and Egypt, The Elizabeth A. Syer Follow this and additional works at: http://elibrary.law.psu.edu/psilr Recommended Citation Syer, Elizabeth A. (2004) "Status of the Crusade to Eradicate Female Genital Mutilation: A Comparative Analysis of Laws and Programs in the United States and Egypt, The," Penn State International Law Review: Vol. 22: No. 4, Article 11. Available at: http://elibrary.law.psu.edu/psilr/vol22/iss4/11 This Comment is brought to you for free and open access by Penn State Law eLibrary. It has been accepted for inclusion in Penn State International Law Review by an authorized administrator of Penn State Law eLibrary. For more information, please contact [email protected]. I Comment I The Status of the Crusade to Eradicate Female Genital Mutilation: A Comparative Analysis of Laws and Programs in the United States and Egypt Elizabeth A. Syer* John F. Kennedy once said, "[O]ur progress as a nation can be no swifter than our progress in education. The human mind is our fundamental resource."' This notion still holds true today. Throughout the course of history, education has proven to be an explosive technique in battling against human rights violations. 2 Female Genital Mutilation (hereinafter "FGM") or female circumcision is a battle that must be fought using education as its cannon;3 only then will this cruel and * Elizabeth A. -

Ovarian Cancer and Cervical Cancer
What Every Woman Should Know About Gynecologic Cancer R. Kevin Reynolds, MD The George W. Morley Professor & Chief, Division of Gyn Oncology University of Michigan Ann Arbor, MI What is gynecologic cancer? Cancer is a disease where cells grow and spread without control. Gynecologic cancers begin in the female reproductive organs. The most common gynecologic cancers are endometrial cancer, ovarian cancer and cervical cancer. Less common gynecologic cancers involve vulva, Fallopian tube, uterine wall (sarcoma), vagina, and placenta (pregnancy tissue: molar pregnancy). Ovary Uterus Endometrium Cervix Vagina Vulva What causes endometrial cancer? Endometrial cancer is the most common gynecologic cancer: one out of every 40 women will develop endometrial cancer. It is caused by too much estrogen, a hormone normally present in women. The most common cause of the excess estrogen is being overweight: fat cells actually produce estrogen. Another cause of excess estrogen is medication such as tamoxifen (often prescribed for breast cancer treatment) or some forms of prescribed estrogen hormone therapy (unopposed estrogen). How is endometrial cancer detected? Almost all endometrial cancer is detected when a woman notices vaginal bleeding after her menopause or irregular bleeding before her menopause. If bleeding occurs, a woman should contact her doctor so that appropriate testing can be performed. This usually includes an endometrial biopsy, a brief, slightly crampy test, performed in the office. Fortunately, most endometrial cancers are detected before spread to other parts of the body occurs Is endometrial cancer treatable? Yes! Most women with endometrial cancer will undergo surgery including hysterectomy (removal of the uterus) in addition to removal of ovaries and lymph nodes. -
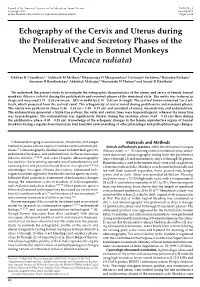
Echography of the Cervix and Uterus During the Proliferative and Secretory Phases of the Menstrual Cycle in Bonnet Monkeys (Macaca Radiata)
Journal of the American Association for Laboratory Animal Science Vol 53, No 1 Copyright 2014 January 2014 by the American Association for Laboratory Animal Science Pages 18–23 Echography of the Cervix and Uterus during the Proliferative and Secretory Phases of the Menstrual Cycle in Bonnet Monkeys (Macaca radiata) Uddhav K Chaudhari,1,* Siddnath M Metkari,2 Dhyananjay D Manjaramkar,2 Geetanjali Sachdeva,1 Rajendra Katkam,1 Atmaram H Bandivdekar,3 Abhishek Mahajan,4 Meenakshi H Thakur,4 and Sanjiv D Kholkute1 We undertook the present study to investigate the echographic characteristics of the uterus and cervix of female bonnet monkeys (Macaca radiata) during the proliferative and secretory phases of the menstrual cycle. The cervix was tortuous in shape and measured 2.74 ± 0.30 cm (mean ± SD) in width by 3.10 ± 0.32 cm in length. The cervical lumen contained 2 or 3 col- liculi, which projected from the cervical canal. The echogenicity of cervix varied during proliferative and secretory phases. The uterus was pyriform in shape (2.46 ± 0.28 cm × 1.45 ± 0.19 cm) and consisted of serosa, myometrium, and endometrium. The endometrium generated a triple-line pattern; the outer and central lines were hyperechogenic, whereas the inner line was hypoechogenic. The endometrium was significantly thicker during the secretory phase (0.69 ± 0.12 cm) than during the proliferative phase (0.43 ± 0.15 cm). Knowledge of the echogenic changes in the female reproductive organs of bonnet monkeys during a regular menstrual cycle may facilitate understanding of other physiologic and pathophysiologic changes. Ultrasound imaging is a noninvasive, atraumatic, and simple Materials and Methods method to assess various organs in humans and nonhuman pri- Animals and husbandry practices. -

Three Middle Eastern American Plays
Tiyatro Eleştirmenliği ve Dramaturji Bölümü Dergisi Journal of Theatre Criticism and Dramaturgy Tiyatro Eleştirmenliği ve Dramaturji Bölümü Dergisi 30, (2020): 35-52 DOI: 10.26650/jtcd.698395 Research Article/Araştırma Makalesi Representation of Problems or Problematic Representation: Three Middle Eastern American Plays Nazila Heidarzadegan1 ABSTRACT Globally, several theatrical performances have staged the consequences of the ‘war on terror’ after 9/11. This paper provides insights into how Middle Eastern American dramatists and characters responded to the war and the post-9/11 era. It explores how Middle Easterners in an American context were stereotyped, *This article is prepared with reference to transformed into problematic subjects, how they resisted backlashing policies, the phd dissertation titled “The Problem of and were influenced by fallout effects of the event in the plays Browntown, Representation in Middle Eastern American Theatre: A Postcolonial Approach” which I Ten Acrobats in an Amazing Leap of Faith, and Nine Parts of Desire by reading completed in 2015 in the Atatürk University them through Homi Bhabha’s postcolonial concepts. This paper argues for Institute of Social Sciences English Language the necessity of recognizing hyphenated people in the mainstream context and Literature Department. and approaches the problem in terms of negotiation instead of the negation 1Assist. Prof. Dr. Karabuk University, Department of hyphenated identities to avoid potential identity problems which may of Western Languages and Literature, lead to social problems. It calls for dramatists of artistic productions to claim Karabuk, Turkey recognition of their identity and correct the distorted images to prevent their ORCID: N.H. 0000-0003-1238-7903 transformation into problematic realms. -

Caring for Yourself After Your Cone Biopsy of the Cervix | Memorial Sloan Kettering Cancer Center
PATIENT & CAREGIVER EDUCATION Caring for Yourself After Your Cone Biopsy of the Cervix This information explains how to care for yourself after a cone biopsy of your cervix. About Your Cone Biopsy of the Cervix Your cervix is the bottom part of your uterus. It connects your uterus to your vagina (see Figure 1). It’s the part of your uterus that dilates (opens) during childbirth. When you have your period, menstrual blood flows through your cervix to your vagina and out of your body. Figure 1. Uterus, cervix, and vagina Caring for Yourself After Your Cone Biopsy of the Cervix 1/3 During a cone biopsy, your doctor will remove a small, cone-shaped part of your cervix. They will study it under a microscope to look for abnormal cells. It usually takes about 4 to 6 weeks for your cervix to heal after this procedure. Caring for Yourself at Home In the first 24 hours after your procedure: Drink 8 to 12 (8-ounce) glasses of liquids. Eat well-balanced, healthy meals. The first 4 days after your procedure, you may have vaginal discharge that looks like menstrual bleeding. The amount varies for everyone. Over the next 2 to 3 weeks after your procedure, your vaginal discharge will become clear and watery and then will stop. Use sanitary pads for vaginal discharge. For 4 to 6 weeks after your procedure or until your doctor tells you your cervix is healed: Don’t put anything inside your vagina (such as tampons and douches) or have vaginal intercourse. Take showers instead of baths. -

Female Genital Cutting: Breaking the Silence, Enabling Change
Synthesis Paper Female Genital Cutting: Breaking the Silence, Enabling Change Julia M. Masterson Julie Hanson Swanson Photos courtesy of: Julia Masterson Design: Manu Badlani Copyright© 2000 International Center for Research on Women and The Centre for Development and Population Activities Female Genital Cutting: Breaking the Silence, Enabling Change Julia M. Masterson Julie Hanson Swanson Table of Contents Preface ................................................................................................................................................. 3 Acknowledgments .............................................................................................................................. 4 Executive Summary............................................................................................................................ 5 Introduction ........................................................................................................................................ 7 What is FGC? ....................................................................................................................................... 8 Applying Global Rights at the Local Level: Three Approaches to Ending FGC ........................... 12 Enabling Change: Lessons and Recommendations....................................................................... 23 Next Steps .......................................................................................................................................... 31 Appendix .......................................................................................................................................... -

Colposcopy of the Uterine Cervix
THE CERVIX: Colposcopy of the Uterine Cervix • I. Introduction • V. Invasive Cancer of the Cervix • II. Anatomy of the Uterine Cervix • VI. Colposcopy • III. Histology of the Normal Cervix • VII: Cervical Cancer Screening and Colposcopy During Pregnancy • IV. Premalignant Lesions of the Cervix The material that follows was developed by the 2002-04 ASCCP Section on the Cervix for use by physicians and healthcare providers. Special thanks to Section members: Edward J. Mayeaux, Jr, MD, Co-Chair Claudia Werner, MD, Co-Chair Raheela Ashfaq, MD Deborah Bartholomew, MD Lisa Flowers, MD Francisco Garcia, MD, MPH Luis Padilla, MD Diane Solomon, MD Dennis O'Connor, MD Please use this material freely. This material is an educational resource and as such does not define a standard of care, nor is intended to dictate an exclusive course of treatment or procedure to be followed. It presents methods and techniques of clinical practice that are acceptable and used by recognized authorities, for consideration by licensed physicians and healthcare providers to incorporate into their practice. Variations of practice, taking into account the needs of the individual patient, resources, and limitation unique to the institution or type of practice, may be appropriate. I. AN INTRODUCTION TO THE NORMAL CERVIX, NEOPLASIA, AND COLPOSCOPY The uterine cervix presents a unique opportunity to clinicians in that it is physically and visually accessible for evaluation. It demonstrates a well-described spectrum of histological and colposcopic findings from health to premalignancy to invasive cancer. Since nearly all cervical neoplasia occurs in the presence of human papillomavirus infection, the cervix provides the best-defined model of virus-mediated carcinogenesis in humans to date. -

Violence Against Women in Africa: a Situational Analysis
United Nations Economic Commission for Africa African Centre for Gender and Social Development (ACGSD) VIOLENCE AGAINST WOMEN IN AFRICA: A SITUATIONAL ANALYSIS Table of Contents Background Methodology Common Abbreviations Situation Analysis of Africa Algeria Angola Benin Botswana Burkina Faso Burundi Cameroon Cape Verde Central African Republic Chad Comoros Congo Cote D’Ivoire Djibouti Democratic Republic of Congo Egypt Equatorial Guinea Eritrea Ethiopia Gabon Gambia Ghana Guinea Bissau Guinea Kenya Lesotho Liberia Libya Madagascar Malawi Mali Mauritania Mauritius Morocco Mozambique Namibia Niger Nigeria Rwanda Sao Tome and Principe Senegal Seychelles Sierra Leone Somalia South Africa Sudan Swaziland Tanzania Togo Tunisia Uganda Zambia Zimbabwe Background Violence against women is perhaps the most widespread and socially tolerated of human rights violations, cutting across borders, race, class, ethnicity and religion. The impact of gender-based violence (GBV) is devastating. The individual women who are victims of such violence often experience life-long emotional distress, mental health problems and poor reproductive health, as well as being at higher risk of acquiring HIV and intensive long-term users of health services. In addition, the cost to women, their children, families and communities is a significant obstacle to reducing poverty, achieving gender equality and ensuring a peaceful transition for post-conflict societies. This, in conjunction with the mental and physical health implications of gender-based violence, impacts on a state or region’s ability to develop and construct a stable, productive society, or reconstruct a country in the wake of conflict. Gender-based violence in Africa, as elsewhere in the world, is a complex issue that has as its root the structural inequalities between men and women that result in the persistence of power differentials between the sexes. -
How Culture Is Affecting Women's Health
Canadian Open Nursing and Midwifery Journal Vol. 1, No. 1, May 2016, pp. 1-13 http://crpub.com/Journals.php Open Access Open Access Research article How Culture is Affecting Women’s Health Angela Bedard, RN, BScN E-mail: [email protected] This work is licensed under a Creative Commons Attribution 4.0 International License ______________________________________________ Abstract Women’s health and the importance placed on it has been an ongoing global issue for many years. The laws of basic human rights for some reason have left women in a very vulnerably and unhealth state which is directly caused by certain societal standards, cultural practices, and religious beliefs. Women’s health and life’s value in certain areas of the world are not as highly regarded as that of a man. Some of the women’s health violations that are having a large effect on women’s health today are: female genital mutilation, gavage, eating disorders, and female feticid. These violations have arisen from partrichial religious favoritism, societal pressures that have been established through media and law, and ideologies surrounding family honor. In countries like North Amerca across to Asia, traditions and the value on women are causing serious global health issues that are burdening the health care system and further more increasing the amount of preventable diseases and deaths accounted for every year. In health care it is important to identify these challenges women are facing globally and how organizations can provide a safer and healthier future for women worldwide. Education is the most effective way to promote health and prevent the reoccurence of current health issues women are facing today. -

CERVICAL CANCER About Gynecologic Cancer
CERVICAL CANCER About Gynecologic Cancer There are five main types of cancer that affect a woman’s reproductive organs: cervical, ovarian, uterine, vaginal, and vulvar. As a group, they are referred to as gynecologic (GY-neh-kuh-LAH-jik) cancer. (A sixth type of gynecologic cancer is the very rare fallopian tube cancer.) This fact sheet about cervical cancer is part of the Centers for Disease Control and Prevention’s (CDC) Inside Knowledge: About Gynecologic Cancer campaign. The campaign helps women get the facts about gynecologic cancer, providing important “inside knowledge” about their bodies and health. What is cervical cancer? Cancer is a disease in which cells Are there tests that can prevent cervical cancer or find it early? in the body grow out of control. There are two tests that can either help prevent cervical cancer or find it early: Cancer is always named for the part of the body where it starts, even if it • Depending on your age, your doctor may recommend you have a Pap spreads to other body parts later. test, or an HPV test, or both tests together. When cancer starts in the • The Pap test (or Pap smear) looks for precancers, cell changes, on the cervix, it is called cervical cancer. cervix that can be treated, so that cervical cancer is prevented. The Pap The cervix is the lower, narrow test also can find cervical cancer early, when treatment is most effective. end of the uterus. The cervix The Pap test only screens for cervical cancer. It does not screen for any connects the vagina (the birth canal) other gynecologic cancer.