Study of Lymphoedema of Non-Filarial Origin in the North West Region Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

Integrated Morbidity Management For
Lessons from the field Integrated morbidity management for lymphatic filariasis and podoconiosis, Ethiopia Kebede Deribe,a Biruck Kebede,b Mossie Tamiru,b Belete Mengistu,c Fikreab Kebede,c Sarah Martindale,d Heven Sime,e Abate Mulugeta,f Biruk Kebede,c Mesfin Sileshi,b Asrat Mengiste,g Scott McPhersonc & Amha Fentayeb Problem Lymphatic filariasis and podoconiosis are the major causes of tropical lymphoedema in Ethiopia. The diseases require a similar provision of care, but until recently the Ethiopian health system did not integrate the morbidity management. Approach To establish health-care services for integrated lymphoedema morbidity management, the health ministry and partners used existing governmental structures. Integrated disease mapping was done in 659 out of the 817 districts, to identify endemic districts. To inform resource allocation, trained health extension workers carried out integrated disease burden assessments in 56 districts with a high clinical burden. To ensure standard provision of care, the health ministry developed an integrated lymphatic filariasis and podoconiosis morbidity management guideline, containing a treatment algorithm and a defined package of care. Experienced professionals on lymphoedema management trained government-employed health workers on integrated morbidity management. To monitor the integration, an indicator on the number of lymphoedema-treated patients was included in the national health management information system. Local setting In 2014, only 24% (87) of the 363 health facilities surveyed provided lymphatic filariasis services, while 12% (44) provided podoconiosis services. Relevant changes To date, 542 health workers from 53 health centres in 24 districts have been trained on integrated morbidity management. Between July 2013 and June 2016, the national health management information system has recorded 46 487 treated patients from 189 districts. -

Podoconiosis in Ethiopia: from Neglect to Priority Public Health Problem
Podoconiosis in Ethiopia: from neglect to priority public health problem Article (Accepted Version) Deribe, Kebede, Kebede, Biruck, Mengistu, Belete, Negussie, Henok, Sileshi, Mesfin, Tamiru, Mossie, Tomezyk, Sara, Tekola-Ayele, Fasil, Davey, Gail and Fentaye, Amha (2017) Podoconiosis in Ethiopia: from neglect to priority public health problem. Ethiopian Medical Journal, 55. pp. 65-74. ISSN 0014-1755 This version is available from Sussex Research Online: http://sro.sussex.ac.uk/id/eprint/70009/ This document is made available in accordance with publisher policies and may differ from the published version or from the version of record. If you wish to cite this item you are advised to consult the publisher’s version. Please see the URL above for details on accessing the published version. Copyright and reuse: Sussex Research Online is a digital repository of the research output of the University. Copyright and all moral rights to the version of the paper presented here belong to the individual author(s) and/or other copyright owners. To the extent reasonable and practicable, the material made available in SRO has been checked for eligibility before being made available. Copies of full text items generally can be reproduced, displayed or performed and given to third parties in any format or medium for personal research or study, educational, or not-for-profit purposes without prior permission or charge, provided that the authors, title and full bibliographic details are credited, a hyperlink and/or URL is given for the original metadata page and the content is not changed in any way. http://sro.sussex.ac.uk Podoconiosis in Ethiopia: From neglect to priority public health problem KebedeDeribe1,2,3,4, Biruck Kebede1, Belete Mengistu1, Henok Negussie2, Biruk Kebede4,Mesfin Sileshi1,4 , Mossie Tamiru1, Sara Tomczyk5, Fasil Tekola-Ayele6, Gail Davey2, Amha Fentaye1 1. -

206 Villages Burnt in the North West and South West Regions
CHRDA Email: [email protected] Website: www.chrda.org Cameroon: The Anglophone Crisis 206 Villages burnt in the North West and South West Regions April 2019 SUMMARY The Center for Human Rights and Democracy in Africa (CHRDA) has analyzed data from local sources and identified 206 villages that have been partially, or completely burnt since the beginning of the immediate crisis in the Anglophone regions. Cameroon is a nation sliding into civil war in Africa. In 2016, English- speaking lawyers, teachers, students and civil society expressed “This act of burning legitimate grievances to the Cameroonian government. Peaceful protests villages is in breach of subsequently turned deadly following governments actions to prevent classical common the expression of speech and assembly. Government forces shot peaceful article 3 to the Four protesters, wounded many and killed several. Geneva Convention 1949 and the To the dismay of the national, regional and international communities, Additional Protocol II the Cameroon government began arresting activists and leaders to the same including CHRDA’s Founder and CEO, Barrister Agbor Balla, the then Convention dealing President of the now banned Anglophone Consortium. Internet was shut with the non- down for three months and all forms of dissent were stifled, forcing international conflicts. hundreds into exile. Also, the burning of In August 2017, President Paul Biya of Cameroon ordered the release of villages is in breach of several detainees, but avoided dialogue, prompting mass protests in national and September 2017 with an estimated 500,000 people on the streets of international human various cities, towns and villages. The government’s response was a rights norms and the brutal crackdown which led to a declaration of independence on October host of other laws” 1, 2017. -
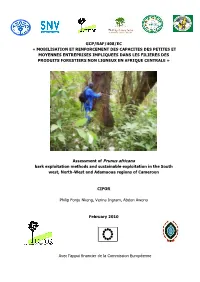
Assessment of Prunus Africana Bark Exploitation Methods and Sustainable Exploitation in the South West, North-West and Adamaoua Regions of Cameroon
GCP/RAF/408/EC « MOBILISATION ET RENFORCEMENT DES CAPACITES DES PETITES ET MOYENNES ENTREPRISES IMPLIQUEES DANS LES FILIERES DES PRODUITS FORESTIERS NON LIGNEUX EN AFRIQUE CENTRALE » Assessment of Prunus africana bark exploitation methods and sustainable exploitation in the South west, North-West and Adamaoua regions of Cameroon CIFOR Philip Fonju Nkeng, Verina Ingram, Abdon Awono February 2010 Avec l‟appui financier de la Commission Européenne Contents Acknowledgements .................................................................................................... i ABBREVIATIONS ...................................................................................................... ii Abstract .................................................................................................................. iii 1: INTRODUCTION ................................................................................................... 1 1.1 Background ................................................................................................. 1 1.2 Problem statement ...................................................................................... 2 1.3 Research questions .......................................................................................... 2 1.4 Objectives ....................................................................................................... 3 1.5 Importance of the study ................................................................................... 3 2: Literature Review ................................................................................................. -
An Under-Recognized Non-Filarial Cause of Lower Extremity Lymphedema
An under-recognized non-filarial cause of lower extremity lymphedema Angie Koriakos, DO, MPH South Texas Dermatology Residency Case A 14-year-old boy presents with bilateral lower extremity elephantiasis with lichenification of the overlying skin and a mossy appearance of the toes. The lesions began 5 years ago and were accompanied by edema and pruritus. The boy is from the Guraghe zone of Ethiopia and because of poor socioeconomic conditions has been barefoot throughout his entire life. He works in the fields and has no significant medical history. Causes of lower extremity lymphedema Deep vein thrombosis Neurofibromatosis Hypoalbuminemia Sclerema neonatorum Renal failure Idiopathic edema Lipedema Congestive heart failure Postoperative complications Venous insufficiency Baker cyst Cellulitis Differential diagnosis Lymphedema secondary to systemic disease (cardiac, renal) Vascular causes Lymphangioma Mycetoma Kaposi sarcoma Leprotic lymphedema Elephantiasis verrucosa nostra Filarial elephantiasis PODOCONIOSIS What is podoconiosis? Podoconiosis is a non-infectious, non-filarial, geochemical lymphedema Derived from Greek terms podos and konos, meaning foot and dust, respectively Elephantiasis dates back to second millennium BC. Until 1924, all forms of elephantiasis were considered infectious until the 1960’s and 1970’s, when non filarial elephantiasis in Ethiopia termed podoconiosis Affects farmers mainly in tropical parts of Africa and is caused by long term barefoot exposure to red clay soil of volcanic origin Epidemiology At least 4 million people globally with podoconiosis Affects people in more than 20 countries Tropical Africa Central and South America Northern India Countries where podoconiosis is endemic or has been described Geographical distribution of podoconiosis in Ethiopia, results from historical maps and recent surveys conducted on podoconiosis. -

Cameroon Page 1 of 27
Cameroon Page 1 of 27 Cameroon Country Reports on Human Rights Practices - 2001 Released by the Bureau of Democracy, Human Rights, and Labor March 4, 2002 Cameroon is a republic dominated by a strong presidency. Since independence a single party, now called the Cameroon People's Democratic Movement (CPDM), has remained in power. In 1997 CPDM leader Paul Biya won reelection as President in an election boycotted by the three main opposition parties, marred by a wide range of procedural flaws, and generally considered by observers not to be free and fair. The 1997 legislative elections, which were dominated by the CPDM, were flawed by numerous irregularities and generally considered not free nor fair by international and local observers. The President retains the power to control legislation or to rule by decree. In the National Assembly, government bills take precedence over other bills, and no bills other than government bills have been enacted since 1991, although the Assembly sometimes has not enacted legislation proposed by the Government. The President has used his control of the legislature to change the Constitution. The 1996 Constitution lengthened the President's term of office to 7 years, while continuing to allow Biya to run for a fourth consecutive term in 1997 and making him eligible to run for one more 7-year term in 2004. In 2000 the Government began discussion on an action plan to create the decentralized institutions envisioned in the 1996 Constitution, such as a partially elected senate, elected regional councils, and a more independent judiciary; however, none of the plans had been executed by year's end. -
Programming of Public Contracts Awards and Execution for the 2020
PROGRAMMING OF PUBLIC CONTRACTS AWARDS AND EXECUTION FOR THE 2020 FINANCIAL YEAR CONTRACTS PROGRAMMING LOGBOOK OF DEVOLVED SERVICES AND OF REGIONAL AND LOCAL AUTHORITIES NORTH-WEST REGION 2021 FINANCIAL YEAR SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of No Designation of PO/DPO Amount of Contracts No. page contracts REGIONAL 1 External Services 9 514 047 000 3 6 Bamenda City Council 13 1 391 000 000 4 Boyo Division 9 Belo Council 8 233 156 555 5 10 Fonfuka Council 10 186 760 000 6 11 Fundong Council 8 203 050 000 7 12 Njinikom Council 10 267 760 000 8 TOTAL 36 890 726 555 Bui Division 13 External Services 3 151 484 000 9 14 Elak-Oku Council 6 176 050 000 9 15 Jakiri Council 10 266 600 000 10 16 Kumbo Council 5 188 050 000 11 17 Mbiame Council 6 189 050 000 11 18 Nkor Noni Council 9 253 710 000 12 19 Nkum Council 8 295 760 002 13 TOTAL 47 1 520 704 002 Donga Mantung Division 20 External Services 1 22 000 000 14 21 Ako Council 8 205 128 308 14 22 Misaje Council 9 226 710 000 15 23 Ndu Council 6 191 999 998 16 24 Nkambe Council 14 257 100 000 16 25 Nwa Council 10 274 745 452 18 TOTAL 48 1 177 683 758 Menchum Division 27 Furu Awa Council 4 221 710 000 19 28 Benakuma Council 9 258 760 000 19 29 Wum Council 7 205 735 000 20 30 Zhoa Council 5 184 550 000 21 TOTAL 25 870 755 000 MINMAP/Public Contracts Programming and Monitoring Division Page 1 of 37 SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of No Designation of PO/DPO Amount of Contracts No. -

Defining and Managing Acute Lymphangioadenitis in Podoconiosis Lymphoedema in Northern Ethiopia
DEFINING AND MANAGING ACUTE LYMPHANGIOADENITIS IN PODOCONIOSIS LYMPHOEDEMA IN NORTHERN ETHIOPIA HENOK NEGUSSIE SEIFU PhD 2017 1 DEFINING AND MANAGING ACUTE LYMPHANGIOADENITIS IN PODOCONIOSIS LYMPHOEDEMA IN NORTHERN ETHIOPIA HENOK NEGUSSIE SEIFU A thesis submitted in partial fulfillment of the requirements of the University of Brighton and the University of Sussex for a programme of study undertaken at Brighton and Sussex Medical School for the degree of Doctor of Philosophy JULY, 2017 2 This thesis was supervised by Prof Gail Davey, Professor of Global Health Epidemiology, Brighton and Sussex Medical Scholl, UK Prof. Melanie Newport, Professor of Global Health and Infection, Brighton and Sussex Medical Scholl, UK Prof Fikre Enquselassie, Professor of Epidemiology and Biostatistics, College of Medicine and Health Sciences, Addis Ababa, University 3 Abstract Podoconiosis (endemic non-filarial elephantiasis) is a non-infectious disease arising in barefoot individuals in long-term contact with irritant red clay soil of volcanic origin. The condition is believed to be caused by the interplay between environmental factors and genetic susceptibility over a prolonged period of time. In the last decade significant progress had been made in research on podoconiosis. Acute dermatolymphangioadenitis (ADLA) is a common and disabling complication of podoconiosis lymphoedema and remain the most painful and distressing condition, with diverse health, social and economic ramifications, yet has been very little investigated to date. This PhD thesis is therefore, aimed at defining ADLA, validating this to measure the impact of ADLA, and to document the impact of a simple foot hygiene intervention on ADLA and quality of life among podoconiosis patients. The study utilized several steps. -

Establishing Rights and Duties in the Prevention And
HHr Health and Human Rights Journal A Human Right to Shoes? Establishing RightsHHR_final_logo_alone.indd 1 10/19/15 10:53 AM and Duties in the Prevention and Treatment of Podoconiosis arianne shahvisi, enguday meskele, and gail davey Abstract Podoconiosis is a debilitating chronic swelling of the foot and lower leg caused by long-term exposure to irritant red volcanic clay soil in the highland regions of Africa, Central America, and India. In this paper, we consider the human rights violations that cause, and are caused by, podoconiosis in Ethiopia. Specifically, we discuss the way in which the right to an adequate basic standard of living is not met in endemic regions, where the following basic necessities are not readily available: appropriate footwear, health education, and affordable, accessible health care. Those living with podoconiosis experience disablement, stigma and discrimination, and mental distress, contributing to greater impoverishment and a reduced quality of life. We suggest that while identifying rights violations is key to characterizing the scale and nature of the problem, identifying duties is critical to eliminating podoconiosis. To this end, we describe the duties of the Ethiopian government, the international community, and those sourcing Ethiopian agricultural products in relation to promoting shoe-wearing, providing adequate health care, and improving health literacy. Arianne Shahvisi is a lecturer in ethics and medical humanities at Brighton and Sussex Medical School, Brighton, UK. Enguday Meskele is a lecturer in human rights law at Wolaita Sodo University, Ethiopia. Gail Davey is a professor of global health epidemiology at Brighton and Sussex Centre for Global Health Research, Brighton, UK. -

Proceedingsnord of the GENERAL CONFERENCE of LOCAL COUNCILS
REPUBLIC OF CAMEROON REPUBLIQUE DU CAMEROUN Peace - Work - Fatherland Paix - Travail - Patrie ------------------------- ------------------------- MINISTRY OF DECENTRALIZATION MINISTERE DE LA DECENTRALISATION AND LOCAL DEVELOPMENT ET DU DEVELOPPEMENT LOCAL Extrême PROCEEDINGSNord OF THE GENERAL CONFERENCE OF LOCAL COUNCILS Nord Theme: Deepening Decentralization: A New Face for Local Councils in Cameroon Adamaoua Nord-Ouest Yaounde Conference Centre, 6 and 7 February 2019 Sud- Ouest Ouest Centre Littoral Est Sud Published in July 2019 For any information on the General Conference on Local Councils - 2019 edition - or to obtain copies of this publication, please contact: Ministry of Decentralization and Local Development (MINDDEVEL) Website: www.minddevel.gov.cm Facebook: Ministère-de-la-Décentralisation-et-du-Développement-Local Twitter: @minddevelcamer.1 Reviewed by: MINDDEVEL/PRADEC-GIZ These proceedings have been published with the assistance of the German Federal Ministry for Economic Cooperation and Development (BMZ) through the Deutsche Gesellschaft für internationale Zusammenarbeit (GIZ) GmbH in the framework of the Support programme for municipal development (PROMUD). GIZ does not necessarily share the opinions expressed in this publication. The Ministry of Decentralisation and Local Development (MINDDEVEL) is fully responsible for this content. Contents Contents Foreword ..............................................................................................................................................................................5 -

The Fulani Problem in the North West Region of Cameroon
THE FULANI PROBLEM IN THE NORTH WEST REGION OF CAMEROON 1 Contents EXECUTIVE SUMMARY .................................................................................................................. 3 GENESIS OF THE PROBLEM .......................................................................................................... 4 THE OUTBREAK OF THE ANGLOPHONE CRISIS .................................................................... 6 SEPARATIST ATTACKS ON MINORITY MBOROROS ............................................................. 7 THE FULANI RAIDS AGAINST THE NATIVES IN NWA SUB DIVISION ............................. 10 THE ATTACKS IN FIGURES .......................................................................................................... 12 FULANI ATTACKS IN BUM ........................................................................................................... 14 SUMMARY AND CONCLUSION.................................................................................................... 15 RECOMMENDATIONS .................................................................................................................... 16 2 EXECUTIVE SUMMARY This report is a detailed research work analyzing the Fulani problem in the North West Region, with particular reference to the recent violence in Nwa Subdivision, Donga-Mantung Division, which has seen many lives lost and much property destroyed, as well as displacement of the natives in Nwa. Similar violence has been recorded in Bum Subdivision, situated in Boyo Division