Cancer in Lahore, Pakistan, 2010–2019: an Incidence Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

S# BRANCH CODE BRANCH NAME CITY ADDRESS 1 24 Abbottabad
BRANCH S# BRANCH NAME CITY ADDRESS CODE 1 24 Abbottabad Abbottabad Mansera Road Abbottabad 2 312 Sarwar Mall Abbottabad Sarwar Mall, Mansehra Road Abbottabad 3 345 Jinnahabad Abbottabad PMA Link Road, Jinnahabad Abbottabad 4 131 Kamra Attock Cantonment Board Mini Plaza G. T. Road Kamra. 5 197 Attock City Branch Attock Ahmad Plaza Opposite Railway Park Pleader Lane Attock City 6 25 Bahawalpur Bahawalpur 1 - Noor Mahal Road Bahawalpur 7 261 Bahawalpur Cantt Bahawalpur Al-Mohafiz Shopping Complex, Pelican Road, Opposite CMH, Bahawalpur Cantt 8 251 Bhakkar Bhakkar Al-Qaim Plaza, Chisti Chowk, Jhang Road, Bhakkar 9 161 D.G Khan Dera Ghazi Khan Jampur Road Dera Ghazi Khan 10 69 D.I.Khan Dera Ismail Khan Kaif Gulbahar Building A. Q. Khan. Chowk Circular Road D. I. Khan 11 9 Faisalabad Main Faisalabad Mezan Executive Tower 4 Liaqat Road Faisalabad 12 50 Peoples Colony Faisalabad Peoples Colony Faisalabad 13 142 Satyana Road Faisalabad 585-I Block B People's Colony #1 Satayana Road Faisalabad 14 244 Susan Road Faisalabad Plot # 291, East Susan Road, Faisalabad 15 241 Ghari Habibullah Ghari Habibullah Kashmir Road, Ghari Habibullah, Tehsil Balakot, District Mansehra 16 12 G.T. Road Gujranwala Opposite General Bus Stand G.T. Road Gujranwala 17 172 Gujranwala Cantt Gujranwala Kent Plaza Quide-e-Azam Avenue Gujranwala Cantt. 18 123 Kharian Gujrat Raza Building Main G.T. Road Kharian 19 125 Haripur Haripur G. T. Road Shahrah-e-Hazara Haripur 20 344 Hassan abdal Hassan Abdal Near Lari Adda, Hassanabdal, District Attock 21 216 Hattar Hattar -

The Lahore Declaration
The Lahore Declaration The following is the text of the Lahore Declaration signed by the Prime Minister, Mr. A. B. Vajpayee, and the Pakistan Prime Minister, Mr. Nawaz Sharif, in Lahore on Sunday: The Prime Ministers of the Republic of India and the Islamic Republic of Pakistan: Sharing a vision of peace and stability between their countries, and of progress and prosperity for their peoples; Convinced that durable peace and development of harmonious relations and friendly cooperation will serve the vital interests of the peoples of the two countries, enabling them to devote their energies for a better future; Recognising that the nuclear dimension of the security environment of the two countries adds to their responsibility for avoidance of conflict between the two countries; Committed to the principles and purposes of the Charter of the United Nations, and the universally accepted principles of peaceful co- existence; Reiterating the determination of both countries to implementing the Simla Agreement in letter and spirit; Committed to the objective of universal nuclear disarmament and non- proliferartion; Convinced of the importance of mutually agreed confidence building measures for improving the security environment; Recalling their agreement of 23rd September, 1998, that an environment of peace and security is in the supreme national interest of both sides and that the resolution of all outstanding issues, including Jammu and Kashmir, is essential for this purpose; Have agreed that their respective Governments: · shall intensify their efforts to resolve all issues, including the issue of Jammu and Kashmir. · shall refrain from intervention and interference in each other's internal affairs. -

Diagnostic Centers'!A1 Laboratories!A1 Dental Centers'!A1 Ophthalmology Clinics'!A1 Medical Center'!A1 Diagnostic Centers
Diagnostic Centers'!A1 Laboratories!A1 Dental Centers'!A1 Ophthalmology Clinics'!A1 Medical Center'!A1 Diagnostic Centers L I S T O F A L L I A N Z E F U N E T W O R K D I S C O U N T D I A G N O S T I C C E N T R E S S.No Hospital Name Address Contact Contact Person Email Contact Number City Discount Category 021-35662052 Mr. Yousuf Poonawala 1 Burhani Diagnostic Centre Jaffer Plaza, Mansfield Street, Saddar, Karachi. 021-5661952 Karachi 10-15% Diagnostic Center 0336-0349355 (Administrator) [email protected] 02136626125-6 0334-3357471 [email protected] 2 Dr. Essa's Laboratory & Diagnostic Centre (Main Centre) B-122 (Blue Building) Block-H, Shahrah-e-Jahangir, Near Five Star, North Nazimabad. Mr. Shakeel / Ms. Shahida 021-36625149 Karachi 10-20% Diagnostic Center 0335-5755529 [email protected] 021-36312746 0335- 2.1 Ayesha Manzil Centre Ali Appartment, FB Area Karachi Karachi 10-20% Diagnostic Center 5755536 021-35862522 021- 2.2 Zamzama Centre Suite # 2, Plot 8-C (Beside Aijaz Boutique), 4th Zamzama Commercial Lane Karachi 10-20% Diagnostic Center 35376887 2.3 Medilink Centre Suite # 103, 1st Floor, The Plaza, 2 Talwar, Khayaban-e-Iqbal, Main Clifton Road, Karachi 021-35376071-74 Karachi 10-20% Diagnostic Center 2.4 Abdul Hassan Isphahani Centre A-1/3&4, Block-4, gulshan-e-Iqbal. Main Abdul Hassan Isphahani Road, Karachi 021-34968377-78 Karachi 10-20% Diagnostic Center 2.5 KPT Centre Karachi Port Trust Hospital Keemari, Karachi 021-34297786 Karachi 10-20% Diagnostic Center 021-34620176 021- 2.6 Gulistan-E-Johar Centre S -

PESA-DP-Hyderabad-Sindh.Pdf
Rani Bagh, Hyderabad “Disaster risk reduction has been a part of USAID’s work for decades. ……..we strive to do so in ways that better assess the threat of hazards, reduce losses, and ultimately protect and save more people during the next disaster.” Kasey Channell, Acting Director of the Disaster Response and Mitigation Division of USAID’s Office of U.S. Foreign Disas ter Ass istance (OFDA) PAKISTAN EMERGENCY SITUATIONAL ANALYSIS District Hyderabad August 2014 “Disasters can be seen as often as predictable events, requiring forward planning which is integrated in to broader de velopment programs.” Helen Clark, UNDP Administrator, Bureau of Crisis Preven on and Recovery. Annual Report 2011 Disclaimer iMMAP Pakistan is pleased to publish this district profile. The purpose of this profile is to promote public awareness, welfare, and safety while providing community and other related stakeholders, access to vital information for enhancing their disaster mitigation and response efforts. While iMMAP team has tried its best to provide proper source of information and ensure consistency in analyses within the given time limits; iMMAP shall not be held responsible for any inaccuracies that may be encountered. In any situation where the Official Public Records differs from the information provided in this district profile, the Official Public Records should take as precedence. iMMAP disclaims any responsibility and makes no representations or warranties as to the quality, accuracy, content, or completeness of any information contained in this report. Final assessment of accuracy and reliability of information is the responsibility of the user. iMMAP shall not be liable for damages of any nature whatsoever resulting from the use or misuse of information contained in this report. -
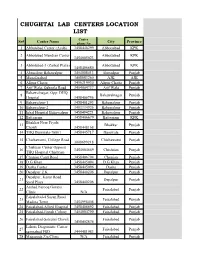
Chughtai Lab Centers Location List
CHUGHTAI LAB CENTERS LOCATION LIST Center Sr# Center Name City Province phone No 1 Abbotabad Center (Ayub) 3458448299 Abbottabad KPK 2 Abbotabad Mandian Center Abbottabad KPK 3454005023 3 Abbotabad-3 (Zarbat Plaza) Abbottabad KPK 3458406680 4 Ahmedpur Bahawalpur 3454008413 Ahmedpur Punjab 5 Muzafarabad 3408883260 AJK AJK 6 Alipur Chatta 3456219930 Alipur Chatta Punjab 7 Arif Wala, Qaboola Road 3454004737 Arif Wala Punjab Bahawalnagar, Opp: DHQ 8 Bahawalnagar Punjab Hospital 3458406756 9 Bahawalpur-1 3458401293 Bahawalpur Punjab 10 Bahawalpur-2 3403334926 Bahawalpur Punjab 11 Iqbal Hospital Bahawalpur 3458494221 Bahawalpur Punjab 12 Battgaram 3458406679 Battgaram KPK Bhakhar Near Piyala 13 Bhakkar Punjab Chowk 3458448168 14 THQ Burewala-76001 3458445717 Burewala Punjab 15 Chichawatni, College Road Chichawatni Punjab 3008699218 Chishtian Center Opposit 16 3454004669 Chishtian Punjab THQ Hospital Chishtian 17 Chunian Cantt Road 3458406794 Chunian Punjab 18 D.G Khan 3458445094 D.G Khan Punjab 19 Daska Center 3458445096 Daska Punjab 20 Depalpur Z.K 3458440206 Depalpur Punjab Depalpur, Kasur Road 21 Depalpur Punjab Syed Plaza 3458440206 Arshad Farooq Goraya 22 Faisalabad Punjab Clinic N/A Faisalabad-4 Susan Road 23 Faisalabad Punjab Madina Town 3454998408 24 Faisalabad-Allied Hospital 3458406692 Faisalabad Punjab 25 Faisalabad-Jinnah Colony 3454004790 Faisalabad Punjab 26 Faisalabad-Saleemi Chowk Faisalabad Punjab 3458402874 Lahore Diagonistic Center 27 Faisalabad Punjab samnabad FSD 3444481983 28 Maqsooda Zia Clinic N/A Faisalabad Punjab Farooqabad, -

Islamabad: Rawalpindi: Lahore: Karachi: Quetta
Contact list – Photo Studios - Pakistan The list below of photo studios in Pakistan has been compiled by the Australian High Commission, based on past experience, for client convenience only. The Australian High Commission does not endorse any of the photo studios appearing in the list, provides no guarantees as to their quality and does not accept any liability if you choose to engage one of these photo studios. Islamabad: Simco Photo Studio and Digital Colour Lab Photech Block 9-E, School Road, F-6 Markaz, Super Shop No. 7, Block 12, School Road, F-6 Markaz, Market, Islamabad – Pakistan, Super Market, Islamabad 051-2822600, 051-2826966 051-2275588, 051-2874583 Rawalpindi: Lahore: Jumbo Digital Lab & Photo Studio AB Digital Color Lab and Studio Chandni Chowk, Murree Road, Rawalpindi Kashif Centre, 80-Chowk Nisbat Road 051-4906923, 051-4906089, 051-4456088 Lahore – Pakistan, 042-37226496, 042-37226611 Karachi: Dossani’s Studio Disney’s Digital Photo Studio Hashoo Terrace, Khayaban-e-Roomi, Boat Basin, Shop No. 3, Decent Tower Shopping Centre, Clifton , Karachi, Gulistan-e-Johar, Block 15, Karachi Tell: +92-21-34013293, 0300-2932088 021-35835547, 021-35372609 Quetta: Sialkot Yadgar Digital Studio Qazi Studio Hussain Abad, Colonal Yunas Road, Hazara Qazi Mentions Town, Quetta. 0343-8020586 Railay Road Sialkot – Pakistan 052-4586083, 04595080 Peshawar: Azeem Studio & Digital Labs 467-Saddar Road Peshawar Cantt Tell: +91-5274812, +91-5271482 Camera Operator Guidelines: Camera: Prints: - High-quality digital or film camera - Print size 35mm -

NATIONAL HIGHWAY AUTHORITY Procurement & Contract Admini.Stration Sedion 28-Mauve Area, G-9/L,Islamabad Tel 9032727, Fax: 9260419
t NATIONAL HIGHWAY AUTHORITY Procurement & Contract Admini.stration Sedion 28-Mauve Area, G-9/L,Islamabad Tel 9032727, Fax: 9260419 Ref:6(441)/GM (P&cA)/NH /L7 I In 3 y'k nugort,2oLT Director General, Public Procurement Regulatory Authority, lst Floor FBC building near State Bank, G-5/2, Islamabad Subject: AUUOUMBMENT OF EVALUATION REPORT |PPRA RULE-351: Consultancy Senrlces for Detailed Design and Constnrction Supervision of Lahore - Sialkot Motorway (LSlMl Link Highway (4 Lanel connectlng LSM to NaranE Mandi and Narowal (73 I(m Approx.l Reference: PPRARule-S5 Kindly find attached the duly filled and signed evaluation report along with Annex-I pertaining to tJre procurement of subject services in view of the above referred PPRA Rule-35 for uploading on your website at earliest, please. //d (MUHAMMAD AZANTI Director (P&CA) Enclosure : Evaluation Report alongrith Annex-I. Copy for kind information to: - Member (Engineering-Coordination), NHA, - General Manager (P&CA). 5 EVAL N REP 1. Nameof ProcuringAgency: NationalHighway Authority 2. Methodof Procurement: SingleStage Two Envelop Procedure 3. Titleof Procurement: ConsultancyServices for DetailedDesign and ConstructionSupervision of Lahore- Sialkot Motoruvay(LSM) Link Highway (4 Lane)connecting LSMto NarangMandi and Narowal (73 Km Approx.) 4. Tenderlnquiry No.: 6(441yGM(P&CAyNHNlTt 5. PPRARef. No. (TSE): TS315425E 6. Date& Time of Bid Closing: 6s June,2017 at 1130hours local time 7. Date& Timeof BidOpening: 6h June,2Q17 at 1200hours localtime 8. No of BidsReceived: Six (06)proposals were received 9. Criteriafor BidEvaluation: Criteriaof BidEvaluation is attachedat Annex-l 10. Detailsof Bid(s)Evaluation: As below Marks Evaluated Rule/Regu lation/SBD"/Pol icy/ Nameof Bidder Cost Basis for Rejection/ Technical Financial (Pak.Rs.) Acceptance as per Rule 35 (if applicable) (if applicable) of PP Rules,2OO4. -

Old-City Lahore: Popular Culture, Arts and Crafts
Bāzyāft-31 (Jul-Dec 2017) Urdu Department, Punjab University, Lahore 21 Old-city Lahore: Popular Culture, Arts and Crafts Amjad Parvez ABSTRACT: Lahore has been known as a crucible of diversified cultures owing to its nature of being a trade center, as well as being situated on the path to the capital city Delhi. Both consumers and invaders, played their part in the acculturation of this city from ancient times to the modern era.This research paperinvestigates the existing as well as the vanishing popular culture of the Old-city Lahore. The cuisine, crafts, kites, music, painting and couture of Lahore advocate the assimilation of varied tastes, patterns and colours, with dissimilar origins, within the narrow streets of the Old- city. This document will cover the food, vendors, artisans, artists and the red-light area, not only according to their locations and existence, butin terms of cultural relations too.The paper also covers the distinct standing of Lahore in the South Asia and its popularity among, not only its inhabitants, but also those who ever visited Lahore. Introduction The Old City of Lahore is characterized by the diversity of cultures that is due tovarious invaders and ruling dynasties over the centuries. The narrow streets, dabbed patches of light andunmatched cuisine add to the colours, fragrance and panorama of this unique place. 22 Old-city Lahore: Popular Culture, Arts and Crafts Figure 1. “Old-city Lahore Street” (2015) By Amjad Parvez Digital Photograph Personal Collection Inside the Old-city Lahore, one may come the steadiness and stationary quality of time, or even one could feel to have been travelled backward in the two or three centuries when things were hand-made, and the culture was non-metropolitan. -

Calculus Renal Failure; a Study to Profile the Calculus Renal Failure and Its 1
CALCULUS RENAL FAILURE The Professional Medical Journal www.theprofesional.com ORIGINAL PROF-4941 DOI: 10.29309/TPMJ/18.4941 CALCULUS RENAL FAILURE; A STUDY TO PROFILE THE CALCULUS RENAL FAILURE AND ITS 1. MCPS (Surgery), FCPS (Urology) SIU Fellow Urology Nephrology MANAGEMENT STRATEGY Centre Mansoura Egypt Fellowship in Uro Oncology Assistant Professor of Urology Azfar Ali1, Ghulam Ghous2, Zakariya Rashid3, Nabeel Shafi4, Irshad Ali5, Department of Urology & Renal Muhammad Hassam Khalid6, Muhammad Safdar Khan7 Transplant AMC/PGMI/Lahore General Hospital ABSTRACT… Background: Urolithiasis is a common urological disease in Pakistan. Calculus Lahore. renal failure is a urological emergency that required immediate intervention to prevent further 2. FCPS Urology Senior Registrar Urology deterioration of renal function. Objectives: The purpose of this study is to present clinical profile SIMS/Services Hospital Lahore. of calculus renal failure patient and to report our experience of management of such patients. 3. FCPS, MRCS(Ed) Study Design: Descriptive Cross sectional study. Setting and Period: Department of urology Assistant Professor Surgery Aziz Fatima Medical & Dental Services Hospital from July 2015 to December 2016 were included. Materials and Methods: College Faisalabad. Patients of all ages of either sex who presented with calculus renal failure. The patients with 4. FCPS Urology obstructive uropathy due to causes other than stone disease were excluded. Demographic Senior Registrar Urology information along with detailed history recorded. Baseline investigations included Complete SIMS/Services Hospital Lahore. 5. MBBS blood counts, serum creatinine, serum electrolytes and ultrasound for KUB. For stone position Registrar Urology Xray KUB in every case & CT in selected cases performed. Functional status of individual kidney SIMS/Services Hospital Lahore. -

Investigation on the Prevalence of Leukaemia at a Tertiary Care Hospital, Lahore
INVESTIGATION ON THE PREVALENCE OF LEUKAEMIA AT A TERTIARY CARE HOSPITAL, LAHORE NIGHAT NASIM, KALIMUDDIN MALIK, NAUMAN A. MALIK SHAISTA MOBEEN, SAUD AWAN AND NAGHMANA MAZHAR Department of Pathology, PGMI / Lahore General Hospital, Lahore ABSTRACT Introduction: Cancer in all forms is causing about 12% deaths throughout the world. After recent advances and improvement in treatment and prevention in cardiovascular diseases, tumour is an important cause of morbidity and mortality. 1 The incidence of leukaemia across the world is 1 per 100,000 annually. It contributes to 25% of childhood cancers. 2 The study was designed to investi- gate the Prevalence of Leukemia subtypes at Lahore General Hospital / The Graduate Medical Insti- tute, Lahore and was carried out in the Bone Marrow Clinic. The study was cross – sectional pros- pective. The period of the study was two year from 01 June, 2010 to 30 June, 2012. Methodology: Complete blood counts, bone marrow aspiration and trephine biopsies were perfor- med according to standard methods. Results: In a total of 45 cases of leukaemia, acute leukemia was more prevalent than chronic leu- kaemia. The ratio of acute and chronic leukaemias was 4:1. Male to female ratio was 1.3: 1. Most of the patients (42%) were below the age of 15 years. ALL (49%) was more common than AML (31%). Among chronic leukaemias, CML (16%) was more common than CLL (2%) and CMML (2%). The study of acute leukaemia subtypes revealed that ALL – L2 was more common (77%) than L 1 (24%). In AML subtypes, M3 (57%) was most prevalent while M 2 (14%) and M 4 (14%) and M 1 (7%) and M 6 (7%) were less prevalent of leukaemia subtypes. -

Curriculum Vitae Prof.Dr. Khalid Mahmood M.B.B.S Frcs,Frcs(Sn)
CURRICULUM VITAE PROF.DR. KHALID MAHMOOD M.B.B.S FRCS,FRCS(SN) INTERCOLLEGIATE BOARD IN NEUROSURGERY UK ENDOSCOPIC SKULL BASE FELLOWSHIP OHIO STATE UNIVERSITY USA PROFESSOR & HEAD NEUROSURGERY UNIT II POSTGRADUATE MEDICAL INSTITUTE/ AMEER-UD-DIN MEDICAL COLLEGE/ LAHORE GENERAL HOSPITAL,LAHORE E-MAIL [email protected] QUALIFICATIONS MBBS (FEB 1987) PUNJAB , PAKISTAN FRCS (OCTOBER 1992) GLASGOW , UK FRCS (SURGICAL NEUROLOGY) (OCTOBER 1998) Intercollegiate Board Neurosurgery Royal college of Surgeons UK&Ireland ENDOSCOPIC SKULL BASE FELLOWSHIP OHIO STATE UNIVERSITY USA 2014 PRESENT APPOINTMENT PROFESSOR & HEAD NEUROSURGERY UNIT II PGMI/AMC/LGH, JOB DESCRIPTION I am working as Professor of Neurosurgery and Head Unit II at Postgraduate Medical Institute/Ameer-ud-Din Medical College/Lahore General Hospital, Lahore. This Neurosurgery Department is oldest in Punjab and being leader of Neurosurgery in Pakistan for last 50 years, has contributed enormously to development of Neurosurgery and Public sector service. The clinical work is divided among three independently functioning Neurosurgery Units. Every year we attract the highest number of postgraduate trainees and Senior Registrars. This indeed is the most sought after professorial position in the country. I take pride in teaching and training postgraduates, Senior Registrars and junior Consultants while at the same time keeping myself updated all the time through National and international workshops, meetings and conferences. This means regular didactic teaching rounds, journal club, morbidity & mortality meetings, development of SOPs, Surgical Audit, pre- operative demonstration of surgical technique in skill laboratory, demonstration of new neurosurgical techniques, innovation and keen supervision during operative procedures. My job is to ensure conducive environment to execute above activities which is reflected by our personal “STICH SKILL Lab” and library with indexed journals and Audio visual aids. -

19 Laboratory Capacity National Institute of Health, Islamabad 28 June 2021
COVID – 19 Laboratory Capacity National Institute of Health, Islamabad 28 June 2021 S. No. Province/ City Category Functional Lab/Site Region (No) 1. Federal Islamabad Public National Institute of Health - (NIH) 2. (35) (35) PIMS – (POCT + PCR) 3. Private Islamabad Diagnostic Center (IDC) 4. Biotech Lab and Research Center 5. Metropole Laboratories 6. Capital Diagnostic Centre 7. Biogene 8. Shifa International 9. Excel Labs 10. Global Clinical Care Diagnostic Centre 11. Temar Diagnostics 12. Margalla Diagnostics and Clinics 13. Advanced Diagnostics Centre 14. Kulsum Intl Hospital 15. Maroof Hospital 16. Nayab Labs 17. Medikay Pvt limited 18. Akbar Niazi Teaching Hospital 19. Real Time PCR Diagnostic, Research & Reference Laboratories 20. Shaafi Hospital PWD 21. Crown Diagnostic Centre 22. Shaheen Medical Laboratories & Health Services 23. DAHA Lab and Diagnostic 24. Rehman Laboratories 25. Islamabad Health Care Laboratory 26. Biomaxx Lab and Diagnostic Centre 27. Ali Medical Centre 28. Ideal Labs & Diagnostic Center 29. European Diagnostic Center 30. BEKS Advanced Medical Services (Pvt) Ltd 31. Global Research and Reference Laboratories 32. Sharif Labs and Diagnostics (Pvt) Ltd 33. Nimra Diagnostic Centre (NDC) 34. Public/Private MedAsk 35. IHITC Lab 36. Punjab Lahore Public Punjab AIDS Control Program incl Hepatitis Lab 37. (77) (39) Punjab Forensic Science Auth Lab 38. Jinnah Hospital 39. PKLI 40. Lahore General Hospital 41. CAMB 42. UVAS (BSL-3) 43. Lahore TB Program (BSL-3) 44. IPH Lahore 45. Private Chughtai Lab 46. Shaukat Khanum Memorial Hospital 47. Islamabad Diagnostic Center (IDC) 48. Rahila Research and Reference Lab 49. Venus Diagnostics 50. Hameed Lateef Hospital 51. Citilab & Research Centre 52.