Aboriginal and Torres Strait Islander Health Care Choices and Access Barriers in Mount Isa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Legislative Assembly Hansard 1982
Queensland Parliamentary Debates [Hansard] Legislative Assembly THURSDAY, 1 APRIL 1982 Electronic reproduction of original hardcopy Workers' Compensation Act Amendment Bill 31 March & 1 April 1982 5465 THURSDAY, 1 APRIL 1982 Mr SPEAKER (Hon. S. J. MuUer, Fassifern) read prayers and took the chair at 11 a.m. PAPERS The following paper was laid on the table, and ordered to be printed:— Report of the Commissioner of Water Resources for the year ended 30 June 1981 5466 1 AprU 1982 Ministerial Statements The following papers were laid on the table:— Orders in Council under— Grammar Schools Act 1975 and the Local Bodies' Loans Guarantee Act 1923-1979 Jury Act 1929-1981 Magistrates Courts Act 1921-1976 Supreme Court Act 1921-1979 Rule under the Coroners Act 1958-1980 MINISTERIAL STATEMENTS Parliamentary White Paper on FamUy Welfare Hon. T. A. WHITE (Redcliffe—Minister for Welfare Services) (11.2 a.m.): I rise today to inform aU members on the progress of the pariiamentary Whke Paper on the proposed family welfare legislation, which I tabled in Parliament on 3 December last year. Members will be aware that, when I tabled the paper, I stressed that its purpose was to promote discussion and concensus in the community about the proposals for the new legislation. I also stated that the paper would be "widely disseminated throughout the community so that individuals and interested organisations may comment upon it". This has been done. Over 5 500 copies of the White Paper have been distributed throughout Queensland. Also, there has been ample media coverage of the paper to further inform the public of what is proposed. -

John Newfong (3/11/1943-30/5/1999), Aboriginal Activist, Commentator, and Public Servant Left an Indelible Mark on Aboriginal Affairs
John Newfong (3/11/1943-30/5/1999), Aboriginal activist, commentator, and public servant left an indelible mark on Aboriginal Affairs. As a descendant of Ngugi people of the Moreton Bay region in Queensland, he drew much on the history of his people and how they maintained a continuous connection with land and sea despite European settlement. It was from this cultural background that John drew during the course of his life and it sustained him whilst working in Canberra and Sydney and overseas. As a print media journalist, he completed a cadetship in the mid-1960s and subsequently worked for The Australian, The Sydney Morning-Herald and The Bulletin in the early 1970s. However, he experienced the tension caused by the often conflicting professional and political demands on him. At the time, the Editor of The Australian , Adrian Deamer warned him that if he did not acquire and develop all of his professional skills, he would do "…nothing else but write about being black". According to David Armstrong, The Australian’s Chief of Staff, John's political activism was the main reason for him leaving the media as "…he eventually felt he was able to do more for the cause". Upon leaving the media, John began to immerse himself more and more in the affairs of FCAATSI and the National Tribal Council. Whilst his full-time career in journalism ended in early 1972, he continued to periodically write as a columnist or commentator for The Australian , The Canberra Times , The Courier-Mail , The Review, The National Interest, The Sydney Morning-Herald , and, The Australian Financial Review until his death. -

Professor Susan Forde Director Griffith Centre for Social and Cultural Research Griffith University
Professor Susan Forde Director Griffith Centre for Social and Cultural Research Griffith University Contact Work: (07) 3735 7229 Email: [email protected] Qualifications Doctor of Philosophy, University of Queensland, 1998 Bachelor of Arts (Hons, Class I) University of Queensland, 1992 Professional Memberships and Positions Visiting Scholar, The Membership Puzzle Project Arthur L. Carter Journalism Institute, New York University January 2018 Advisory Board Griffith Review November 2017-present Vice President (Research) Journalism Education and Research Association of Australia (JERAA) December 2017-present Advisory Board Community Communication and Alternative Media section International Association for Media and Communication Research July 2017-present Founding Editor (with Professor Chris Atton) Journal of Alternative and Community Media (joacm.org) Jointly published by the IAMCR’s Community Communication and Alternative Media section and the Griffith ePress Launched Montreal, Canada July 2015 Vice-Chair (elected position) Community Communication Section International Association of Media and Communication Research July 2012-June 2016 Editorial Advisory Board 3CMedia: Journal of Third Sector Media Scholarly e-journal, published by the Community Broadcasting Association of Australia Editor, 2006-2013 Australian Journalism Monographs Jointly published by the Journalism Education Association of Australia (now JERAA); and Griffith University Journalism Education & Research Association of Australia, Member Australian & New Zealand Communications -

Full Thesis Draft No Pics
A whole new world: Global revolution and Australian social movements in the long Sixties Jon Piccini BA Honours (1st Class) A thesis submitted for the degree of Doctor of Philosophy at The University of Queensland in 2013 School of History, Philosophy, Religion & Classics Abstract This thesis explores Australian social movements during the long Sixties through a transnational prism, identifying how the flow of people and ideas across borders was central to the growth and development of diverse campaigns for political change. By making use of a variety of sources—from archives and government reports to newspapers, interviews and memoirs—it identifies a broadening of the radical imagination within movements seeking rights for Indigenous Australians, the lifting of censorship, women’s liberation, the ending of the war in Vietnam and many others. It locates early global influences, such as the Chinese Revolution and increasing consciousness of anti-racist struggles in South Africa and the American South, and the ways in which ideas from these and other overseas sources became central to the practice of Australian social movements. This was a process aided by activists’ travel. Accordingly, this study analyses the diverse motives and experiences of Australian activists who visited revolutionary hotspots from China and Vietnam to Czechoslovakia, Algeria, France and the United States: to protest, to experience or to bring back lessons. While these overseas exploits, breathlessly recounted in articles, interviews and books, were transformative for some, they also exposed the limits of what a transnational politics could achieve in a local setting. Australia also became a destination for the period’s radical activists, provoking equally divisive responses. -

A Reflection on the First 30 Days of the 1972 Aboriginal Embassy
A REFLECTION ON THE FIRST THIRTY DAYS OF THE EMBASSY By Gary Foley From the book: Foley, G, Schaap, A & Howell, E 2013, The Aboriginal Tent Embassy. [electronic resource] : Sovereignty, Black Power, Land Rights and the State, Hoboken : Taylor and Francis, 2013 It was in the first four weeks of the 1972 Aboriginal Embassy protest that a small group of Aboriginal activists rapidly improvised and transformed an opportunistic accident into an effective protest that captured world attention and brought significant historical and political change in Australia.1 What had begun as a simple knee-jerk reaction to an Australia Day statement on Land Rights by the Australian Prime Minister, resulted in the accidental discovery that there was no law in Canberra that prevented the activists from staging a protest camp on the lawns of Parliament. The swift action of the activists to take advantage of this situation enabled them to gain political advantage over the McMahon Government in the propaganda war and political battle that would take place over the next six months. Exactly how these events unfolded has never been written about in detail. Even in Scott Robinson’s (ch.1 in this volume) or in Kathy Lothian’s (2007) accounts, the crucial early days are not fully examined. Yet if we are to gain a better understanding of why the Aboriginal Embassy was able to become such an effective protest action, it is important to gain an awareness of how it all began. So in this chapter I will examine some of the factors that enabled the already highly effective group of Aboriginal activists from the Redfern Black Power collective to create a highly effective challenge to the political power structure and force a major change in policy. -

82 3.3.4.4.3 Ecogeographic Studies of the Cranial Shape The
82 3.3.4.4.3 Ecogeographic studies of the cranial shape The measurement of the human head of both the living and dead has long been a matter of interest to a variety of professions from artists to physicians and latterly to anthropologists (for a review see Spencer 1997c). The shape of the cranium, in particular, became an important factor in schemes of racial typology from the late 18th Century (Blumenbach 1795; Deniker 1898; Dixon 1923; Haddon 1925; Huxley 1870). Following the formulation of the cranial index by Retzius in 1843 (see also Sjovold 1997), the classification of humans by skull shape became a positive fashion. Of course such classifications were predicated on the assumption that cranial shape was an immutable racial trait. However, it had long been known that cranial shape could be altered quite substantially during growth, whether due to congenital defect or morbidity or through cultural practices such as cradling and artificial cranial deformation (for reviews see (Dingwall 1931; Lindsell 1995). Thus the use of cranial index of racial identity was suspect. Another nail in the coffin of the Cranial Index's use as a classificatory trait was presented in Coon (1955), where he suggested that head form was subject to long term climatic selection. In particular he thought that rounder, or more brachycephalic, heads were an adaptation to cold. Although it was plausible that the head, being a major source of heat loss in humans (Porter 1993), could be subject to climatic selection, the situation became somewhat clouded when Beilicki and Welon demonstrated in 1964 that the trend towards brachycepahlisation was continuous between the 12th and 20th centuries in East- Central Europe and thus could not have been due to climatic selection (Bielicki & Welon 1964). -

Managing Indigenous Pastoral Lands
module three land information MANAGING INDIGENOUS PASTORAL LANDS Pub no. 14/019 McClelland Rural Services Pty Ltd MODULE 3 land information Contents Introduction 3 List of Tables Indigenous Land Rights and Pastoral Figure 3.1 Map of Northern Territory Land Holdings 5 Aboriginal Land 7 Land Rights 5 Figure 3.2 Map of Queensland Indigenous Pastoral Land Holdings 5 Aboriginal Land 8 Land Tenure 10 Figure 3.3 Map of Western Australian Indigenous Lands - Aboriginal Land (Kimberley & Pilbara) 9 Definitions and Complexities 10 Indigenous Land Holding Arrangements List of Photos in the Northern Territory 11 Cover Photo – Ghost gums Legal Framework 11 Permitted Land Uses 11 Indigenous Land Holding Arrangements in Queensland 12 Legal Framework 12 Forms of Land Acquisition 12 Renewals of Pastoral Leases 13 Indigenous Land Holding Arrangements in Western Australia 14 Legal Framework 14 Forms of Land Acquisition 14 Pastoral Lease Reform 15 Renewals of Pastoral Leases 15 Role of Land Councils 18 Overview 18 Northern Territory 18 Queensland 18 Western Australia 19 Land Use Agreements 20 Mining Tenures and Income from Mining on Indigenous Land 22 Mining Tenures 22 Mining Income 24 2 MODULE 3 land information Introduction Module 3 describes the rights and obligations of Indigenous land holders in the northern Australia pastoral industry. Indigenous land tenure is administered differently in the Northern Territory (NT), Queensland (Qld) and Western Australia (WA) which has resulted in a high degree of complexity. In addition, this whole area is undergoing a great deal of change. • In November 2012, the Northern Australia Ministerial Forum (NAMF) initiated a review of land tenure management across northern Australia. -

Critical Australian Indigenous Histories
Transgressions critical Australian Indigenous histories Transgressions critical Australian Indigenous histories Ingereth Macfarlane and Mark Hannah (editors) Published by ANU E Press and Aboriginal History Incorporated Aboriginal History Monograph 16 National Library of Australia Cataloguing-in-Publication entry Title: Transgressions [electronic resource] : critical Australian Indigenous histories / editors, Ingereth Macfarlane ; Mark Hannah. Publisher: Acton, A.C.T. : ANU E Press, 2007. ISBN: 9781921313448 (pbk.) 9781921313431 (online) Series: Aboriginal history monograph Notes: Bibliography. Subjects: Indigenous peoples–Australia–History. Aboriginal Australians, Treatment of–History. Colonies in literature. Australia–Colonization–History. Australia–Historiography. Other Authors: Macfarlane, Ingereth. Hannah, Mark. Dewey Number: 994 Aboriginal History is administered by an Editorial Board which is responsible for all unsigned material. Views and opinions expressed by the author are not necessarily shared by Board members. The Committee of Management and the Editorial Board Peter Read (Chair), Rob Paton (Treasurer/Public Officer), Ingereth Macfarlane (Secretary/ Managing Editor), Richard Baker, Gordon Briscoe, Ann Curthoys, Brian Egloff, Geoff Gray, Niel Gunson, Christine Hansen, Luise Hercus, David Johnston, Steven Kinnane, Harold Koch, Isabel McBryde, Ann McGrath, Frances Peters- Little, Kaye Price, Deborah Bird Rose, Peter Radoll, Tiffany Shellam Editors Ingereth Macfarlane and Mark Hannah Copy Editors Geoff Hunt and Bernadette Hince Contacting Aboriginal History All correspondence should be addressed to Aboriginal History, Box 2837 GPO Canberra, 2601, Australia. Sales and orders for journals and monographs, and journal subscriptions: T Boekel, email: [email protected], tel or fax: +61 2 6230 7054 www.aboriginalhistory.org ANU E Press All correspondence should be addressed to: ANU E Press, The Australian National University, Canberra ACT 0200, Australia Email: [email protected], http://epress.anu.edu.au Aboriginal History Inc. -

Asymmetrical Distinctions in Waanyi Kinship Terminology1 Mary Laughren
12 Asymmetrical Distinctions in Waanyi Kinship Terminology1 Mary Laughren Introduction Background Waanyi2 kinship terms map onto an ‘Arandic’ system with distinct encoding of the four logical combinations of maternal and paternal relations in the ascending harmonic (‘grandparent’) generation: 1 Without the generous collaboration of the late Mr Roy Seccin Kamarrangi, who valiantly attempted to teach me Waanyi between 2000 and 2005, this study would not have begun. I also acknowledge the assistance received from the late Mr Eric King Balyarrinyi and his companions at the Doomadgee nursing home. I am indebted to Gavan Breen, who shared his Waanyi field notes and insights with me, and to John Dymock, who gave me copies of his vast corpus of Waanyi vocabulary. Thank you to the two anonymous reviewers, whose input to the development of this chapter was substantial, and to Barry Alpher, who provided invaluable feedback on an earlier draft. Errors of fact or interpretation remain my responsibility. The research on Waanyi was supported by a number of small ARC grants through the University of Queensland and the Waanyi Nation Aboriginal Corporation. 2 Waanyi was traditionally spoken in land watered by the upper branches of the Nicholson River and its tributaries, which straddles the Queensland–Northern Territory border to the south of the Gulf of Carpentaria (see Tindale 1974; Trigger 1982). The most closely related language is Garrwa (Breen 2003; Mushin 2012), spoken to the immediate north of Waanyi. The Garrwa-Waanyi language block lies between the northern and southern branches of the Warluwarric language group (Blake 1988, 1990) and is bordered on the east by the Tangkic language Yukulta, also called Ganggalida, (Keen 1983; Nancarrow et al. -

Pulling Down Fences an Oral History with Lyall Munro Jr
Online Only Pulling down fences An oral history with Lyall Munro Jr by Susan Forde (https://www.griffithreview.com/contributors/susan-forde/) Aboriginal and Torres Strait Islander people are advised that this article contains the names of people who have died. In 2012, researchers Susan Forde, Kerrie Foxwell, and Elizabeth Burrows embarked on a research project to collect and present the ‘voices’ of the movement for land rights and equality in Queensland. It was motivated by an urgent need to record the contribution of many activists and political voices little known to the broader Australian community who have had a significant impact on the shape of Indigenous politics and affairs over the past century. The project was scoped in consultation with the people interviewed, and aimed to engage with and listen to both the Indigenous researchers who worked on the project and the interviewees themselves to guide the project’s content and boundaries. For much of our recent history, Aboriginal voices have been interpreted and twisted to meet particular news and political agendas. Given this understanding, a key aim of this project has been to present the voices of the movement ‘unfiltered’. The following interview with long-time activist Lyall Munro Jr has been lightly edited in the interests of moulding the story and bringing reading clarity to Lyall’s memories and thoughts; but on the whole, the text presented below is raw in its insights and recollections. Lyall Munro Jr is a Kamilaroi man who was born in Moree, in northern New South Wales, in 1951. He has taken a leading and radical role in the Aboriginal land rights movement, participating in major actions such as the 1972 Aboriginal Tent Embassy, 1982 Commonwealth Games protests, 1988 bicentennial protests, anti- Bjelke-Petersen actions in Queensland, and the dismantling of the gates of the Parliament Houses in both Sydney and Brisbane following failed land rights negotiations. -

The Blackwords Symposium: the Past, Present, and Future of Aboriginal and Torres Strait Islander Literature
The BlackWords Symposium: The Past, Present, and Future of Aboriginal and Torres Strait Islander Literature KERRY KILNER University of Queensland PETER MINTER University of Sydney We write to create, to survive, and to revolutionise; we write to haunt and we ache because we refuse to leave the past alone. We aim to disrupt the State’s founding order of things, to disrupt ‘patriarchal white sovereignty’ (Moreton- Robinson), white heteronormativity, and the colonial-continuum of history. (Harkin, herein) The BlackWords Symposium, held in October 2012, celebrated the fifth anniversary of the establishment of BlackWords, the AustLit-supported project recording information about, and research into, Aboriginal and Torres Strait Islander writers and storytellers. The symposium showcased the exciting state of Aboriginal and Torres Strait Islander creative writing and storytelling across all forms, contemporary scholarship on Indigenous writing, alongside programs such as the State Library of Queensland’s black&write! project, which supports writers’ fellowships, editing mentorships, and a trainee editor program for professional development for Indigenous editors. But really, the event was a celebration of the sort of thinking, the sort of resistance, and the re-writing of history that is evident in the epigraph to this introduction. The speakers, who included Melissa Lucashenko, Wesley Enoch, Sandra Phillips, Ellen Van Neerven, Jeanine Leane, and Boori Pryor alongside the authors of the works in this collection, explored a diverse range of topics -
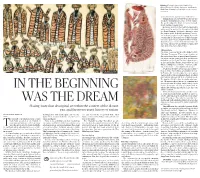
150718-TH.M-4-In the Beginning Was the Dream
Alluring (Clockwise from left) ‘Untitled’ by William Barak; 'Red Plains Kangaroo' by Yirawala; 'Bush Plum Country' by Poly Ngal. National Gallery of Australia innocence comes apart when we look closer. William Barak (1824-1903) belonged to the Wu- rundjeri/ Woiwurung peoples, of Port Phillip. His work bridges the divide between the tradi- tional and the contemporary. He moves away from the traditional geometric patterns in the work of the Aboriginals that did not depict humans, but were a means to seize the animal spirit. In Barak’s painting ‘Corrobo- ree’ we have people of cooler regions, dressed in Possum skin cloaks. Barak was a child when Eu- ropeans began to make incursions into Port Phil- lip and he represents the transition of cultures in his works. The Europeans referred to him as the ‘last chief of the Yarra Yarra Tribe.’ Three sisters The video room has works of the Bidjara artist, Christian Thompson. Three large monitors at the centre show three women of mixed ancestry. An off-screen fan blows their hair and they are bathed in a yellow light. The idea is that they are in the Queensland desert, buffeted by its arid winds. A lilting piece of music — hypnotic, calm- ing and sensuous — accompanies the images. I learn that the three are not just any women — they are three sisters whose grandfather is Char- SPOTLIGHT lie Perkins, the first Aboriginal person to gain a degree and become a permanent head of federal government. His parents were of mixed blood. His daughter, Hetti Perkins, is an influential cura- tor.