Feb Issue No.1 Final 24-02-10 6.48 PM.Pmd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Alphabetical List of Persons for Whom Recommendations Were Received for Padma Awards - 2015
Alphabetical List of Persons for whom recommendations were received for Padma Awards - 2015 Sl. No. Name 1. Shri Aashish 2. Shri P. Abraham 3. Ms. Sonali Acharjee 4. Ms. Triveni Acharya 5. Guru Shashadhar Acharya 6. Shri Gautam Navnitlal Adhikari 7. Dr. Sunkara Venkata Adinarayana Rao 8. Shri Pankaj Advani 9. Shri Lal Krishna Advani 10. Dr. Devendra Kumar Agarwal 11. Shri Madan Mohan Agarwal 12. Dr. Nand Kishore Agarwal 13. Dr. Vinay Kumar Agarwal 14. Dr. Shekhar Agarwal 15. Dr. Sanjay Agarwala 16. Smt. Raj Kumari Aggarwal 17. Ms. Preety Aggarwal 18. Dr. S.P. Aggarwal 19. Dr. (Miss) Usha Aggarwal 20. Shri Vinod Aggarwal 21. Shri Jaikishan Aggarwal 22. Dr. Pratap Narayan Agrawal 23. Shri Badriprasad Agrawal 24. Dr. Sudhir Agrawal 25. Shri Vishnu Kumar Agrawal 26. Prof. (Dr.) Sujan Agrawal 27. Dr. Piyush C. Agrawal 28. Shri Subhash Chandra Agrawal 29. Dr. Sarojini Agrawal 30. Shri Sushiel Kumar Agrawal 31. Shri Anand Behari Agrawal 32. Dr. Varsha Agrawal 33. Dr. Ram Autar Agrawal 34. Shri Gopal Prahladrai Agrawal 35. Shri Anant Agrawal 36. Prof. Afroz Ahmad 37. Prof. Afzal Ahmad 38. Shri Habib Ahmed 39. Dr. Siddeek Ahmed Haji Panamtharayil 40. Dr. Ranjan Kumar Akhaury 41. Ms. Uzma Akhtar 42. Shri Eshan Akhtar 43. Shri Vishnu Akulwar 44. Shri Bruce Alberts 45. Captain Abbas Ali 46. Dr. Mohammed Ali 47. Dr. Govardhan Aliseri 48. Dr. Umar Alisha 49. Dr. M. Mohan Alva 50. Shri Mohammed Amar 51. Shri Gangai Amaren 52. Smt. Sindhutai Ramchandra Ambike 53. Mata Amritanandamayi 54. Dr. Manjula Anagani 55. Shri Anil Kumar Anand 56. -

South India to North America Journey of Journalist
South India to North America Journey of Journalist South India to North America Journey of Journalist Narisetti Innaiah South India to North America Journey of Journalist Page 1 Contents 1. Childhood - Sweet and Sour 4 2. Twists and turns at college level 11 3. College life is not that smooth (1953-58) 15 4. University Education 28 5. Taste of Politics 32 6. Untrained teacher 38 7. Entered Married Life 43 8. Encounter Different Personalities 47 9. Beyond Religion 49 10. A.B.Shah - Leader of Secular Movement 52 11. Joyful Life - Naveena, Raju 56 12. Can Reason Appeal 58 13. Komala Unique Person 60 14. Meandering into Research 63 15. Facing New Phase 66 16. Friendship with Chief Justice 68 17. A Decade of Experience 71 18. Reporting Legislative discussions 74 19. Helping Elected Representatives 78 20. Joyful Humanism 80 19. Bureau chief of Telugu daily 82 20. V.R. Narla dedicates his last play 89 21. Writer with human face 92 22. Chief Minister with difference 95 23. A friend in deed 98 South India to North America Journey of Journalist Page 2 24. Facing hardships 104 25. Encounter with academic cheats 107 26. At last owned a house 113 27. Unscientific alternatives 116 28. Playing with blind believers 119 29. Widening humanist horizon 128 30. Friendship with Rationalist, Skeptics 135 31. Feeling the Cosmos 141 32. India once again 145 33. Regional Associations in America 154 34. Thinkers groups 157 36. A story of Thesis 160 37. Pictures to remember South India to North America Journey of Journalist Page 3 111.1.. -

State Bank of India - 4388 1 P
SOUVENIR - 2017 STATE BANK OF INDIA - 4388 1 P . DAST AGIRI REDDY NANDY AL 76 S. B. RAMA KRISHNA ADONI 151 R. SHARSCHANDRA ALLAGADDA 2 P . GOWRI NANDY AL 77 N. DHARANI ADONI 152 P . SRINIV ASULU ALLAGADDA 3 K. DIVY A RAGHA VENDRA A. KODUR 78 K. HARI PRASAD ADONI 153 E. NARASIMHAM ALLAGADDA 4 TEEGA RAMADEVI A.MUPP ALLA 79 KOMALA BHARA TH KUMAR ADONI 154 K. INDRAJA ALLAGADDA 5 S. CHANDRA SEKHAR A.P ALLI 80 M.P . LA V ANY A ADONI 155 G . VISWESW ARAIAH ALLAGADDA 6 MA T ALA YERRINAIDU A.PURAM 81 M. CHOLARAJU ADONI 156 P . SUDHAKAR REDDY ALLAGADDA 7 RASAD DHARAMIREDDY A.PURAM 82 N. SRIDHAR ADONI 157 B. VIJA Y A LAKSHMI ALLAGADDA 8 KOLA GOV ARDHAN ABBASAHEBPET A 83 B. RA VINDRA ADONI 158 M. RAMANA REDDY ALLAGADDA 9 G . CHANDRA SEKAR REDDY ACHAMPET 84 S. AMARNA THA REDDY ADONI 159 B. NAGABHUSHANAM ALLAP ADU 10 T . ESMAIL ACHAMPET 85 S. RA VI KUMAR ADONI 160 K. SOWJANY A RANI ALLUR V ARIP A TNAM 1 1 K. YELLA SWAMY ACHAMPET 86 SURE KRISHNA ADONI 161 KELLA MURTHI ALUGOLU 12 CHIKKUDU SHEKHAR ACHAMPET 87 S. RIZWANA ADONI 162 V . KOTESW ARA REDDY ALUR 13 SURESH MUDA V A TH ACHAMPET 88 B. VEERESHAMMA ADONI 163 K. CHINNA BABU ALUR 14 M. BHASKAR ACHAMPET 89 C. PRAKASH ADONI 164 B. RAJA SEKHARA REDDY ALUR 15 P . PAR THASARADHI ACHAMPET 90 N. USHA RANI ADONI 165 H.B. RA VIKUMAR GOUD ALUR 16 M. P . CHAKRA V AR THY ACHAMPET 91 B. -

Alphabetical List of Recommendations Received for Padma Awards - 2014
Alphabetical List of recommendations received for Padma Awards - 2014 Sl. No. Name Recommending Authority 1. Shri Manoj Tibrewal Aakash Shri Sriprakash Jaiswal, Minister of Coal, Govt. of India. 2. Dr. (Smt.) Durga Pathak Aarti 1.Dr. Raman Singh, Chief Minister, Govt. of Chhattisgarh. 2.Shri Madhusudan Yadav, MP, Lok Sabha. 3.Shri Motilal Vora, MP, Rajya Sabha. 4.Shri Nand Kumar Saay, MP, Rajya Sabha. 5.Shri Nirmal Kumar Richhariya, Raipur, Chhattisgarh. 6.Shri N.K. Richarya, Chhattisgarh. 3. Dr. Naheed Abidi Dr. Karan Singh, MP, Rajya Sabha & Padma Vibhushan awardee. 4. Dr. Thomas Abraham Shri Inder Singh, Chairman, Global Organization of People Indian Origin, USA. 5. Dr. Yash Pal Abrol Prof. M.S. Swaminathan, Padma Vibhushan awardee. 6. Shri S.K. Acharigi Self 7. Dr. Subrat Kumar Acharya Padma Award Committee. 8. Shri Achintya Kumar Acharya Self 9. Dr. Hariram Acharya Government of Rajasthan. 10. Guru Shashadhar Acharya Ministry of Culture, Govt. of India. 11. Shri Somnath Adhikary Self 12. Dr. Sunkara Venkata Adinarayana Rao Shri Ganta Srinivasa Rao, Minister for Infrastructure & Investments, Ports, Airporst & Natural Gas, Govt. of Andhra Pradesh. 13. Prof. S.H. Advani Dr. S.K. Rana, Consultant Cardiologist & Physician, Kolkata. 14. Shri Vikas Agarwal Self 15. Prof. Amar Agarwal Shri M. Anandan, MP, Lok Sabha. 16. Shri Apoorv Agarwal 1.Shri Praveen Singh Aron, MP, Lok Sabha. 2.Dr. Arun Kumar Saxena, MLA, Uttar Pradesh. 17. Shri Uttam Prakash Agarwal Dr. Deepak K. Tempe, Dean, Maulana Azad Medical College. 18. Dr. Shekhar Agarwal 1.Dr. Ashok Kumar Walia, Minister of Health & Family Welfare, Higher Education & TTE, Skill Mission/Labour, Irrigation & Floods Control, Govt. -
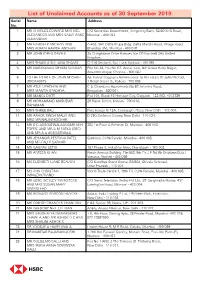
List of Unclaimed Accounts As of 30 September 2019. Serial Name Address No
List of Unclaimed Accounts as of 30 September 2019. Serial Name Address No. 1 MR CHARLES EDWARD MICHAEL C/O Securtiies Department, Hongkong Bank, 52/60 M G Road, ALEXANDER AND MRS SALLY ANNE Mumbai - 400 023 ALEXANDER 2 MR HARISH P ANCHAN AND A-402, Shri Datta Krupa Bldg, Datta Mandir Road, Village Road, MRS ROHINI HARISH ANCHAN Bhandup (W), Mumbai - 400 078. 3 MR JOHN IDRES DAVIES 25 Claughbane Drive Ramsey Isle Of Man Im8 2Ay United Kingdom. 4 MRS SHAKILA SULTANA SHAMS Cl-176 Sector-II, Salt Lake, Kolkata - 700 091. 5 MR NARAYANAN SHYAM SUNDAR Plot No 34, Flat No G2, Annai Illam, 6th Street Balaji Nagar, Alwarthirunagar, Chennai - 600 087. 6 TO THE ESTATE OF JOHN MICHAEL Ajit Kumar Dasgupta Administrator To The Estate Of John Michael, (DECEASED) 1 British Indian St, Kolkata - 700 069. 7 MR ATUL UPADHYA AND C-5, Chandana Apartments No 82, Infantry Road, MRS MAMTA UPADHYA Bengaluru - 560 001. 8 MR MANOJ DUTT Flat 101, Block 45 Heritage City, Gurgaon - 122 002. 4013739 9 MR MOHAMMAD MASUDAR 28 Ripon Street, Kolkata - 700 016. RAHAMAN 10 MRS SHREE BALI Punj House M 13A, Connaught Place, New Delhi - 110 001. 11 MR ASHOK SINGH MALIK AND D-250, Defence Colony, New Delhi - 110 024. MRS MRINALINI KOCHAR 12 MR S D AGBOATWALAANDMR M H 282 1st Floor A Rehman St, Mumbai - 400 003. TOFFIC AND MR A M PATKA (DEC) AND MR A A AGBOATWALA 13 MR JEHANGIR PESTONJI PATEL Gulestan, Cuffe Parade, Mumbai - 400 005. AND MR FALI P SARKARI 14 MR GAURAV SETHI 157 Phase II, Industrial Area, Chandigarh - 160 002. -

Stateandhra PRADESH
State ANDHRA PRADESH Address -1 NEAR RAILWAY GATE Address -2 GUNJ ROAD City ADILABAD Pin Code 504 001 State ANDHRA PRADESH Zone SOUTH STD Code 08732 TEL 1 230777 TEL -2 FAX -1 230777 ContactPerson DR G PRAKASH DR G PRAKASH HOSPITAL NAME ADITYA NURSING HOME Address -1 COLLEGE ROAD Address -2 City ADONI Pin Code 518 301 State ANDHRA PRADESH Zone SOUTH STD Code 08512 TEL 1 231006 TEL -2 230792 FAX -1 ContactPerson DR B SRINIVASALU HOSPITAL NAME VIJAYALAKSHMI NURSING HOME Address -1 S K D COLONY, 3RD FR. EXTENSION Address -2 KALLUMATAM City ADONI Pin Code 518 301 State ANDHRA PRADESH Zone SOUTH STD Code 08512 TEL 1 25 3928 TEL -2 FAX -1 25 3928 ContactPerson DR I GANGADHARA RAO SRI SAI SATYANARAYANA NURSING HOSPITAL NAME HOME Address -1 VARADAVARI QUARTERS Address -2 MAIN ROAD City AMADALAVALASA Pin Code 532 185 State ANDHRA PRADESH Zone SOUTH STD Code 08942 TEL 1 28 6436 TEL -2 FAX -1 28 6436 ContactPerson DR P TATAYYALU HOSPITAL NAME V N NURSING HOME Address -1 D NO 3-2-117E COLLEGE ROAD Address -2 City AMALAPURAM Pin Code 533 201 State ANDHRA PRADESH Zone SOUTH STD Code 08856 TEL 1 231166 TEL -2 FAX -1 232133 ContactPerson DR CHIRANJEEVI RAJU HOSPITAL NAME AASHA HOSPITALS Address -1 7/201, COURT ROAD Address -2 City ANANTHAPUR Pin Code 515 001 State ANDHRA PRADESH Zone SOUTH STD Code 08554 TEL 1 274194 TEL -2 FAX -1 74494 ContactPerson MR NAGA RAJU HOSPITAL NAME DIVYASREE HOSPITAL Address -1 ADIMURTHY NAGAR Address -2 GUILD OF SERVICE ROAD City ANANTHAPUR Pin Code 515 002 State ANDHRA PRADESH Zone SOUTH STD Code 08554 TEL 1 274322 TEL -
![[01900000-02050000] (702Kb)](https://docslib.b-cdn.net/cover/1802/01900000-02050000-702kb-4661802.webp)
[01900000-02050000] (702Kb)
Dated : 23/4/2016 Signatory ID Name CIN Company Name Defaulting Year 01900025 KHATOD PUKHRAJ U17119GJ1993PTC020009 ALANKAR TEXTURISING 2008-09, 2009-10 SANTOSHDEVI PVT LTD 01900054 MANAGARAJ U17111TZ2006PTC013310 KEERTHANA TEXTILES 2008-09, 2009-10 MURUGASAMY MILLS PRIVATE LIMITED 01900137 KENNEDY MUTHIAH U15400TN2008PTC067049 GAYATHRI FROZEN 2008-09, 2009-10 VICTORJOHN PRODUCTS PRIVATE 01900159 PANKAJ SABOO U25209DL2001PTC112780 QUALITY FOAM 2007-08, 2008-09, 2009-10 PROCESSORS PRIVATE 01900231 SHEIKH ZAHIR U52590MP2007PTC020067 AIM INDIA MARKETING 2008-09, 2009-10 PRIVATE LIMITED 01900257 HUSSAIN NADEEM U52590MP2007PTC020067 AIM INDIA MARKETING 2008-09, 2009-10 PRIVATE LIMITED 01900302 DEVI MAHAWAR VIDYA U67120CT2006PTC020073 GIGANTIC CAPITAL PRIVATE 2009-10 LIMITED 01900306 MANIVANNAN PRAKASH U51505TN2007PTC065588 ROYAL REF - TECH PRIVATE 2008-09, 2009-10 LIMITED 01900309 APELAGUNTA VINIL U93000TG2008PTC057437 ARROSE ADVISORY 2008-09, 2009-10 SERVICES PRIVATE LIMITED 01900314 MAHAWAR SAPNA U67120CT2006PTC020073 GIGANTIC CAPITAL PRIVATE 2009-10 LIMITED 01900317 RAVIKUMARARAJAA U20211TN1998PLC041178 SUPER PANEL LIMITED 2007-08, 2008-09, 2009-10 SINGARAVELU VINAYAGA 01900326 JATINDER KUMAR U45201PB2007PTC031492 ORA INFRASTRUCTURE 2008-09, 2009-10 PRIVATE LIMITED 01900332 KAMALEE RAJA U20211TN1998PLC041178 SUPER PANEL LIMITED 2007-08, 2008-09, 2009-10 01900343 GUPTA KSHITIJ U45400DL2008PTC172673 KVG ESTATE PRIVATE 2009-10 LIMITED 01900355 ARUN SINGARAVELU U20211TN1998PLC041178 SUPER PANEL LIMITED 2007-08, 2008-09 VINAYAGA 01900357 ALLETE VENKATRAM U51900TG2007PTC056860 THIRD EYE RECONN 2008-09, 2009-10 PRIVATE LIMITED 01900369 LAKSHMI MIKKILINENI SREE U74999TG2008PTC058270 ESSVI ENTERPRISES (INDIA) 2008-09, 2009-10 PRIVATE LIMITED 01900381 SHAUN SWEENEY U74140DL2008PTC182850 EAST LINK CONSULTING 2009-10 INDIA PRIVATE LIMITED. 01900415 FLAHERTY PAUL THOMAS U74140DL2008PTC182850 EAST LINK CONSULTING 2009-10 INDIA PRIVATE LIMITED. 01900431 ALI MUNNAWAR U18101DL2008ULT172186 SHAHNAI APPARELS 2009-10 PRIVATE LIMITED 01900457 ASHOK KUMAR U29308DL1997PTC086966 R.S. -

Investor First Name Investor Middle Name Investor Last Name Father
Unclaimed and Unpaid Dividend - FY 2010-11 Prposed date Amount of transfer to Investor First Name Investor Middle Name Investor Last Name Father / Husband First Name Address Country State Pincode DP ID / Client ID / Folio No Transferred IEPF A JAGANATHAN NA D NO 140/3 CHENNIYAPA COMPLEX PETHAM PALAYAM RD THIRUVENGADAM PALAYAM PERUNDUR ERODE INDIA Tamil Nadu 638052 IN302902-49001634-0000 120 23-Sep-2018 A K MOHANAN KUTTANPILLAI SRUTHI MANNAR CHENGANNUR INDIA Kerala 689623 12023900-00331649-GE00 276 23-Sep-2018 A KAVITHA NA PLOT NO 347 H M T HILLS OPP JNTU KUKATPALLY INDIA Andhra Pradesh 500072 IN300669-10168398-0000 30 23-Sep-2018 A LAKSHMI NARSAMMA ARAMALINGAIAH FLAT NO 101 PARIMALA RATNA VIHAR MARUTHI NAGAR KOTHAPET HYDERABAD INDIA Andhra Pradesh 500074 IN300394-14499672-0000 120 23-Sep-2018 A SUJATHA NA D NO3-10-90 KOTHA BAZAR NELLORE DIST KAVALI INDIA Andhra Pradesh 524201 12033200-04107672-GE00 1.2 23-Sep-2018 ABDUL HAFEEZ ABBASI NA 318 KANTI SIKHARA APTS PANJAGUTTA HYDERABAD INDIA Andhra Pradesh 500082 12033200-05681768-GE00 490.8 23-Sep-2018 ABDUL KAREEM KK NA KODAKKAT HOUSE HOUSE NO-3/866 OLAVANNA INDIA Kerala 673025 IN301811-10055648-0000 12 23-Sep-2018 ABHAY DUTT KAUSHIK NA 98, LOHIYAN STREET NEAR CHAMUNDA MANDIR INDIA Uttar Pradesh 246761 IN300708-10590564-0000 12 23-Sep-2018 ABHIJAT L TANNA NA C/O BANK OF PUNJAB LTD 7 SURYA MAHAL 118 NAGINDAS MASTR RD FORT MUMBAI INDIA Maharashtra 400023 GEOM0000000000018007 300 23-Sep-2018 ABHIJEET AJIT RUDRE NA TELEPHONE OFFICE AT AND POST CHOPDA TAL CHOPDA INDIA Maharashtra 425107 IN301696-10960788-0000 24 23-Sep-2018 ABHIJIT SOMNATH OZA SOMNATHOZA BLOCK NO. -
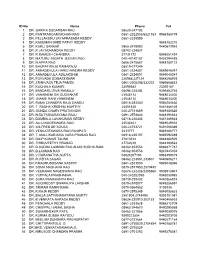
IMA APPA FSS Members List
ID No Name Phone Cell 1 DR. GARIKA SUDARSAN RAO 08623-247183 2 DR. PANTRANGAM MOHAN RAO 0861-2322038/6521163 9966365779 3 DR. PELLAKURU JAYAPRASADA REDDY 0861-2329559 4 DR. KAKUMAN SREE PATHY REDDY 9848152210 5 DR. KURLI SANKAR 0866-2478082 9440673953 6 DR. R.JAYACHANDRA REDDY 08742-224827 7 DR. R.RAMESH CHANDRA 27731772 9848051424 8 DR. MATURU JAGATH JEEVAN RAO 040-40140187 9424294455 9 DR. N.APPA RAO 0866-2478687 9848180172 10 DR. BHUPATIRAJU RAMARAJU 08819-277249 11 DR. ANNADEVULA HARICHANDRA REDDY 0861-2324801 9849048347 12 DR. ANNADEVULA ADILAKSHMI 0861-2324801 9849048347 13 DR. PUVVADA SOMASEKHAR 228568,227124 9848298939 14 DR. SRINIVASA TEJA PAMIDI 0861-2305295/332222 9949668833 15 DR. KUCHALA KUMARI 23095582 23092187 16 DR. BANDARU SIVA RAMULU 08494-224284 9396462746 17 DR. VANKINENI SAI SUDHAKAR 23548114 9848034400 18 DR. JHANSI RANI VANKINENI 23548114 9848034400 19 DR. RAMA CHANDRA RAJU DANDU 08816-283330 9866283630 20 DR. T. RADHA KRISHNA MURTHY 23351525 9441886169 21 DR. GUNDA CHARY PRATHINIDHI 040-27731659 9849180825 22 DR. N.SATYANARAYANA RAJU 0891-2574643 9848190643 23 DR. DUMBALA LAVAKUMAR REDDY 08716-220303 9347389634 24 DR. ALLU NAGESWARA RAO 23033401 9848049352 25 DR. WILFRED DE SOUZA 040-24753721 9391006389 26 DR. VENKATESWARA RAO RAVIPATI 2433777 9849186777 28 DR. T. MALLIKARJUNA VARA PRASAD RAO 08518-235197, 9885592089 29 DR. DILIP KUMAR TAUNK 27813514 9848360505 30 DR. THIRUVEETHY PRASAD 27762619 9848193532 31 DR. D.SUDHA LAXMAN RAO ALIAS SUDHA RANI 08462-653553 9866071787 32 DR. D.LAXMAN RAO 08462-653553 9247845353 33 DR. V.HARANATHA GUPTA 08924207193 9948399019 34 DR. R.VIDYA SAGAR 08462-223501,233501 9440606217 35 DR.P.MADHUSUDANA SASTRY 0861-2331509 9849048396 36 DR. -

Devnar Brouchure
DEVNAR Founder Chairman Dr. A. Saibaba Goud and the Correspondent Mrs. A. Jyothi Goud receiving accolades from top dignitories Devnar Foundation for the Blind - Scaling new hights ‘DEVNAR’ is a combination of two and motivation to make something special happen. words DEV (God) and NAR (Man), The avowed objective of Devnar Foundation for highlighting the fact that there is God the Blind is to provide opportunities for the visually in every man. If the entire humanity is challenged children in India on international the family of God, the visually standards so that they can be absorbed in the challenged children are special mainstream of society as socially productive members in it. And so, they should be individuals. In Devnar School, education, boarding given every possible opportunity to and lodging are absolutely free and any Visually develop their potentialities and latent Challenged child is admitted during any part of talents. the year. Devnar Foundation tries to unleash the Devnar Foundation started the school on 10-7- incredible capacity of students by giving 1992 with four students in a rented house. Within them value-based education and a span of 18 years, the school has grown to the enabling them to realize that within present stature with 400 students, housed in a three them can be found the skill, knowledge storeyed building owned by the Foundation. This phenomenal growth is due to the undoubted ability and unflinching enthusiasm of the founder Dr. A. Devnar Foundation for the Saibaba Goud, and his wife Mrs. Jyothi, the Blind provides all that is dedicated staff, many philanthropists and donors. -

(1954-2014) Year-Wise List 1954
MINISTRY OF HOME AFFAIRS (Public Section) Padma Awards Directory (1954-2014) Year-Wise List Sl. Prefix First Name Last Name Award State Field 1954 1 Dr. Sarvapalli Radhakrishnan BR TN Public Affairs 2 Shri Chakravarti Rajagopalachari BR TN Public Affairs 3 Shri Chandrasekhara Raman BR TN Science & Venkata 4 Dr. Satyendra Nath Bose PV WB Litt. & Edu. 5 Shri Nandlal Bose PV WB Art 6 Dr. Zakir Husain PV AP Public Affairs 7 Shri Bal Gangadhar Kher PV MAH Public Affairs 8 Shri V.K. Krishna Menon PV KER Public Affairs 9 Shri Jigme Dorji Wangchuk PV BHU Public Affairs 10 Dr. Homi Jehangir Bhabha PB MAH Science & 11 Dr. Shanti Swarup Bhatnagar PB UP Science & 12 Shri Mahadeva Iyer Ganapati PB OR Civil Service 13 Dr. Jnan Chandra Ghosh PB WB Science & 14 Shri Radha Krishna Gupta PB DEL Civil Service 15 Shri Maithilisharan Gupta PB UP Litt. & Edu. 16 Shri R.R. Handa PB PUN Civil Service 17 Shri Amarnath Jha PB UP Litt. & Edu. 21 May 2014 Page 1 of 193 Sl. Prefix First Name Last Name Award State Field 18 Shri Ajudhia Nath Khosla PB DEL Science & 19 Dr. K.S. Krishnan PB TN Science & 20 Shri Moulana Hussain Madni PB PUN Litt. & Edu. Ahmad 21 Shri Josh Malihabadi PB DEL Litt. & Edu. 22 Shri V.L. Mehta PB GUJ Public Affairs 23 Shri Vallathol Narayan Menon PB KER Litt. & Edu. 24 Dr. Arcot Mudaliar PB TN Litt. & Edu. Lakshamanaswami 25 Lt. (Col) Maharaj Kr. Palden T Namgyal PB PUN Public Affairs 26 Shri V. Narahari Raooo PB KAR Civil Service 27 Shri Pandyala Rau PB AP Civil Service Satyanarayana 28 Shri Jamini Roy PB WB Art 29 Shri Sukumar Sen PB WB Civil Service 30 Shri Satya Narayana Shastri PB UP Medicine 31 Late Smt. -

State Bank of India - 4768 1 P
SOUVENIR - 2018 STATE BANK OF INDIA - 4768 1 P . DAST AGIRI REDDY NANDY AL 76 J.RAMESH ADONI 151 E. NARASIMHAM ALLAGADDA 2 P . GOWRI NANDY AL 77 K RAJU ADONI 152 G . VISWESW ARAIAH ALLAGADDA 3 K. DIVY A RAGHA VENDRA A. KODUR 78 K. ANIL KUMAR ADONI 153 K. INDRAJA ALLAGADDA 4 T .CHAIT ANY AKUMAR REDDY A.GUDUR 79 K. BHARA TH KUMAR ADONI 154 K. SREENADHA REDDY ALLAGADDA 5 TEEGA RAMADEVI A.MUPP ALLA 80 K. HARI PRASAD ADONI 155 M. KAL Y ANI ALLAGADDA 6 S. CHANDRA SEKHAR A.P ALLI 81 K. JHANSI ADONI 156 M. MYTHILI ALLAGADDA 7 MA T ALA YERRINAIDU A.PURAM 82 K. KHAJA HUSSAIN ADONI 157 M. RAMANA REDDY ALLAGADDA 8 RASAD DHARAMIREDDY A.PURAM 83 K. LAKSHMI ADONI 158 M. SARALA DEVI ALLAGADDA 9 KOLA GOV ARDHAN ABBASAHEBPET A 84 K. LAKSHMI KANTH ADONI 159 M.V . RAMANA ALLAGADDA 10 CHIKKUDU SHEKHAR ACHAMPET 85 K. PRAKASH ADONI 160 N.V . NAGARJUNA ALLAGADDA 1 1 G . CHANDRA SEKAR REDDY ACHAMPET 86 K. RANAGASWAMY NAIDU ADONI 161 P . SRINIV ASULU ALLAGADDA 12 K. YELLA SWAMY ACHAMPET 87 K. SHALINI ADONI 162 P . SUDHAKAR REDDY ALLAGADDA 13 M. BHASKAR ACHAMPET 88 K. SOMA SEKHAR ADONI 163 R. SHARSCHANDRA ALLAGADDA 14 M. P . CHAKRA V AR THY ACHAMPET 89 K. SRIKALA ADONI 164 S. ABDUL KHA YUM ALLAGADDA 15 P . PAR THASARADHI ACHAMPET 90 K. SRIVIDY A ADONI 165 V .SUJIT KUMAR ALLAGADDA 16 SURESH MUDA V A TH ACHAMPET 91 K. SUDHINDRA ADONI 166 V ASANTHA LAKSHMI .K ALLAGADDA 17 T .