Perspective Rxpipeline
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WELLBUTRIN SR Safely and Effectively
HIGHLIGHTS OF PRESCRIBING INFORMATION psychosis, hallucinations, paranoia, delusions, homicidal ideation, These highlights do not include all the information needed to use aggression, hostility, agitation, anxiety, and panic, as well as suicidal WELLBUTRIN SR safely and effectively. See full prescribing ideation, suicide attempt, and completed suicide. Observe patients information for WELLBUTRIN SR. attempting to quit smoking with bupropion for the occurrence of such symptoms and instruct them to discontinue bupropion and contact a WELLBUTRIN SR (bupropion hydrochloride) sustained-release tablets, healthcare provider if they experience such adverse events. (5.2) for oral use • Initial U.S. Approval: 1985 Seizure risk: The risk is dose-related. Can minimize risk by gradually increasing the dose and limiting daily dose to 400 mg. Discontinue if WARNING: SUICIDAL THOUGHTS AND BEHAVIORS seizure occurs. (4, 5.3, 7.3) See full prescribing information for complete boxed warning. • Hypertension: WELLBUTRIN SR can increase blood pressure. Monitor blood pressure before initiating treatment and periodically during • Increased risk of suicidal thinking and behavior in children, treatment. (5.4) adolescents and young adults taking antidepressants. (5.1) • Activation of mania/hypomania: Screen patients for bipolar disorder and • Monitor for worsening and emergence of suicidal thoughts and monitor for these symptoms. (5.5) behaviors. (5.1) • Psychosis and other neuropsychiatric reactions: Instruct patients to contact a healthcare professional if such reactions occur. (5.6) --------------------------- INDICATIONS AND USAGE ---------------------------- • Angle-closure glaucoma: Angle-closure glaucoma has occurred in WELLBUTRIN SR is an aminoketone antidepressant, indicated for the patients with untreated anatomically narrow angles treated with treatment of major depressive disorder (MDD). (1) antidepressants. -

Concomitant Drugs Associated with Increased Mortality for MDMA Users Reported in a Drug Safety Surveillance Database Isaac V
www.nature.com/scientificreports OPEN Concomitant drugs associated with increased mortality for MDMA users reported in a drug safety surveillance database Isaac V. Cohen1, Tigran Makunts2,3, Ruben Abagyan2* & Kelan Thomas4 3,4-Methylenedioxymethamphetamine (MDMA) is currently being evaluated by the Food and Drug Administration (FDA) for the treatment of post-traumatic stress disorder (PTSD). If MDMA is FDA-approved it will be important to understand what medications may pose a risk of drug– drug interactions. The goal of this study was to evaluate the risks due to MDMA ingestion alone or in combination with other common medications and drugs of abuse using the FDA drug safety surveillance data. To date, nearly one thousand reports of MDMA use have been reported to the FDA. The majority of these reports include covariates such as co-ingested substances and demographic parameters. Univariate and multivariate logistic regression was employed to uncover the contributing factors to the reported risk of death among MDMA users. Several drug classes (MDMA metabolites or analogs, anesthetics, muscle relaxants, amphetamines and stimulants, benzodiazepines, ethanol, opioids), four antidepressants (bupropion, sertraline, venlafaxine and citalopram) and olanzapine demonstrated increased odds ratios for the reported risk of death. Future drug–drug interaction clinical trials should evaluate if any of the other drug–drug interactions described in our results actually pose a risk of morbidity or mortality in controlled medical settings. 3,4-Methylenedioxymethamphetamine (MDMA) is currently being evaluated by the Food and Drug Adminis- tration (FDA) for the treatment of posttraumatic stress disorder (PTSD). During the past two decades, “ecstasy” was illegally distributed and is purported to contain MDMA, but because the market is unregulated this “ecstasy” may actually contain adulterants or no MDMA at all1. -

Joel L. Young, M.D
Joel L. Young, M.D. 441 South Livernois Road, Suite 100 Rochester Hills, Michigan 48307 Phone: 248-608-8800 / Fax: 248-608-2490 / E-mail: [email protected] Professional History 2000 – Present: Chief Medical Officer and Founder, Clinical Trials Group at the Rochester Center for Behavioral Medicine, Rochester Hills, MI 1993 – Present: Medical Director and Founder, Rochester Center for Behavioral Medicine, Rochester Hills, MI (www.rcbm.net). 2008 (Current): Clinical Associate Professor of Psychiatry, Wayne State University, Detroit, MI. 2000 – 2007: Medical Director, Crittenton Network for Behavioral Health, Rochester, MI. 2000 – 2002: Chief of Staff, Department of Psychiatry, Crittenton Hospital, Rochester, MI. July, 1993 – 1997: Medical Director, Psychiatric Emergency Services, Crittenton Hospital. July, 1992 – June, 1993: Chief Resident of Adult Services, Department of Psychiatry, University of Michigan Hospitals, Ann Arbor, MI. Oct. 1991-Sept. 1993: Unit Psychiatrist, Bon Secours Adolescent Mental Health Unit, Grosse Pointe, MI. August, 1991 – 1996: Consulting Psychiatrist, Beacon Hill Clinic, Birmingham, MI. July, 1991 – June, 1992: Consulting Psychiatrist, Washtenaw County Community Mental Health Services, Ann Arbor, MI. July, 1990 – June, 1992: House Officer, Department of Psychiatry, University of Michigan Hospitals. June, 1989 – June, 1990: Intern, Departments of Internal Medicine, Pediatrics and Psychiatry, University of Michigan Hospitals. Boards 2018 Fellow: American Board of Psychiatry and Neurology 2017 Re-certification of Geriatric Qualifications by the American Board of Psychiatry and Neurology through 2027. 2017 Re-certification of Forensic Qualifications by the American Board of Psychiatry and Neurology through 2027 2014 Re-Certification by the American Board of Psychiatry and Neurology 2007 Re-certification by the American Board of Adolescent Psychiatry. -

Supported by an Educational Grant from Sunovion Pharmaceuticals Inc. Faculty
Supported by an educational grant from Sunovion Pharmaceuticals Inc. Faculty Leslie Citrome, MD, MPH C. Brendan Montano, MD Clinical Professor of Psychiatry and CT Clinical Research Behavioral Sciences Director, Principal Investigator New York Medical College Private Practice, Internal Medicine Valhalla, New York Cromwell, Connecticut Faculty Disclosure • Dr. Citrome: Consultant—Acadia, Alkermes, Allergan, Intra-Cellular Therapeutics, Janssen, Lundbeck, Merck, Neurocrine, Noven, Osmotica, Otsuka, Pfizer, Shire, Sunovion, Takeda, Teva, Vanda; Royalties—Springer Healthcare (book), UpToDate (reviewer), Wiley (Editor in Chief, International Journal of Clinical Practice); Shareholder (and spouse)—Bristol-Myers Squibb, Eli Lilly, J & J, Merck, Pfizer; Speaker—Acadia, Alkermes, Allergan, Janssen, Lundbeck, Merck, Neurocrine, Otsuka, Pfizer, Shire, Sunovion, Takeda, Teva. • Dr. Montano: Consultant—Allergan, Shire/Takeda Pharmaceutical Company Ltd., Sunovion Pharmaceuticals Inc., Arbor Pharmaceuticals Ltd.; Research Support—Allergan, Avanir, Sunovion Pharmaceuticals Inc., Tonix, BioHaven, Axsome Therapeutics, Arbor Pharmaceuticals Ltd.; Speakers Bureau— Allergan, Shire/Takeda Pharmaceutical Company Ltd., Arbor Pharmaceutical Ltd. Disclosure • The faculty have been informed of their responsibility to disclose to the audience if they will be discussing off-label or investigational use(s) of drugs, products, and/or devices (any use not approved by the US Food and Drug Administration). – The off-label and investigational use of antidepressants, topiramate, -

Horizon Scanning Status Report June 2019
Statement of Funding and Purpose This report incorporates data collected during implementation of the Patient-Centered Outcomes Research Institute (PCORI) Health Care Horizon Scanning System, operated by ECRI Institute under contract to PCORI, Washington, DC (Contract No. MSA-HORIZSCAN-ECRI-ENG- 2018.7.12). The findings and conclusions in this document are those of the authors, who are responsible for its content. No statement in this report should be construed as an official position of PCORI. An intervention that potentially meets inclusion criteria might not appear in this report simply because the horizon scanning system has not yet detected it or it does not yet meet inclusion criteria outlined in the PCORI Health Care Horizon Scanning System: Horizon Scanning Protocol and Operations Manual. Inclusion or absence of interventions in the horizon scanning reports will change over time as new information is collected; therefore, inclusion or absence should not be construed as either an endorsement or rejection of specific interventions. A representative from PCORI served as a contracting officer’s technical representative and provided input during the implementation of the horizon scanning system. PCORI does not directly participate in horizon scanning or assessing leads or topics and did not provide opinions regarding potential impact of interventions. Financial Disclosure Statement None of the individuals compiling this information have any affiliations or financial involvement that conflicts with the material presented in this report. Public Domain Notice This document is in the public domain and may be used and reprinted without special permission. Citation of the source is appreciated. All statements, findings, and conclusions in this publication are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI) or its Board of Governors. -

Classification Decisions Taken by the Harmonized System Committee from the 47Th to 60Th Sessions (2011
CLASSIFICATION DECISIONS TAKEN BY THE HARMONIZED SYSTEM COMMITTEE FROM THE 47TH TO 60TH SESSIONS (2011 - 2018) WORLD CUSTOMS ORGANIZATION Rue du Marché 30 B-1210 Brussels Belgium November 2011 Copyright © 2011 World Customs Organization. All rights reserved. Requests and inquiries concerning translation, reproduction and adaptation rights should be addressed to [email protected]. D/2011/0448/25 The following list contains the classification decisions (other than those subject to a reservation) taken by the Harmonized System Committee ( 47th Session – March 2011) on specific products, together with their related Harmonized System code numbers and, in certain cases, the classification rationale. Advice Parties seeking to import or export merchandise covered by a decision are advised to verify the implementation of the decision by the importing or exporting country, as the case may be. HS codes Classification No Product description Classification considered rationale 1. Preparation, in the form of a powder, consisting of 92 % sugar, 6 % 2106.90 GRIs 1 and 6 black currant powder, anticaking agent, citric acid and black currant flavouring, put up for retail sale in 32-gram sachets, intended to be consumed as a beverage after mixing with hot water. 2. Vanutide cridificar (INN List 100). 3002.20 3. Certain INN products. Chapters 28, 29 (See “INN List 101” at the end of this publication.) and 30 4. Certain INN products. Chapters 13, 29 (See “INN List 102” at the end of this publication.) and 30 5. Certain INN products. Chapters 28, 29, (See “INN List 103” at the end of this publication.) 30, 35 and 39 6. Re-classification of INN products. -

MEDICATION GUIDE WELLBUTRIN® (WELL Byu-Trin) (Bupropion Hydrochloride) Tablets
NDA 018644/S-041 NDA 020358/S-048 Page 6 MEDICATION GUIDE WELLBUTRIN® (WELL byu-trin) (bupropion hydrochloride) Tablets Read this Medication Guide carefully before you start using WELLBUTRIN and each time you get a refill. There may be new information. This information does not take the place of talking with your doctor about your medical condition or your treatment. If you have any questions about WELLBUTRIN, ask your doctor or pharmacist. IMPORTANT: Be sure to read the three sections of this Medication Guide. The first section is about the risk of suicidal thoughts and actions with antidepressant medicines; the second section is about the risk of changes in thinking and behavior, depression and suicidal thoughts or actions with medicines used to quit smoking; and the third section is entitled “What Other Important Information Should I Know About WELLBUTRIN?” Antidepressant Medicines, Depression and Other Serious Mental Illnesses, and Suicidal Thoughts or Actions This section of the Medication Guide is only about the risk of suicidal thoughts and actions with antidepressant medicines. Talk to your, or your family member’s, healthcare provider about: • all risks and benefits of treatment with antidepressant medicines • all treatment choices for depression or other serious mental illness What is the most important information I should know about antidepressant medicines, depression and other serious mental illnesses, and suicidal thoughts or actions? 1. Antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, and young adults within the first few months of treatment. 2. Depression and other serious mental illnesses are the most important causes of suicidal thoughts and actions. -
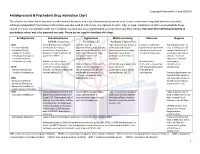
Antidepressant & Psychedelic Drug Interaction Chart
Copyright Psychedelic School 8/2020 Antidepressant & Psychedelic Drug Interaction Chart This chart is not intended to be used to make medical decisions and is for informational purposes only. It was constructed using data whenever possible, although extrapolation from known information was also used to inform risk. Any decision to start, stop, or taper medication and/or use psychedelic drugs should be made in conjunction with your healthcare provider(s). It is recommended to not perform any illicit activity. This chart the intellectual property of psychedelic school and is for personal use only. Please do not copy or distribute this chart. Antidepressant Phenethylamines Tryptamines MAOI-containing Ketamine Ibogaine -MDMA, mescaline -Psilocybin, LSD -Ayahuasca, Syrian Rue SSRIs Taper & discontinue at least 2 Consider taper & Taper & discontinue at least 2 Has been studied and Taper & discontinue at · Paroxetine (Paxil) weeks prior (all except discontinuation at least 2 weeks weeks prior (all except found effective both with least 2 weeks prior (all · Sertraline (Zoloft) fluoxetine) or 6 weeks prior prior (all except fluoxetine) or 6 fluoxetine) or 6 weeks prior and without concurrent except fluoxetine) or 6 · Citalopram (Celexa) (fluoxetine only) due to loss of weeks prior (fluoxetine only) (fluoxetine only) due to use of antidepressants weeks prior (fluoxetine · Escitalopram (Lexapro) psychedelic effect due to potential loss of potential risk of serotonin only) due to risk of · Fluxoetine (Prozac) psychedelic effect syndrome additive QTc interval · Fluvoxamine (Luvox) MDMA is unable to cause Recommended prolongation, release of serotonin when the Chronic antidepressant use may Life threatening toxicities can to be used in conjunction arrhythmias, or SPARI serotonin reuptake pump is result in down-regulation of occur with these with oral antidepressants cardiotoxicity · Vibryyd (Vilazodone) blocked. -

Phd Thesis Project: Pharmacological and Toxicological Investigations of New Psychoactive Substances, Supervised by Prof
PHARMACOLOGICAL AND TOXICOLOGICAL INVESTIGATIONS OF NEW PSYCHOACTIVE SUBSTANCES Inauguraldissertation zur Erlangung der Würde eines Doktors der Philosophie vorgelegt der Philosophisch-Naturwissenschaftlichen Fakultät der Universität Basel von Dino Lüthi aus Rüderswil, Bern Basel, 2018 Originaldokument gespeichert auf dem Dokumentenserver der Universität Basel edoc.unibas.ch Dieses Werk ist lizenziert unter einer Creative Commons Namensnennung-Nicht kommerziell 4.0 International Lizenz (https://creativecommons.org/licenses/by-nc-sa/4.0/deed.de). Genehmigt von der Philosophisch-Naturwissenschaftlichen Fakultät auf Antrag von Prof. Stephan Krähenbühl, Prof. Matthias E. Liechti und Prof. Anne Eckert. Basel, den 26.06.2018 Prof. Martin Spiess Dekan der Philosophisch- Naturwissenschaftlichen Fakultät PHARMACOLOGICAL AND TOXICOLOGICAL INVESTIGATIONS OF NEW PSYCHOACTIVE SUBSTANCES “An adult must make his own decision as to whether or not he should expose himself to a specific drug, be it available by prescription or proscribed by law, by measuring the potential good and bad with his own personal yardstick.” ― Alexander Shulgin, Pihkal: A Chemical Love Story. PREFACE This thesis is split into a pharmacology part and a toxicology part. The pharmacology part consists of investigations on the monoamine transporter and receptor interactions of traditional and newly emerged drugs, mainly stimulants and psychedelics; the toxicology part consists of investigations on mechanisms of hepatocellular toxicity of synthetic cathinones. All research described in this thesis has been published in peer-reviewed journals, and was performed between October 2014 and June 2018 in the Division of Clinical Pharmacology and Toxicology at the Department of Biomedicine of the University Hospital Basel and University of Basel, and partly at the pRED Roche Innovation Center Basel at F. -

MEDICATION GUIDE Bupropion Hydrochloride Extended-Release
MEDICATION GUIDE BuPROPion Hydrochloride Extended-Release Tablets, USP (SR) (byoo-PROE-pee-on) Read this Medication Guide carefully before you start taking bupropion hydrochloride extended-release tablets (SR) and each time you get a refill. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or your treatment. If you have any questions about bupropion hydrochloride extended-release tablets (SR), ask your healthcare provider or pharmacist. IMPORTANT: Be sure to read the three sections of this Medication Guide. The first section is about the risk of suicidal thoughts and actions with antidepressant medicines; the second section is about the risk of changes in thinking and behavior, depression and suicidal thoughts or actions with medicines used to quit smoking; and the third section is entitled “What Other Important Information Should I Know About Bupropion Hydrochloride Extended-Release Tablets (SR)?” Antidepressant Medicines, Depression and Other Serious Mental Illnesses, and Suicidal Thoughts or Actions This section of the Medication Guide is only about the risk of suicidal thoughts and actions with antidepressant medicines. Talk to your healthcare provider or your family member’s healthcare provider about: • all risks and benefits of treatment with antidepressant medicines • all treatment choices for depression or other serious mental illness What is the most important information I should know about antidepressant medicines, depression and other serious mental illnesses, and suicidal thoughts or actions? 1. Antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, or young adults within the first few months of treatment. -

Treatment-Resistant Attention-Deficit Hyperactivity Disorder: Clinical
Review Treatment-resistant Attention-deficit Hyperactivity Disorder: Clinical Significance, Concept, and Management Mu‑Hong Chen, M.D., Ph.D.1,2, Kai‑Lin Huang, M.D.1,2, Ju‑Wei Hsu, M.D.1,2,*, Shih‑Jen Tsai, M.D.1,2,* 1Department of Psychiatry, Taipei Veterans General Hospital, 2Division of Psychiatry, School of Medicine, National Yang‑Ming University, Taipei, Taiwan Abstract Background: Attention-deficit hyperactivity disorder (ADHD) is the most commonly diagnosed neurodevelopmental disorder known to cause impairment across the lifespan. ADHD was ranked as approximately the 50th leading cause of global years lived with disability for children, coming in ahead of diabetes, meningitis, and intellectual disability. About 20%–40% of patients with ADHD would not achieve the treatment response and symptomatic remission, increasing future risks of substance abuse, suicidal behavior, and premature mortality. However, there is no standard consensus for defining treatment resistance in ADHD.Method: In this systematic review, we intend to focus on treatment-resistant ADHD in the aspects of disease definition, psychopathology, pathophysiology, and treatment. Results: We suggest that the more ideal strategy of defining treatment resistance should consider the improvement of ADHD symptoms and the global functioning simultaneously. Psychiatric comorbidities (i.e. destructive behavior disorders and mood disorders), physical comorbidities (i.e. epilepsy), and psychosocial adversities (i.e. parental psychopathology and poor family functioning) should be the first to be assessed in the evaluation of treatment response or resistance. The optimal medication adjustment or the combination of medications and psychotherapy may be the potential therapeutic strategy for treatment-resistant ADHD. Conclusion: Further studies would be necessary to elucidate the underlying mechanisms of treatment-resistant ADHD and to research the novel treatment strategies for ADHD. -

Rxoutlook® 1St Quarter 2019
® RxOutlook 1st Quarter 2020 optum.com/optumrx a RxOutlook 1st Quarter 2020 Orphan drugs continue to feature prominently in the drug development pipeline In 1983 the Orphan Drug Act was signed into law. Thirty seven years later, what was initially envisioned as a minor category of drugs has become a major part of the drug development pipeline. The Orphan Drug Act was passed by the United States Congress in 1983 in order to spur drug development for rare conditions with high unmet need. The legislation provided financial incentives to manufacturers if they could demonstrate that the target population for their drug consisted of fewer than 200,000 persons in the United States, or that there was no reasonable expectation that commercial sales would be sufficient to recoup the developmental costs associated with the drug. These “Orphan Drug” approvals have become increasingly common over the last two decades. In 2000, two of the 27 (7%) new drugs approved by the FDA had Orphan Designation, whereas in 2019, 20 of the 48 new drugs (42%) approved by the FDA had Orphan Designation. Since the passage of the Orphan Drug Act, 37 years ago, additional regulations and FDA designations have been implemented in an attempt to further expedite drug development for certain serious and life threatening conditions. Drugs with a Fast Track designation can use Phase 2 clinical trials to support FDA approval. Drugs with Breakthrough Therapy designation can use alternative clinical trial designs instead of the traditional randomized, double-blind, placebo-controlled trial. Additionally, drugs may be approved via the Accelerated Approval pathway using surrogate endpoints in clinical trials rather than clinical outcomes.