To Reduce the Global Burden of Human Schistosomiasis, Use 'Old Fashioned' Snail Control
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of Reviewers (As Per the Published Articles) Year: 2019
List of Reviewers (as per the published articles) Year: 2019 South Asian Journal of Research in Microbiology 2019 - Volume 3 [Issue 1] In vitro Antibacterial Efficacy of Bryophyllum pinnatum Leaf Extracts DOI: 10.9734/SAJRM/2019/v3i130075 (1) Oshim, Ifeanyi Onyema, Nnamdi Azikiwe University, Nigeria. (2) Shibabrata Pattanayak, India. Complete Peer review History: http://www.sdiarticle3.com/review-history/46584 Production of Plant Growth Regulators by Some Fungi Isolated under Salt Stress DOI: 10.9734/SAJRM/2019/v3i130076 (1) Toshik Iarley da Silva, Federal University of Viçosa, Brazil. (2) Toungos, Mohammed Dahiru, Adamawa State University Mubi, Nigeria. Complete Peer review History: http://www.sdiarticle3.com/review-history/46911 Biosynthesis and Characterization of Silver Nanoparticles Produced by Plant Extracts and Its Antimicrobial Activity DOI: 10.9734/SAJRM/2019/v3i130077 (1) Nguyen Thi Hieu Trang, Vietnam. (2) Ajoy Kumer, European University of Bangladesh, Bangladesh. (3) Tahmina Monowar, AIMST University, Malaysia. Complete Peer review History: http://www.sdiarticle3.com/review-history/46186 Microbiological and Physiochemical Quality of Freshwater in Isiokpo Community, Rivers State, Nigeria DOI: 10.9734/SAJRM/2019/v3i130078 (1) Yongchun Zhu, Shenyang Normal University, China. (2) Prof. Graciela Pucci, Argentina. Complete Peer review History: http://www.sdiarticle3.com/review-history/47362 Microbiological and Proximate Analyses of Lebanese Bread (Pita) from Akure Metropolis DOI: 10.9734/SAJRM/2019/v3i130079 (1) C. E. Oshoma, University of Benin, Nigeria. (2) H. A. Rathnayake, University of Sri Jayewardenepura, Sri Lanka. (3) P. Saravana Kumari, Rathnavel Subramaniam College of Arts and Science, India. Complete Peer review History: http://www.sdiarticle3.com/review-history/47284 2019 - Volume 3 [Issue 2] Antibacterial Activity of Zingiber officinale (Ginger) against Clinical Bacterial Isolates DOI: 10.9734/SAJRM/2019/v3i230080 (1) Evbuomwan Lucky, University of Benein, Nigeria. -

Historical Biogeography and Phylogeography of Indoplanorbis Exustus
bioRxiv preprint doi: https://doi.org/10.1101/2021.05.28.446081; this version posted May 30, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Historical biogeography and phylogeography of Indoplanorbis exustus Maitreya Sil1*, Juveriya Mahveen1,2, Abhishikta Roy1,3, K. Praveen Karanth4, and Neelavara Ananthram Aravind1,5* 1 Suri Sehgal Centre for Biodiversity and Conservation, Ashoka Trust For Research In Ecology And The Environment, Royal Enclave, Sriramapura, Jakkur PO, Bangalore 560064, India 2The Department of Microbiology, St. Joseph’s College, Bangalore 560027, India 3The University of Trans-Disciplinary Health Sciences and Technology, Jarakbande Kaval, Bangalore 560064, India 4 Centre for Ecological Sciences, Indian Institute of science, Bangalore 560012, India 5Yenepoya Research Centre, Yenepoya (Deemed to be University), University Road, Derlakatte, Mangalore 575018, India *Author for correspondence [email protected] [email protected] Abstract: The history of a lineage is intertwined with the history of the landscape it resides in. Here we showcase how the geo-tectonic and climatic evolution in South Asia and surrounding landmasses have shaped the biogeographic history of Indoplanorbis exustus, a tropical Asian, freshwater, pulmonated snail. We amplified partial COI gene fragment from all over India and combined this with a larger dataset from South and Southeast Asia to carry out phylogenetic reconstruction, species delimitation analysis, and population genetic analyses. Two nuclear genes were also amplified from one individual per putative species to carry out divergence dating and ancestral area reconstruction analyses. -

In Bahia, Brazil
Volume 52(40):515‑524, 2012 A NEW GENUS AND SPECIES OF CAVERNICOLOUS POMATIOPSIDAE (MOLLUSCA, CAENOGASTROPODA) IN BAHIA, BRAZIL 1 LUIZ RICARDO L. SIMONE ABSTRACT Spiripockia punctata is a new genus and species of Pomatiopsidae found in a cave from Serra Ramalho, SW Bahia, Brazil. The taxon is troglobiont (restricted to subterranean realm), and is characterized by the shell weakly elongated, fragile, translucent, normally sculptured by pus‑ tules with periostracum hair on tip of pustules; peristome highly expanded; umbilicus opened; radular rachidian with 6 apical and 3 pairs of lateral cusps; osphradium short, arched; gill filaments with rounded tip; prostate flattened, with vas deferens inserting subterminally; penis duct narrow and weakly sinuous; pallial oviduct simple anteriorly, possessing convoluted by‑ pass connecting base of bulged portion of transition between visceral and pallial oviducts with base of seminal receptacle; spermathecal duct complete, originated from albumen gland. The description of this endemic species may raise protective environmental actions to that cave and to the Serra Ramalho Karst area. Key-Words: Pomatiopsidae; Spiripockia punctata gen. nov. et sp. nov.; Brazil; Cave; Tro- globiont; Anatomy. INTRODUCTION An enigmatic tiny gastropod has been collected in caves from the Serra Ramalho Kars area, southwestern The family Pomatiopsidae is represented in the Bahia state, Brazil. It has a pretty, fragile, translucent Brazilian region by only two species of the genus Id‑ shell in such preliminary gross anatomy, which already iopyrgus Pilsbry, 1911 (Simone, 2006: 94). However, reveals troglobiont adaptations, i.e., depigmentation, the taxon is much richer in remaining mainland ar- lack of eyes and small size. The sample has been brought eas, with both freshwater and semi-terrestrial habits by Maria Elina Bichuette, who is specialized in subter- (Ponder & Keyzer, 1998; Kameda & Kato, 2011). -

Mitochondrial Genome of Bulinus Truncatus (Gastropoda: Lymnaeoidea): Implications for Snail Systematics and Schistosome Epidemiology
Journal Pre-proof Mitochondrial genome of Bulinus truncatus (Gastropoda: Lymnaeoidea): implications for snail systematics and schistosome epidemiology Neil D. Young, Liina Kinkar, Andreas J. Stroehlein, Pasi K. Korhonen, J. Russell Stothard, David Rollinson, Robin B. Gasser PII: S2667-114X(21)00011-X DOI: https://doi.org/10.1016/j.crpvbd.2021.100017 Reference: CRPVBD 100017 To appear in: Current Research in Parasitology and Vector-Borne Diseases Received Date: 21 January 2021 Revised Date: 10 February 2021 Accepted Date: 11 February 2021 Please cite this article as: Young ND, Kinkar L, Stroehlein AJ, Korhonen PK, Stothard JR, Rollinson D, Gasser RB, Mitochondrial genome of Bulinus truncatus (Gastropoda: Lymnaeoidea): implications for snail systematics and schistosome epidemiology, CORTEX, https://doi.org/10.1016/ j.crpvbd.2021.100017. This is a PDF file of an article that has undergone enhancements after acceptance, such as the addition of a cover page and metadata, and formatting for readability, but it is not yet the definitive version of record. This version will undergo additional copyediting, typesetting and review before it is published in its final form, but we are providing this version to give early visibility of the article. Please note that, during the production process, errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. © 2021 The Author(s). Published by Elsevier B.V. Journal Pre-proof Mitochondrial genome of Bulinus truncatus (Gastropoda: Lymnaeoidea): implications for snail systematics and schistosome epidemiology Neil D. Young a,* , Liina Kinkar a, Andreas J. Stroehlein a, Pasi K. Korhonen a, J. -

Healthy Planet, Healthy People Guide
HEALTHY PLANET, HEALTHY PEOPLE A Guide to Human Health and Biodiversity UNEP, 2011-2012 declared “Year of the Bat” Bats provide a range of biodiversity benefits to humans … New drug synthesized from vampire bat saliva in development … Could help stroke victims … SAN FRANCISCO, Sep. 6, 2012 … Yosemite National Park … hantavirus warning … 22,000 visitors may have been exposed to deadly mouse-borne disease … confirmed cases growing “Healthy people are better able to learn, be productive and contribute to their communities. At the same time, a healthy environment is a prerequisite for good health.” Dr. Margaret Chan, Director-General of the World Health Organization, 22 June 2012 Healthy Planet Healthy People: A Guide to Human Health and Biodiversity (This page is intentionally left blank) Citation: It is suggested this Guide be cited as: Bridgewater, Peter; Régnier, Mathieu; and Wang Zhen. (2012). HEALTHY PLANET, HEALTHY PEOPLE ‐ A Guide to Human Health and Biodiversity. Secretariat of the Convention on Biological Diversity, Montreal. ACKOWLEDGEMENTS: Alice Barbe, Kathryn Campbell, David Cooper and a number of reviewers who all provided helpful comments and examples. Photo credits (alphabetical order of photographer): P39 bushmeat picture © E.Bennett/WCS, 2009 P47 © Boréalis, 2009 P29, 56, 60, 61 © Peter Bridgewater P39 H5N1 virus © Centre for Disease Control and Prevention, United States of America Government P9, 48, 52 © Christine Estrada P13, 15, 30, 52,58 (marine fresco) © Mathieu Régnier P58 © Urbainculteurs, 2012 The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the Convention on Biological Diversity concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

Aflenz Basin, Eastern Alps, Austria
Pala¨ontol Z DOI 10.1007/s12542-011-0117-x RESEARCH PAPER A Middle Miocene endemic freshwater mollusc assemblage from an intramontane Alpine lake (Aflenz Basin, Eastern Alps, Austria) Mathias Harzhauser • Thomas A. Neubauer • Oleg Mandic • Martin Zuschin • Stjepan C´ oric´ Received: 18 February 2011 / Accepted: 11 August 2011 Ó Springer-Verlag 2011 Abstract The mollusc fauna of the early Middle Miocene roetzeli Harzhauser and Neubauer nov. sp., Nematurella (Langhian) intramontane Alpine Lake Groisenbach is zuschini Neubauer and Harzhauser nov. sp., Romania described for the first time. The shells derive from the fastigata Neubauer and Harzhauser nov. sp., Odontohy- Feistring Formation in the Aflenz Basin in Austria, which drobia groisenbachensis Neubauer and Harzhauser nov. sp., was covered by Lake Groisenbach. The assemblage is Odontohydrobia pompatica Neubauer and Harzhauser nov. moderately diverse with 12 gastropod and 2 bivalve species, sp., Odontohydrobia styriaca Harzhauser and Neubauer nov. suggesting shallow lacustrine and fluvial settings. Among sp., Planorbis austroalpinus Harzhauser and Neubauer the gastropods, only Theodoxus crenulatus (Klein, 1853) is nov. sp., Gyraulus sachsenhoferi Harzhauser and Neubauer known from other Miocene localities, whilst all other spe- nov. sp., Bulinus corici Harzhauser and Neubauer nov. sp., cies are documented so far only from Lake Groisenbach. Ferrissia crenellata Harzhauser and Neubauer nov. sp. and None of the Early and Middle Miocene lake systems of the Stagnicola reinholdkunzi Harzhauser and Neubauer nov. Alpine-Carpathian Foredeep and the Balkan Peninsula sp. are introduced as new species. displays any faunistic resemblance with this new fauna. Even coeval lake faunas from the close-by Graz Basin have Keywords Gastropoda Á Miocene Á Freshwater Á no species in common with Lake Groisenbach. -

University of Copenhagen, Denmark
A one health approach to reducing schistosomiasis transmission in Lake Malawi Stauffer, Jr., Jay Richard; Madsen, Henry Published in: Preventive Medicine and Community Health DOI: 10.15761/PMCH.1000115 Publication date: 2018 Document version Publisher's PDF, also known as Version of record Document license: CC BY Citation for published version (APA): Stauffer, Jr., J. R., & Madsen, H. (2018). A one health approach to reducing schistosomiasis transmission in Lake Malawi. Preventive Medicine and Community Health, 1(3), 1-4. https://doi.org/10.15761/PMCH.1000115 Download date: 01. Oct. 2021 Preventive Medicine and Community Health Research Article ISSN: 2516-7073 A one health approach to reducing schistosomiasis transmission in Lake Malawi Jay Richard Stauffer1,2* and Henry Madsen3 1Forest Resources Building, Penn State University, University Park, USA 2South African Institute for Aquatic Biodiversity, Grahamstown, South Africa 3Faculty of Health and Medical Sciences, University of Copenhagen, Denmark Abstract Objective: To review what we know about urinary schistosomiasis in Lake Malawi and summarize our attempts to use fishes as a biological control of the intermediate hosts. Conclusions: A One Health approach must be employed to effectively control urinary schistosomiasis in Lake Malawi. Health clinics must be supplied with praziquantel for distribution. Education centers must emphasize the need for sanitation and clearly state precautions (e.g., avoid swimming between 1000-1500). Additionally, the importance of snail-eating fishes to control the intermediate hosts must be emphasized. If biological controls are to be implemented, alternate food sources (agriculture, aquaculture) must be made available. A true One Health approach must be utilized to effectively control the transmission of schistosomiasis along the lake shores of Lake Malawi. -
Freshwater Snail Guide
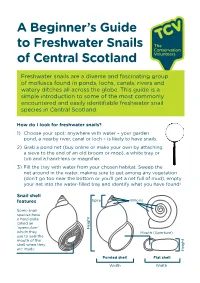
A Beginner’s Guide to Freshwater Snails of Central Scotland Freshwater snails are a diverse and fascinating group of molluscs found in ponds, lochs, canals, rivers and watery ditches all across the globe. This guide is a simple introduction to some of the most commonly encountered and easily identifiable freshwater snail species in Central Scotland. How do I look for freshwater snails? 1) Choose your spot: anywhere with water – your garden pond, a nearby river, canal or loch – is likely to have snails. 2) Grab a pond net (buy online or make your own by attaching a sieve to the end of an old broom or mop), a white tray or tub and a hand-lens or magnifier. 3) Fill the tray with water from your chosen habitat. Sweep the net around in the water, making sure to get among any vegetation (don’t go too near the bottom or you’ll get a net full of mud), empty your net into the water-filled tray and identify what you have found! Snail shell features Spire Whorls Some snail species have a hard plate called an ‘operculum’ Height which they Mouth (Aperture) use to seal the mouth of the shell when they are inside Height Pointed shell Flat shell Width Width Pond Snails (Lymnaeidae) Variable in size. Mouth always on right-hand side, shells usually long and pointed. Great Pond Snail Common Pond Snail Lymnaea stagnalis Radix balthica Largest pond snail. Common in ponds Fairly rounded and ’fat’. Common in weedy lakes, canals and sometimes slow river still waters. pools. -

Pomacea Canaliculata) Behaviors in Different Water Temperature Gradients
water Article Comparison of Invasive Apple Snail (Pomacea canaliculata) Behaviors in Different Water Temperature Gradients Mi-Jung Bae 1, Eui-Jin Kim 1 and Young-Seuk Park 2,* 1 Nakdonggang National Institute of Biological Resources, Sangju 37242, Korea; [email protected] (M.-J.B.); [email protected] (E.-J.K.) 2 Department of Biology, Kyung Hee University, Dongdaemun, Seoul 02447, Korea * Correspondence: [email protected]; Tel.: +82-2-961-0946 Abstract: Pomacea canaliculata (known as invasive apple snail) is a freshwater snail native to South America that was introduced into many countries (including Asia and North America) as a food source or for organic farming systems. However, it has invaded freshwater ecosystems and become a serious agricultural pest in paddy fields. Water temperature is an important factor determining behavior and successful establishment in new areas. We examined the behavioral responses of P. canaliculata with water temperature changes from 25 ◦C to 30 ◦C, 20 ◦C, and 15 ◦C by quantifying changes in nine behaviors. At the acclimated temperature (25 ◦C), the mobility of P. canaliculata was low during the day, but high at night. Clinging behavior increased as the water temperature decreased from 25 ◦C to 20 ◦C or 15 ◦C. Conversely, ventilation and food consumption increased when the water temperature increased from 25 ◦C to 30 ◦C. A self-organizing map (an unsupervised artificial neural network) was used to classify the behavioral patterns into seven clusters at different water temperatures. These results suggest that the activity levels or certain behaviors of P. canaliculata vary with the water temperature conditions. -

Gastropoda: Physidae) in Singapore
BioInvasions Records (2015) Volume 4, Issue 3: 189–194 Open Access doi: http://dx.doi.org/10.3391/bir.2015.4.3.06 © 2015 The Author(s). Journal compilation © 2015 REABIC Research Article Clarifying the identity of the long-established, globally-invasive Physa acuta Draparnaud, 1805 (Gastropoda: Physidae) in Singapore Ting Hui Ng1,2*, Siong Kiat Tan3 and Darren C.J. Yeo1,2 1Department of Biological Sciences, National University of Singapore 14 Science Drive 4, Singapore 117543, Republic of Singapore 2NUS Environmental Research Institute, National University of Singapore, 5A Engineering Drive 1, #02-01, Singapore 117411, Republic of Singapore 3Lee Kong Chian Natural History Museum, National University of Singapore, 2 Conservatory Drive, Singapore 117377, Republic of Singapore E-mail: [email protected] (THN), [email protected] (SKT), [email protected] (DCJY) *Corresponding author Received: 24 December 2014 / Accepted: 6 May 2015 / Published online: 2 June 2015 Handling editor: Vadim Panov Abstract The freshwater snail identified as Physastra sumatrana has been recorded in Singapore since the late 1980’s. It is distributed throughout the island and commonly associated with ornamental aquatic plants. Although the species has previously been considered by some to be native to Singapore, its origin is currently categorised as unknown. Morphological comparisons of freshly collected specimens and material in museum collections with type material, together with DNA barcoding, show that both Physastra sumatrana, and a recent gastropod record of Stenophysa spathidophallus, in Singapore are actually the same species—the globally-invasive Physa acuta. An unidentified physid snail was also collected from the Singapore aquarium trade. -

Laboratory Feeding of Bulinus Truncatus and Bulinus Globosus with Tridax Procumbens Leaves
Vol. 5(3), pp. 31-35, March 2013 DOI: 10.5897/JPVB 13.0109 Journal of Parasitology and ISSN 2141-2510 © 2013 Academic Journals http://www.academicjournals.org/JPVB Vector Biology Full Length Research Paper Laboratory feeding of Bulinus truncatus and Bulinus globosus with Tridax procumbens leaves O. M. Agbolade*, O. W. Lawal and K. A. Jonathan Department of Plant Science and Applied Zoology, Parasitology and Medical Entomology Laboratory, Olabisi Onabanjo University, P.M.B. 2002, Ago-Iwoye, Ogun State, Nigeria. Accepted 18 March, 2013 Suitability of Tridax procumbens leaves in laboratory feeding of Bulinus truncatus and Bulinus globosus was assessed in comparison with Lactuca sativa between September and October, 2011. The snails were collected from Eri-lope stream in Ago-Iwoye, while T. procumbens were collected from the Mini Campus of the Olabisi Onabanjo University, Ago-Iwoye, Ijebu North, Southwestern Nigeria. For B. truncatus, fresh, sun-dried and oven-dried T. procumbens were used, while only fresh T. procumbens were used for B. globosus. The mean percentage survivals of B. truncatus fed with fresh, sun-dried and oven-dried T. procumbens compared with those of the corresponding control snails showed no significant difference (2 = 0.51, 1.85, and 2.21, respectively). B. truncatus fed with fresh T. procumbens had the highest mean live-weight percentage increase (46.4%) as compared to those fed with sun-dried and oven-dried (2 = 45.65). The mean percentage survival of B. globosus fed with fresh T. procumbens (79.2%) was similar with that of the control (84.6%) (2 = 0.18). -

Abstract Volume
ABSTRACT VOLUME August 11-16, 2019 1 2 Table of Contents Pages Acknowledgements……………………………………………………………………………………………...1 Abstracts Symposia and Contributed talks……………………….……………………………………………3-225 Poster Presentations…………………………………………………………………………………226-291 3 Venom Evolution of West African Cone Snails (Gastropoda: Conidae) Samuel Abalde*1, Manuel J. Tenorio2, Carlos M. L. Afonso3, and Rafael Zardoya1 1Museo Nacional de Ciencias Naturales (MNCN-CSIC), Departamento de Biodiversidad y Biologia Evolutiva 2Universidad de Cadiz, Departamento CMIM y Química Inorgánica – Instituto de Biomoléculas (INBIO) 3Universidade do Algarve, Centre of Marine Sciences (CCMAR) Cone snails form one of the most diverse families of marine animals, including more than 900 species classified into almost ninety different (sub)genera. Conids are well known for being active predators on worms, fishes, and even other snails. Cones are venomous gastropods, meaning that they use a sophisticated cocktail of hundreds of toxins, named conotoxins, to subdue their prey. Although this venom has been studied for decades, most of the effort has been focused on Indo-Pacific species. Thus far, Atlantic species have received little attention despite recent radiations have led to a hotspot of diversity in West Africa, with high levels of endemic species. In fact, the Atlantic Chelyconus ermineus is thought to represent an adaptation to piscivory independent from the Indo-Pacific species and is, therefore, key to understanding the basis of this diet specialization. We studied the transcriptomes of the venom gland of three individuals of C. ermineus. The venom repertoire of this species included more than 300 conotoxin precursors, which could be ascribed to 33 known and 22 new (unassigned) protein superfamilies, respectively. Most abundant superfamilies were T, W, O1, M, O2, and Z, accounting for 57% of all detected diversity.