The Urinary System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
2 Surgical Anatomy
2 Surgical Anatomy Nancy Dugal Perrier, Michael Sean Boger contents 2.2 Morphology 2.1 Introduction . 7 The paired retroperitoneal adrenal glands are found 2.2 Morphology ...7 in the middle of the abdominal cavity, residing on 2.3 Relationship of the Adrenal Glands to the Kidneys ...10 the superior medial aspect of the upper pole of each 2.4 Blood Supply, Innervation, and Lymphatics ...10 kidney (Fig. 1). However, this location may vary 2.4.1 Arterial . 10 depending on the depth of adipose tissue.By means of 2.4.2 Venous ...10 pararenal fat and perirenal fascia,the adrenals contact 2.4.3 Innervation ...11 the superior portion of the abdominal wall. These 2.4.4 Lymphatic . 11 structures separate the adrenals from the pleural re- 2.5 Left Adrenal Gland Relationships ...11 flection, ribs, and the subcostal, sacrospinalis, and 2.6 Right Adrenal Gland Relationships ...14 latissimus dorsi muscles [2].Posteriorly,the glands lie 2.7 Summary ...17 References . 17 near the diaphragmatic crus and arcuate ligament [10]. Laterally, the right adrenal resides in front of the 12th rib and the left gland is in front of the 11th and 12th ribs [2]. Each adrenal gland weighs approximately 2.1 Introduction Liver Adrenal gland The small paired adrenal glands have a grand history. Eustachius published the first anatomical drawings of the adrenal glands in the mid-sixteenth century [17].In 1586, Piccolomineus and Baunin named them the suprarenal glands. Nearly two-and-a-half centuries later, Cuvier described the anatomical division of each gland into the cortex and medulla. -

Anatomical Variations in the Arterial Supply of the Suprarenal Gland. Int J Health Sci Res
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Anatomical Variations in the Arterial Supply of the Suprarenal Gland Sushma R.K1, Mahesh Dhoot2, Hemant Ashish Harode2, Antony Sylvan D’Souza3, Mamatha H4 1Lecturer, 2Postgraduate, 3Professor & Head, 4Assistant Professor; Department of Anatomy, Kasturba Medical College, Manipal University, Manipal-576104, Karnataka, India. Corresponding Author: Mamatha H Received: 29/03//2014 Revised: 17/04/2014 Accepted: 21/04/2014 ABSTRACT Introduction: Suprarenal gland is normally supplied by superior, middle and inferior suprarenal arteries which are the branches of inferior phrenic, abdominal aorta and renal artery respectively. However the arterial supply of the suprarenal gland may show variations. Therefore a study was conducted to find the variations in the arterial supply of Suprarenal Gland. Materials and methods: 20 Formalin fixed cadavers, were dissected bilaterally in the department of Anatomy, Kasturba Medical College, Manipal to study the arterial supply of the suprarenal gland, which were photographed and different variations were noted. Results: Out of 20 cadavers variations were observed in five cases in the arterial pattern of supra renal gland. We found that in one cadaver superior supra renal artery on the left side was arising directly from the coeliac trunk. Another variation was observed on the right side ina cadaver that inferior and middle suprarenal arteries were arising from accessory renal artery and on the right side it gave another small branch to the gland. Conclusion: Variations in the arterial pattern of suprarenal gland are significant for radiological and surgical interventions. KEY WORDS: Suprarenal gland, suprarenal artery, renal artery, abdominal aorta, inferior phrenic artery INTRODUCTION accessory renal arteries (ARA). -

Kidney, Renal Tubule – Dilation
Kidney, Renal Tubule – Dilation Figure Legend: Figure 1 Kidney, Renal tubule - Dilation in a male B6C3F1 mouse from a chronic study. Dilated tubules are noted as tracts running through the cortex and outer medulla. Figure 2 Kidney, Renal tubule - Dilation in a male F344/N rat from a chronic study. Tubule dilation is present throughout the outer stripe of the outer medulla, extending into the cortex. Figure 3 Kidney, Renal tubule - Dilation in a male B6C3F1 mouse from a chronic study. Slight tubule dilation is associated with degeneration and necrosis. Figure 4 Kidney, Renal tubule - Dilation in a male F344/N rat from a chronic study. Tubule dilation is associated with chronic progressive nephropathy. Comment: Renal tubule dilation may occur anywhere along the nephron or collecting duct system. It may occur in focal areas or as tracts running along the entire length of kidney sections (Figure 1). 1 Kidney, Renal Tubule – Dilation Renal tubule dilation may occur from xenobiotic administration, secondary mechanisms, or an unknown pathogenesis (see Kidney – Nephropathy, Obstructive (Figure 2). Dilation may result from direct toxic injury to the tubule epithelium interfering with absorption and secretion (Figure 3). It may also occur secondary to renal ischemia or from prolonged diuresis related to drug administration. Secondary mechanisms of tubule dilation may result from lower urinary tract obstruction, the deposition of tubule crystals, interstitial inflammation and/or fibrosis, and chronic progressive nephropathy (Figure 4). A few dilated tubules may be regarded as normal histologic variation. Recommendation: Renal tubule dilation should be diagnosed and given a severity grade. The location of tubule dilation should be included in the diagnosis as a site modifier. -

Adrenal Metastasis from an Esophageal Squamous Cell Carcinoma - a Case Report and Review of Literature
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 15, Issue 10 Ver. VII (October. 2016), PP 20-22 www.iosrjournals.org Adrenal Metastasis from an Esophageal Squamous Cell Carcinoma - A Case Report and Review of Literature Prof. Subbiah Shanmugam MS Mch1, Dr Sujay Susikar MS Mch2, Dr. H Prasanna Srinivasa Rao Mch Post Graduate2 1,2Department Of Surgical Oncology, Centre For Oncology, Government Royapettah Hospital & Kilpauk Medical College, Chennai, India Abstract: Adrenal metastasis from esophageal carcinoma is quite uncommon. The identification of adrenal metastasis and their differentiation from incidentally detected benign adrenal tumors is challenging especially when functional imaging facilities are unavailable. Here we present a case report of a 43 year old male presenting with adrenal metastasis from an esophageal squamous cell carcinoma. The use of minimally invasive surgery to confirm the metastatic nature of disease in a resource limited setup has been described. Keywords: adrenal metastasis, adrenalectomy, esophageal squamous cell carcinoma I. Introduction Adrenal metastases have been reported in various malignancies; most commonly from cancers of lung, breast but uncommonly from esophageal primary. The diagnostic difficulties in the identification of adrenal secondaries are due to the small size of the lesion, difficulty in differentiating benign from malignant adrenal lesions based on computed tomography findings alone and the anatomical position of adrenal making it difficult to target for biopsy under image guidance. The functional scans (PET CT) not only reliably differentiate metastatic adrenal lesions, but also light up other areas of metastasis. Such information is definitely needed before deciding on the intent of treatment and the surgery for the primary lesion. -

Female Urethra
OBJECTIVES: • By the end of this lecture, student should understand the anatomical structure of urinary system. General Information Waste products of metabolism are toxic (CO2, ammonia, etc.) Removal from tissues by blood and lymph Removal from blood by Respiratory system And Urinary system Functions of the Urinary System Elimination of waste products Nitrogenous wastes Toxins Drugs Functions of the Urinary System Regulate homeostasis Water balance Acid-base balance in the blood Electrolytes Blood pressure Organs of the Urinary system Kidneys Ureters Urinary bladder Urethra Kidneys Primary organs of the urinary system Located between the 12th thoracic and 3rd lumbar vertebrae. Right is usually lower due to liver. Held in place by connective tissue [renal fascia] and surrounded by thick layer of adipose [perirenal fat] Each kidney is approx. 3 cm thick, 6 cm wide and 12 cm long Regions of the Kidney Renal cortex: outer region Renal medulla: pyramids and columns Renal pelvis: collecting system Kidneys protected by three connective tissue layers Renal fascia -Attaches to abdominal wall Renal capsule: -Surrounds each kidney -Fibrous sac -Protects from trauma and infection Adipose capsule -Fat cushioning kidney Nephrons Each kidney contains over a million nephrons [functional structure] • Blood enters the nephron from a network that begins with the renal artery. • This artery branches into smaller and smaller vessels and enters each nephron as an afferent arteriole. • The afferent arteriole ends in a specialized capillary called the Glomerulus. • Each kidney has a glomerulus contained in Bowman’s Capsule. • Any cells that are too large to pass into the nephron are returned to the venous blood supply via the efferent arteriole. -

The Human Body Systems for Kids
1 Maine Regional School Unit #67 Chester, Lincoln, Mattawamkeag The Human Body Systems for Kids KidsKonnect.com and kidshealth.org provide links to more detailed information about each of the systems listed below. The first group of systems are commonly taught in the elementary grades. Teachers wishing more detailed information should consult sources beyond this handout. There are many systems in the human body. • Skeletal System (bones) • Respiratory System (nose, trachea, lungs) • Circulatory System (heart, blood, vessels) • Digestive System (mouth, esophogus, stomach, intestines) • Muscular System (muscles) • Nervous System (brain, spinal cord, nerves) • Excretory System (lungs, large intestine, kidneys) • Urinary System (bladder, kidneys) • Endocrine System (glands) • Reproductive System (male and female reproductive organs) • Immune System (many types of protein, cells, organs, tissues) 2 The Skeletal System has three major jobs: • It protects our vital organs such as the brain, the heart, and the lungs. • It gives us the shape that we have. • It allows us to move. Because muscles are attached to bones, when muscles move, they move the bones and the body moves. http://kidshealth.org/kid/htbw/bones.html The Respiratory System is the system of the body that deals with breathing. When we breathe, the body takes in the oxygen that it needs and removes the carbon dioxide that it doesn't need. The organ most closely connected with this system is the lung. The human body has two lungs. http://kidshealth.org/kid/htbw/lungs.html 3 The Circulatory System is the system by which oxygen and nutrients reach the body's cells, and waste materials are carried away. -

The Muscular System
THE MUSCULAR SYSTEM COMPILED BY HOWIE BAUM 1 Muscles make up the bulk of the body and account for 1/3 of its weight.!! Blood vessels and nerves run to every muscle, helping control and regulate each muscle’s function. The muscular system creates body heat and also moves the: Bones of the Skeletal system Food through Digestive system Blood through the Circulatory system Fluids through the Excretory system MUSCLE TISSUE The body has 3 main types of muscle tissue 1) Skeletal, 2) Smooth, and 3) Cardiac SKELETAL MUSCLE SMOOTH MUSCLE CARDIAC MUSCLE Skeletal muscles attach to and move bones by contracting and relaxing in response to voluntary messages from the nervous system. Skeletal muscle tissue is composed of long cells called muscle fibers that have a striated appearance. Muscle fibers are organized into bundles supplied by blood vessels and innervated by motor neurons. Muscle structure Skeletal (striated or voluntary) muscle consists of densely packed groups of hugely elongated cells known as myofibers. These are grouped into bundles (fascicles). A typical myofiber is 2–3 centimeters ( 3/4–1 1/5 in) long and 0.05millimeters (1/500 inch) in diameter and is composed of narrower structures – myofibrils. These contain thick and thin myofilaments made up mainly of the proteins actin and myosin. Numerous capillaries keep the muscle supplied with the oxygen and glucose needed to fuel contraction. Skeletal Muscles • Skeletal muscles attach to bones by tendons (connective tissue) and enable movement. • Skeletal muscles are mostly voluntary Feel the back of your ankle to feel your Achilles tendon - the largest tendon in your body. -

Excretory Products and Their Elimination
290 BIOLOGY CHAPTER 19 EXCRETORY PRODUCTS AND THEIR ELIMINATION 19.1 Human Animals accumulate ammonia, urea, uric acid, carbon dioxide, water Excretory and ions like Na+, K+, Cl–, phosphate, sulphate, etc., either by metabolic System activities or by other means like excess ingestion. These substances have to be removed totally or partially. In this chapter, you will learn the 19.2 Urine Formation mechanisms of elimination of these substances with special emphasis on 19.3 Function of the common nitrogenous wastes. Ammonia, urea and uric acid are the major Tubules forms of nitrogenous wastes excreted by the animals. Ammonia is the most toxic form and requires large amount of water for its elimination, 19.4 Mechanism of whereas uric acid, being the least toxic, can be removed with a minimum Concentration of loss of water. the Filtrate The process of excreting ammonia is Ammonotelism. Many bony fishes, 19.5 Regulation of aquatic amphibians and aquatic insects are ammonotelic in nature. Kidney Function Ammonia, as it is readily soluble, is generally excreted by diffusion across 19.6 Micturition body surfaces or through gill surfaces (in fish) as ammonium ions. Kidneys do not play any significant role in its removal. Terrestrial adaptation 19.7 Role of other necessitated the production of lesser toxic nitrogenous wastes like urea Organs in and uric acid for conservation of water. Mammals, many terrestrial Excretion amphibians and marine fishes mainly excrete urea and are called ureotelic 19.8 Disorders of the animals. Ammonia produced by metabolism is converted into urea in the Excretory liver of these animals and released into the blood which is filtered and System excreted out by the kidneys. -

Nitric Oxide Synthase in Macula Densa Regulates Glomerular Capillary
Proc. Nati. Acad. Sci. USA Vol. 89, pp. 11993-11997, December 1992 Pharmacology Nitric oxide synthase in macula densa regulates glomerular capillary pressure (kidney/tubuloglomerular feedback response/glomerular ifitration rate/afferent arteriole) CHRISTOPHER S. WILCOX*t, WILLIAM J. WELCH*, FERID MURADf, STEVEN S. GROSS§, GRAHAM TAYLOR¶, ROBERTO LEVI§, AND HARALD H. H. W. SCHMIDTII** *Division of Nephrology, Hypertension and Transplantation Departments of Medicine, Pharmacology and Therapeutics, University of Florida College of Medicine and Department of Veterans Affairs Medical Center, Gainesville, FL 32608; I'Department of Pharmacology, Northwestern University School of Medicine, Chicago, IL; tAbbott Laboratories, Abbott Park, IL 60064-3500; iDepartment of Pharmacology, Cornell University Medical College, New York, NY 10021; and IDepartment of Clinical Pharmacology, The Royal Postgraduate Medical School, Hammersmith Hospital, London, England W12 OHS Communicated by Robert F. Furchgott, September 3, 1992 ABSTRACT Tubular-fluid reabsorption by specialized Previous studies have established that L-arginine-derived cells of the nephron at the junction of the ascending limb of the nitric oxide (NO) is produced by several cells within the loop of Henle and the distal convoluted tubule, termed the kidney, including isolated glomerular mesangial (6) and en- macula densa, releases compounds causing vasoconstriction of dothelial cells (7), and a renal epithelial cell line (8), but its the adjacent afferent arteriole. Activation of this tubuloglo- integrative role in the control ofrenal function is not yet clear merular feedback response reduces glomerular capillary pres- (9). In the vessel wall, the endothelium can mediate vasodi- sure of the nephron and, hence, the glomerular filtration rate. lator responses to agents such as acetylcholine (10) and can The tubuloglomerular feedback response functions in a nega- blunt the actions of certain vasoconstrictors (11). -

Basic Histology (23 Questions): Oral Histology (16 Questions
Board Question Breakdown (Anatomic Sciences section) The Anatomic Sciences portion of part I of the Dental Board exams consists of 100 test items. They are broken up into the following distribution: Gross Anatomy (50 questions): Head - 28 questions broken down in this fashion: - Oral cavity - 6 questions - Extraoral structures - 12 questions - Osteology - 6 questions - TMJ and muscles of mastication - 4 questions Neck - 5 questions Upper Limb - 3 questions Thoracic cavity - 5 questions Abdominopelvic cavity - 2 questions Neuroanatomy (CNS, ANS +) - 7 questions Basic Histology (23 questions): Ultrastructure (cell organelles) - 4 questions Basic tissues - 4 questions Bone, cartilage & joints - 3 questions Lymphatic & circulatory systems - 3 questions Endocrine system - 2 questions Respiratory system - 1 question Gastrointestinal system - 3 questions Genitouirinary systems - (reproductive & urinary) 2 questions Integument - 1 question Oral Histology (16 questions): Tooth & supporting structures - 9 questions Soft oral tissues (including dentin) - 5 questions Temporomandibular joint - 2 questions Developmental Biology (11 questions): Osteogenesis (bone formation) - 2 questions Tooth development, eruption & movement - 4 questions General embryology - 2 questions 2 National Board Part 1: Review questions for histology/oral histology (Answers follow at the end) 1. Normally most of the circulating white blood cells are a. basophilic leukocytes b. monocytes c. lymphocytes d. eosinophilic leukocytes e. neutrophilic leukocytes 2. Blood platelets are products of a. osteoclasts b. basophils c. red blood cells d. plasma cells e. megakaryocytes 3. Bacteria are frequently ingested by a. neutrophilic leukocytes b. basophilic leukocytes c. mast cells d. small lymphocytes e. fibrocytes 4. It is believed that worn out red cells are normally destroyed in the spleen by a. neutrophils b. -
The Urinary Tract and How It Works
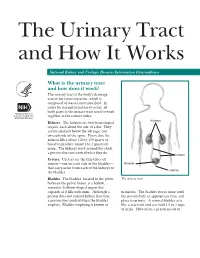
The Urinary Tract and How It Works National Kidney and Urologic Diseases Information Clearinghouse What is the urinary tract and how does it work? The urinary tract is the body’s drainage system for removing urine, which is composed of wastes and extra fluid. In order for normal urination to occur, all body parts in the urinary tract need to work together in the correct order. Kidneys Kidneys. The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the spine. Every day, the kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine. The kidneys work around the clock; a person does not control what they do. Ureters Ureters. Ureters are the thin tubes of muscle—one on each side of the bladder— Bladder that carry urine from each of the kidneys to Urethra the bladder. Bladder. The bladder, located in the pelvis The urinary tract between the pelvic bones, is a hollow, muscular, balloon-shaped organ that expands as it fills with urine. Although a urination. The bladder stores urine until person does not control kidney function, the person finds an appropriate time and a person does control when the bladder place to urinate. A normal bladder acts empties. Bladder emptying is known as like a reservoir and can hold 1.5 to 2 cups of urine. How often a person needs to urinate depends on how quickly the kidneys Why is the urinary tract produce the urine that fills the bladder. -

Claudins in the Renal Collecting Duct
International Journal of Molecular Sciences Review Claudins in the Renal Collecting Duct Janna Leiz 1,2 and Kai M. Schmidt-Ott 1,2,3,* 1 Department of Nephrology and Intensive Care Medicine, Charité-Universitätsmedizin Berlin, 12203 Berlin, Germany; [email protected] 2 Molecular and Translational Kidney Research, Max-Delbrück-Center for Molecular Medicine in the Helmholtz Association (MDC), 13125 Berlin, Germany 3 Berlin Institute of Health (BIH), 10178 Berlin, Germany * Correspondence: [email protected]; Tel.: +49-(0)30-450614671 Received: 22 October 2019; Accepted: 20 December 2019; Published: 28 December 2019 Abstract: The renal collecting duct fine-tunes urinary composition, and thereby, coordinates key physiological processes, such as volume/blood pressure regulation, electrolyte-free water reabsorption, and acid-base homeostasis. The collecting duct epithelium is comprised of a tight epithelial barrier resulting in a strict separation of intraluminal urine and the interstitium. Tight junctions are key players in enforcing this barrier and in regulating paracellular transport of solutes across the epithelium. The features of tight junctions across different epithelia are strongly determined by their molecular composition. Claudins are particularly important structural components of tight junctions because they confer barrier and transport properties. In the collecting duct, a specific set of claudins (Cldn-3, Cldn-4, Cldn-7, Cldn-8) is expressed, and each of these claudins has been implicated in mediating aspects of the specific properties of its tight junction. The functional disruption of individual claudins or of the overall barrier function results in defects of blood pressure and water homeostasis. In this concise review, we provide an overview of the current knowledge on the role of the collecting duct epithelial barrier and of claudins in collecting duct function and pathophysiology.