In Epidemiology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Willingness to Pay for Margalla Hills National Park: Evidence from the Travel Cost Method
The Lahore Journal of Economics 11 : 2 (Winter 2006) pp. 43-70 Willingness to Pay for Margalla Hills National Park: Evidence from the Travel Cost Method Himayatullah Khan* Abstract This study, which is among the first in Pakistan to value recreational benefits, estimates the benefits of the Margalla Hills National Park near Islamabad. The study examines how much park visitors are willing to pay to visit the park. Annual benefits from the park are considerable—the total annual consumer surplus or economic benefit obtained from recreation in the park is approximately Rs. 23 million (US $ 0.4 million). Various factors influence the value visitors obtain from the park — these include travel cost, household income, and the quality of the park. Improvements in the quality of the park are estimated to increase recreational benefits by 39%. The study recommends that a park entrance fee of Rs. 20 per person be introduced, which could be utilized for park management. This would generate nearly Rs. 11 million in revenues annually, a sizable amount of money that represents about 4% of the annual budget allocated to the environment sector in Pakistan. JEL Classification: Keywords: Environmental valuation, willingness to pay, total recreational value, consumer surplus, environmental resources, national parks, Pakistan. * The author is Professor at the Institute of Development Studies, NWFP Agricultural University, Peshawar and currently on deputation to Department of Development Studies, COMSATS Institute of Information Technology, Abbottabad. This paper is based on Himayatullah (2003). The author gratefully acknowledges the financial support provided by the South Asian Network for Development and Environmental Economics (SANDEE). -

On Epidemiology and Geographic Information Systems: a Review and Discussion of Future Directions Keith C
Perspectives On Epidemiology and Geographic Information Systems: A Review and Discussion of Future Directions Keith C. Clarke, Ph.D., Sara L. McLafferty, Ph.D,. and Barbara J. Tempalski Hunter College-CUNY, New York, New York, USA Geographic information systems are powerful automated systems for the capture, stor- age, retrieval, analysis, and display of spatial data. While the systems have been in development for more than 20 years, recent software has made them substantially easier to use for those outside the field. The systems offer new and expanding opportunities for epidemiology because they allow an informed user to choose between options when geographic distributions are part of the problem. Even when used minimally, these systems allow a spatial perspective on disease. Used to their optimum level, as tools for analysis and decision making, they are indeed a new information management vehicle with a rich potential for public health and epidemiology. Geographic information systems (GIS) are Computers were first applied to geography as “automated systems for the capture, storage, re- analytical and display tools during the 1960s (3). trieval, analysis, and display of spatial data” (1). GIS emerged as a multidisciplinary field during Common to all GIS is a realization that spatial the 1970s. The discipline’s heritage lies in cartog- data are unique because their records can be raphy’s mathematical roots: in urban planning’s linked to a geographic map. The component parts map overlay methods for selecting regions and of a GIS include not just a database, but also locations based on multiple factors (4); in the im- spatial or map information and some mechanism pact of the quantitative revolution on the disci- to link them together.GIS has also been described pline of geography; and in database management as the technology side of a new discipline, geo- developments in computer science. -

Common Mullein, Pharmacological and Chemical Aspects
Rev Bras Farmacogn 23(2013): 948-959 Review Article Common mullein, pharmacological and chemical aspects Muhammad Riaza,*, Muhammad Zia-Ul-Haqb, Hawa Z.E. Jaafarc,* aDepartment of Pharmacy, University of Swabi, Pakistan bThe Patent Office, Karachi, Pakistan cDepartment of Crop Science, Faculty of Agriculture, University Putra Malaysia, Selangor, Malaysia ARTICLE INFO ABSTRACT Article history: Verbascum thapsus L. [Khardhag or Common mullein], a member of the family Scrophulariaceae, Received 17 November 2013 is a famous herb that is found all over Europe, in temperate Asia, in North America and is Accepted 30 December 2013 well-reputed due to its medicinal properties. This medicinal herb contains various chemical constituents like saponins, iridoid and phenylethanoid glycosides, flavonoids, vitamin C Keywords: and minerals. It is famous in various communities worldwide for the treatment of various Verbascum thapsus disorders of both humans and animals aliments. A number of pharmacological activities Phytochemistry such as anti-inflammatory, antioxidant, anticancer, antimicrobial, antiviral, antihepatotoxic Pharmacology and anti-hyperlipidemic activity have been ascribed to this plant. The plant is used to treat Ethnomedicinal tuberculosis also, earache and bronchitis. In the present paper botanical and ethnomedicinal Scrophulariaceae description, pharmacological profile and phytochemistry of this herb is being discussed. © 2013 Brazilian Society of Pharmacognosy. Published by Elsevier Editora Ltda. All rights reserved. Introduction also in advanced countries (Turker and Camper, 2002) where the United States like dried leaves and flowers, capsules, The origin of majority of remedies, recipes and alcohlic extracts and the flower oil of this plant can easily pharmaceuticals has been traced to medicinal plants. There be found in health stores (Turker and Gurel, 2005). -

Public Health GIS News and Information, No. 44 (January 2002)
PUBLIC HEALTH GIS NEWS AND INFORMATION January 2002 (No. 44) Dedicated to CDC/ATSDR scientific excellence and advancement in disease control and prevention using GIS Selected Contents: Events Calendar (pp.1-2); News from GIS Users (pp.2-6); GIS Outreach (pp.6-7); Public Health and GIS Literature (pp.7-17); DHHS and Federal Update (pp.17- 21); Website(s) of Interest (pp.21-22); Final Thoughts (pp.22-24) I. Public Health GIS (and related)Events Austin, Texas [See site: http://www.tnris.state.tx.us/gis SPECIAL NCHS/CDC/ATSDR GIS LECTURES festival] FEBRUARY 12, 2002. “Mapping Community- � Level Housing and Related Data on the Web at the Fifth Annual International Conference: Map India Department of Housing and Urban Development 2002, February 6-8, 2002, New Delhi, India [See: (HUD)” by Jon Sperling and David Chase, U.S. http://www.mapindia.org] Department of Housing and Urban Development � th (HUD), from 2:00-3:30PM. This NCHS Cartography 8 Biennial Symposium on Minorities, the and GIS Guest Lecture Series programs will be held at Medically Underserved & Cancer, February 6-10, the NCHS Auditorium, RM1100, Hyattsville, MD; 2002, Washington, D.C. [See: http://www.iccnetwork. Envision is available to offsite CDC/ATSDR org] locations; Web access is available to all others at � http://video.cdc.gov/ramgen/envision/live.rm (link GIS and Crime Science Conference, February 14, becomes active approximately 30 minutes prior to the 2002, University of London, London, England [See: event and viewing requires RealPlayer http://www.ucl.ac.uk/spp/jdi/events_pubs.htm] installation).See abstract for presentations in this � edition. -
Pdfmachine Trial Version
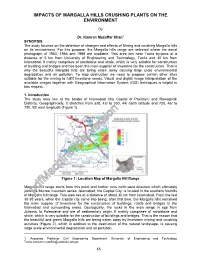
IMPACTS OF MARGALLA HILLS CRUSHING PLANTS ON THE ENVIRONMENT By Dr. Kamran Muzaffar Khan1 SYNOPSIS The study focuses on the detection of changes and effects of Mining and crushing Margalla hills on its environment. For this purpose, the Margalla hills range are selected where the aerial photograph of 1953, 1986 and 1999 are available. This area lies near Taxila by-pass at a distance of 5 km from University of Engineering and Technology, Taxila and 30 km from Islamabad. It mainly comprises of sandstone and shale, which is very suitable for construction of building and bridges and has been the main supplier of limestone for the construction. That is why the beautiful Margalla hills are being eaten away causing large scale environmental degradation and air pollution. To stop destruction we need to propose certain other sites suitable for the mining to fulfill limestone needs. Visual and digital image interpretation of the available images together with Geographical Information System (GIS) techniques is helpful in this respect. 1. Introduction The study area lies at the border of Islamabad (the Capital of Pakistan) and Rawalpindi Districts. Geographically, it stretches from 330, 42/ to 330, 44/ north latitude and 720, 46/ to 720, 52/ east longitude (Figure 1). Figure 1: Location Map of Margalla Hill Range Margalla hill range starts from this point and further runs north-west direction which ultimately joins tpdfMachinehe Murree mountain series .trial Islamab aversiond, the Capital City; is located in the southern foothills of Margalla hill range. This area lies at a distance of about 30 km from Islamabad. -

Public Health GIS News and Information, No. 43 (November 2001)
PUBLIC HEALTH GIS NEWS AND INFORMATION November 2001 (No. 43) Dedicated to CDC/ATSDR scientific excellence and advancement in disease control and prevention using GIS Selected Contents: Events Calendar (pp.1-2); News from GIS Users (pp.2-8); GIS Outreach (p.8); Public Health and GIS Literature (pp.8-15); DHHS and Federal Update (pp.16- 22); Website(s) of Interest (pp.22-24); Final Thoughts (pp.24-25) I. Public Health GIS (and related)Events [Note: Calendar events are posted as received; for a more complete SPECIAL NCHS/CDC/ATSDR GIS LECTURES: listing see prior two bimonthly reports at NCHS GIS website] K "GIS In Telecoms 2001," The Open GIS 14th Annual Geography Awareness Week Consortium, Inc. (OGC) (Wayland, MA) and IIR NOVEMBER 27, 2001 “GIS and Lyme Disease: Conferences-UK (UK), November 12-15, 2001, Exploring Space-Time Relationships with Geneva, Switzerland [See: http://www.iir-conferences. Geostatistics,” by Lee De Cola, Geographer and com] Mathematician, U.S. Geological Survey and Charles M. Croner, Geographer and Survey Statistician, L GIS Day 2001: “Discovering the World through Office of Research and Methodology, NCHS, CDC, GIS,” November 14, 2001 [See: http://www.gisday. from 2:00-3:30PM. com] NOVEMBER 29, 2001. “LandView V: A Federal Spatial Data Viewer,” by E. J. (Jerry) McFaul, K First Annual ESRI Health Conference, November Computer Scientist, U.S. Geological Survey, and and 12-14, 2001, Washington, DC [See: http://www.esri. Peter Gattuso, Information Management Specialist at com] the Environmental Protection Agency, from -

Rubus Fruticosus and Verbascum Thapsus Medicinal Plants Collected from Dir (L) N.W.F.P
Antioxidant and anti-inflammatory study of Rubus fruticosus and Verbascum thapsus medicinal plants collected from Dir (L) N.W.F.P. Pakistan Muhammad Riaz, B. Pharm. Department of Pharmacognosy Faculty of Pharmacy, University of Karachi Karachi-75270, Pakistan 2012 Antioxidant and anti-inflammatory study of Rubus fruticosus and Verbascum thapsus medicinal plants collected from Dir (L) N.W.F.P. Pakistan THESIS SUBMITTED FOR THE FULFILMENT OF THE DEGREE OF DOCTOR OF PHILLOSOPHY By Muhammad Riaz, B. Pharm. Supervised by Dr. Mansoor Ahmad, I.F. Meritorious Professor Department of Pharmacognosy Faculty of Pharmacy, University of Karachi Karachi-75270, Pakistan 2012 DIDICATED TO MY PARENTS i PUBLICATION FROM THESIS Riaz M , Ahmad M and Rahman N (2011). Antimicrobial screening of fruit, leaves, root and stem of Rubus fruticosus . J. Med. Plants Res ., 5(24): 5920-5924. ii CONTENTS i. Acknowledgements viii ii. Abstract ix iii. Khulasa xii 1. Introduction 01 I. Rubus fruticosus 03 II. Verbascum thapsus 07 2. Literature search i. Literature survey of Rubus fruticosus 13 ii. Therapeutic application of Rubus fruticosus 15 iii. Literature data for total phenols, anthocyanins and ascorbic acid 17 iv. Phytochemical literature survey of Rubus fruticosus 18 v. Structures of chemical constituents reported from R. fruticosus 23 vi. Literature survey of Verbascum thapsus 28 vii. Pharmacological literature survey of Verbascum thapsus 30 viii. Phytochemical literature survey of Verbascum thapsus 32 ix. Structures of chemical constituents reported from V. thapsus 38 3. Experimental 42 i. General/Materials 42 ii. Instruments 43 iii. Abbreviations 44 iv. Pharmacognostic evaluation/Standardization of drugs 45 v. Thin layer chromatography 48 vi. -

6 X 10.5 Three Line Title.P65
Cambridge University Press 978-0-521-86169-4 - Sorrow and Joy among Muslim Women: The Pukhtuns of Northern Pakistan Amineh Ahmed Frontmatter More information Sorrow and Joy among Muslim Women The Pukhtuns are numerically and politically one of the most significant ethnolinguistic groups in Pakistan and Afghanistan. This important study of Pukhtun society concentrates on the lives, thoughts and gham-khadi¯ (funeral- wedding) ceremonies of the women, especially of the elite, wealthy and educated women (Bibiane) who have largely been overlooked in previous studies. Con- testing their conventional representation as idle, it illustrates their commitment to various forms of work within familial and social contexts. It challenges the commonly assumed models of contemporary Pakistan society, which make a simplistic divide between rural and urban, Punjab and non-Punjab, and feudal and non-feudal spaces and peoples. It also contributes to broader debates about the nature and expression of elite cultures and issues of sociality, funerals and marriage, custom and religion, space and gender, morality and reason, and social role and personhood within the contexts of Islam in the Middle East and South Asia. amineh ahmed hoti received her PhD from the Faculty of Social Anthro- pology at the University of Cambridge and is a Visiting Scholar at Lucy Cavendish College. She runs the Society for Dialogue and Action, which promotes under- standing between people of the Abrahamic faiths, namely Jews, Christians and Muslims. © Cambridge University Press www.cambridge.org -

Monitoring Forest Fire with Climatic, Vegetation, Topography and Human
Monitoring Forest Fire using Geo-Spatial Information Techniques and Spatial Statistics: One Case Study of Forest re in Margalla Hills, Islamabad, Pakistan Aqil Tariq Wuhan University Hong Shu ( [email protected] ) Wuhan University https://orcid.org/0000-0003-2108-1797 Saima Siddiqui University of the Punjab Research Keywords: Forest re, Geospatial analysis, Delta normalized burn ratio, Determining factors, Fire severity. Posted Date: August 25th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-60874/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License 1 Monitoring forest fire using Geo-spatial information techniques and spatial statistics: one 2 case study of forest fire in Margalla Hills, Islamabad, Pakistan 3 Aqil Tariq1, Hong Shu1*, Saima Siddiqui2 4 1State key laboratory of Information Engineering in Surveying, Mapping and Remote Sensing 5 (LIESMARS) Wuhan University, 430079, Wuhan, China. 6 2Department of Geography, University of the Punjab, Lahore, Pakistan. 7 8 9 10 Corresponding Authors 11 Hong Shu ([email protected] ) 12 State key laboratory of Information Engineering in Surveying, Mapping and Remote Sensing 13 (LIESMARS) Wuhan University, 430079, Wuhan, China. 14 15 Abstract 16 Background 17 Understanding the spatial patterns of forest fires is of key importance for fire risk management 18 with ecological implications. Fire occurrence, which may result from the presence of an ignition 19 source and the conditions necessary for a fire to spread, is an essential component of fire risk 20 assessment. 21 Methods 22 The aim of this research was to develop a methodology for analyzing spatial patterns of forest fire 23 danger with a case study of tropical forest fire at Margalla Hills, Islamabad, Pakistan. -

Owin, a Lost and Ruined Fortress and Defense
SECTION B Sci.Int.(Lahore),28(4),239-243,2016 ISSN 1013-5316;CODEN: SINTE 8 239 OWIN, A LOST AND RUINED FORTRESS AND DEFENSE WATCH TOWER IN KASHMIR AT THE EDGE OF PUNJAB, PAKISTAN Samina Saleem Government Post Graduate College for Women Satellite Town Rawalpindi (Sub Campus University of Gujrat) Taxila Institute of Asian Civilizations Quaid-i-Azam University Islamabad [email protected] ABSTRACT:: This research paper is a case study of a lost small fortress or watch Tower that is not documented up till now. Actually this place Owin is not even mentioned on the Archaeological map, but the link of the area tells that this area must be an ancient hidden route to Kashmir. This small building tells us the story of brutality of human, who had Sufism in their roots, but it does not show any love for humanity. The oral information about this fortress makes one to realize that, how difficult it would have been for the people of that area to build that watch tower in such a faraway place. This research also reveals the facts that how the people of that area were able to construct it with powerful material, stone, that was available in the area. It will open a window to the past when these kinsd of buildings were erected for mailing purpose or sending messages through light. The hardships that the people of this area must have faced while constructing this watch Tower can be felt. This small fortress is situated in between the rugged mountains and it is quite difficult to reach there even now after so much development. -

Ethnopharmocological Treatment of Common
112 Afr. J. Trad. CAM (2007) 4 (1): 112 - 120 Afr. J. Traditional, Complementary and Alternative Medicines Research Paper www.a f ricanethnom edicines.net ISSN 0189-6016©2007 TREATMENT OF COMMON AILMENTS BY PLANT-BASED REMEDIES AMONG THE PEOPLE OF DISTRICT ATTOCK (PUNJAB) OF NORTHERN PAKISTAN Mushtaq Ahmad, Mir Ajab Khan, Muhammad Zafar and Shazia Sultana Department of Biological Sciences, Quaid-I-Azam University, Islamabad-Pakistan 46000 E-Mail: [email protected] Abstract District Attock is one of the resource-based areas of medicinal plants in the north of Punjab province of Pakistan. The local people of the area have always used medicinal plants for their common ailments by traditional methods. Indigenous knowledge of local people about medicinal plants is directly linked to their culture and history. It is therefore felt worthwhile to record the indigenous knowledge about the plant-based remedies. The present communication deals with the common diseases treated by plant based remedies such as abdominal pain and worms, asthma, cough and bronchitis, cold, flu, influenza, diabetes, diarrheoa, dysentery, digestive disorders, ear infections and eye complaints. 25 species belonging to 25 genera were used for common ailments. It was found that plant based remedies were used in effective prescriptions, which are simple, inexpensive, and acceptable among the local inhabitants of the area. Key words: Ailments, medicinal plants, Attock, Pakistan Introduction District Attock is a famous historical region situated in the north of Punjab province of Pakistan. It acts as a gateway for the province N.W.F.P. of Pakistan. Due to its unique location, it has very useful resources of medicinal plants. -

Archaeological Potential of Capital of Pakistan-Islamabad and Pioneer Archaeological Excavation in Islamabad (Buddhist Stupa-Ban Faqiran)
Journal of the Punjab University Historical Society Volume No. 31, Issue No. 1, January - June 2018 Shahbaz Ahmad Bhatti * Abdul Ghaffar Loan** Muhammad Amir*** Archaeological potential of Capital of Pakistan-Islamabad and pioneer Archaeological Excavation in Islamabad (Buddhist Stupa-Ban Faqiran) Abstract: Modern city of Islamabad is one of the oldest living inhabitants in the world. Islamabad has the complete sequence and archaeological findings of Stone Age life showing a continuity of man in this region from the early Stone Age. Geographically, Islamabad remained the natural bearer and defensive zone of Rawalpindi against north western boarders and invaders. Buddhist site of Ban Faqiran, is the oldest historical monument discovered in Islamabad. Archaeological remains of Ban Faqiran and the oldest mosque in Islamabad are perched atop on Margalla hills. Federal Department of Archaeology and museums carried out a comprehensive and fruitful excavation at the site and exposed the buried cultural heritage of Buddhist era and a mosque of Muslim dynasty. Besides structural remains, rare copper coins, iron arrow heads and pot shreds discovered.1 Introduction of the Site Archaeological complex of Ban Faqiran, Islamabad, is at the crossed roads on one of the ancient routes, connecting the Taxila Valley with the Pothohar plateau through natural passage formed by hill torrents of Margalla mighty hills. 2 The remains of Ban Faqiran Site are situated in the Western edge of Islamabad, the capital of Pakistan. The given name, “Ban Faqiran” is derived from local vernacular; “ban” (reservoir) and “faqiran” (saints). Ban Faqiran stands for a reservoir dedicated to saints. Average height of the site from sea level is 850 meters.