Assessment of CRVS ICT AJK
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

RFP Document 11-12-2020.Pdf
Utility Stores Corporation (USC) Tender Document For Supply, Installation, Integration, Testing, Commissioning & Training of Next Generation Point of Sale System as Lot-1 And End-to-end Data Connectivity along with Platform Hosting Services as Lot-2 Of Utility Stores Locations Nationwide on Turnkey Basis Date of Issue: December 11, 2020 (Friday) Date of Submission: December 29, 2020 (Tuesday) Utility Stores Corporation of Pakistan (Pvt) Ltd, Head Office, Plot No. 2039, F-7/G-7 Jinnah Avenue, Blue Area, Islamabad Phone: 051-9245047 www.usc.org.pk Page 1 of 18 TABLE OF CONTENTS 1. Introduction ....................................................................................................................... 3 2. Invitation to Bid ................................................................................................................ 3 3. Instructions to Bidders ...................................................................................................... 4 4. Definitions ......................................................................................................................... 5 5. Interpretations.................................................................................................................... 7 6. Headings & Tiles ............................................................................................................... 7 7. Notice ................................................................................................................................ 7 8. Tender Scope .................................................................................................................... -

S.No Institutename Enrolled Appeared Passed Promoted Fail Absent Percen
FEDERAL DIRECTORATE OF EDUCATION EXAMINATION SECTION Centralized Annual Examination Class-V,2017 **** INSTITUTION WISE RESULT BRIEFPASS/PROMOTED/FAILED/PASS PERCENTAGE/GRADES/GPA S.No InstituteName Enrolled Appeared Passed Promoted Fail Absent Percen. GPA 1 Islamabad College for Boys G-6/3, Islamabad. 349 348 314 32 2 1 99.43 4.18 2 Islamabad Model College for Boys F-7/3, Islamabad. 184 180 162 15 3 4 98.33 3.68 3 Islamabad Model College for Boys F-8/4, Islamabad. 172 171 158 12 1 1 99.42 4.50 4 Islamabad Model College for Boys I-8/3, Islamabad. 129 128 106 18 4 1 96.88 3.41 5 Islamabad Model College for Boys I-10/1, Islamabad. 145 145 142 3 0 0 100.00 4.54 6 Islamabad Model College for Boys G-10/4, Islamabad. 196 194 192 2 0 2 100.00 4.82 7 Islamabad Model College for Boys G-11/1, Islamabad. 75 75 54 15 6 0 92.00 2.79 8 Islamabad Model School ( I-V ) G-11/1, Islamabad. 65 65 50 15 0 0 100.00 2.85 9 Islamabad Model College for Boys F-10/3, Islamabad. 74 73 65 6 2 1 97.26 3.82 10 Islamabad Model School ( I-V ) F-10/1, Islamabad. 26 26 21 4 1 0 96.15 3.65 11 Islamabad Model School ( I-V ) F-10/2, Islamabad. 37 37 31 4 2 0 94.59 3.16 12 Islamabad Model School ( I-V ) F-10/4, Islamabad. -

Parcel Post Compendium Online Pakistan Post PKA PK
Parcel Post Compendium Online PK - Pakistan Pakistan Post PKA Basic Services CARDIT Carrier documents international Yes transport – origin post 1 Maximum weight limit admitted RESDIT Response to a CARDIT – destination Yes 1.1 Surface parcels (kg) 50 post 1.2 Air (or priority) parcels (kg) 50 6 Home delivery 2 Maximum size admitted 6.1 Initial delivery attempt at physical Yes delivery of parcels to addressee 2.1 Surface parcels 6.2 If initial delivery attempt unsuccessful, Yes 2.1.1 2m x 2m x 2m No card left for addressee (or 3m length & greatest circumference) 6.3 Addressee has option of paying taxes or Yes 2.1.2 1.5m x 1.5m x 1.5m Yes duties and taking physical delivery of the (or 3m length & greatest circumference) item 2.1.3 1.05m x 1.05m x 1.05m No 6.4 There are governmental or legally (or 2m length & greatest circumference) binding restrictions mean that there are certain limitations in implementing home 2.2 Air parcels delivery. 2.2.1 2m x 2m x 2m No 6.5 Nature of this governmental or legally (or 3m length & greatest circumference) binding restriction. 2.2.2 1.5m x 1.5m x 1.5m Yes (or 3m length & greatest circumference) 2.2.3 1.05m x 1.05m x 1.05m No 7 Signature of acceptance (or 2m length & greatest circumference) 7.1 When a parcel is delivered or handed over Supplementary services 7.1.1 a signature of acceptance is obtained Yes 3 Cumbersome parcels admitted No 7.1.2 captured data from an identity card are Yes registered 7.1.3 another form of evidence of receipt is No Parcels service features obtained 5 Electronic exchange of information -

List of Ngos
Registration Sr. Name of NGO Address Status(Reg No,& No Date & Relevant Law Malot Commercial Center, Shahpur VSWA/ICT/494 ,Date: 1. Aas Welfare Association Simly Dam Road, Islamabad. 051- 6/9/2006, VSWA 2232394, 03005167142 Ordinance 1961 VSWA/ICT/439, Village Khana Dak, Madina Town, Date:31/3/2004, 2. Abaseen Welfare Society Jabbah, Barma Chowk, Islamabad. VSWA Ordinance 03005308511 1961 Office No.5, 1st Floor, A & K Plaza, F- VSWA/ICT/511,Date 3. Acid Survivors Foundation. 10 Markaz, Islamabad. 051-2214052, 02/08/2007, VSWA 03008438984 Ordinance 1961 VSWA/ICT/282, Date Ali Pur Frash Lehtrar Road, 4. Akhmat Welfare Centre 24/04/1998, VSWA Islamabad. 051-2519062 Ordinance 1961 Al Mustafa Towers VSWA/ICT/438, Date # 204, Al Mustafa Towers F-10 5. Residents Associations 27/03/2004,VSWA Markaz, Islamabad. 03458555872 (AMPTRWA) Ordinance 1961 VSWA/ICT/520, Date Al-Firdous Welfare Mohallah Ara, Bharakau, Islamabad. 6. 2/04/2008, VSWA Association 051-2512308, 03008565227 Ordinance 1961 VSWA/ICT/261,Date:0 Model Village Ali Pur Farash 7. Al-Itehad Welfare Society 5/08/1996, VSWA Islamabad. Ordinance 1961 VSWA/ICT/202,Date:1 NearF.G.Boys High School Shahdra 8. Al-Jihad Youth Organization 7/06/1993,VSWA Islamabad Ordinance 1961 VSWA/ICT/377, Date H.No.39 Gali No.67 I- 9. Al-Noor Foundation. 17.4.2002, VSWA 10/1,Islamabad.051-4443227 Ordinance 1961 VSWA/ICT/90, Date 10. Al-Noor Islamic Center Rawal Town Islamabad 2.12.1990 VSWA Ordinance 1961 VSWA/ICT/89, Date 11. Al-Noor Islamic Center Sharifabad Tarlai Islamabad 2.12.1990 VSWA Ordinance 1961 VSWA/ICT/271, Date PEC Building, Ataturk Avenue, G-5/2, 12. -
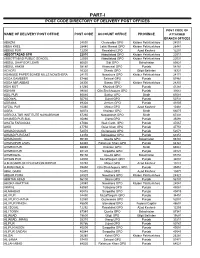
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Male / Co-Education) and Male Head of Institution at Ssc Level Upto 14-07-2021
1 LIST OF AFFILIATED INSTITUTIONS WITH STATUS (MALE / CO-EDUCATION) AND MALE HEAD OF INSTITUTION AT SSC LEVEL UPTO 14-07-2021 Inst Inst Principal S.No Inst Adress Gender Principal Name Phone No Principal Mobile No level Code Gender Angelique School, St.No.81, Embassy 051-2831007-8, 1. SSC 1002 Co-Education Maj (R) Nomaan Khan MALE 0321-5007177 Road, G-6/4, Islamabad 0321-5007177 Sultana Foundation Boys High School, 2. SSC 1042 Farash Town, Lehtrar Road (F.A), MALE WASEEM IRSHAD MALE 051-2618201 (Ext 152) 0315-7299977 Islamabad Scientific Model School, 25-26, Humak 051-4491188 , 3. SSC 1051 Co-Education KHAWAJA BASHIR AHMAD MALE 0345-5366348 (F.A), Islamabad 0345-5366348 Fauji Foundation Model School, Chak Wing Cdre Muhammad Laeeq 051-2321214, 4. SSC 1067 Co-Education MALE 0320-5635441 Shahzad Campus (F.A), Islamabad. Akhtar 0321-4044282 Academy of Secondary Education, Nai 051-4611613, 5. SSC 1070 Abadi G.T Road, Rewat (F.A), Co-Education Mr. AZHAR ALI SHAH MALE 0314-5136657 0314-5136657 Islamabad National Public Secondary School, G. 051-4612166, 6. SSC 1077 Co-Education IRFAN MAHMOOD MALE 03005338499 T Road, Rewat (F.A), Islamabad 0300-5338499 National Special Education Centre for 9260858, 7. SSC 1080 Physically Handicapped Children, G- Co-Education Islam Raziq MALE 0333-0732141 9263253 8/4, Islamabad Oxford High School, 413, Street No 43, 8. SSC 1083 Co-Education Lt. Col. Zafar Iqbal Malik (Retd) MALE 051-2253646 0321-5010789 Sector G-9/1, Islamabad Rawat Residential College, college 9. SSC 1090 Co-Education Tanzeela Malik Awan MALE 051-2516381 03465296351 Road, Rawat (F.A), Islamabad Sir Syed Ideal School System, House 10. -

Abbreviations and Acronyms
P ART III] THE GAZETTE OF PAKISTAN, EXTRA., JANUARY 15, 2020 61 ISLAMABAD, WEDNESDAY, JANUARY 15, 2020 PART III Other Notifications, Orders, etc. GOVERNMENT OF PAKISTAN OFFICE OF THE ADDL: DEPUTY COMMISSIONER (REVENUE)/ DISTRICT COLLECTOR, ICT ISLAMABAD NOTIFICATION Islamabad, the 15th January, 2020 No.36/1(192)-DRA.—In exercise of the powers conferred upon me under provision of Section 27-A of Stamp Act, 1899, the value of the immoveable properties in respect of Revenue Estates/Mouzas falling within the revenue limits of Islamabad Capital Territory specified in column (4) are hereby notified as per column (5), thereof. (2) As far as the Sectoral Areas / Industrial Areas / Agro / Poultry / Vegetable Farm / Fruit & Vegetable Markets etc. are concerned, the value of immovable properties have already been notified by Federal Board of Revenue vide S.R.O No.834(I)/2019 dated 23-07-2019 and same stands applicable. (61) Price : Rs. 80.00 [5050(2020)/Ex. Gaz.] 62 THE GAZETTE OF PAKISTAN, EXTRA., JANUARY 15, 2020 [PART III (3) As far as the immovable properties in Revenue Estates / Mouzas of Islamabad Capital Territory partially falling within District Rawalpindi and having revenue record with the office of District Collector, Rawalpindi are concerned, the value/rates notified by the District Collector, Rawalpindi shall stand applicable. (4) This notification shall come into force with immediate effect. ISLAMABAD VALUATION OF IMMOVABLE PROPERTIES MOHRA NOOR, QANUNGOI, TEHSIL & DISTRICT ISLAMABAD Qanungoi Mouza Classification Khasra No. Rates (Per Marla) in Rupees 1 2 3 4 5 Mohra Mohra Commercial 256 to 263, 291 to 294, 297, 298, 333 to 12,00,000 Noor Noor 335, 337, 341 to 343, 345, 346, 350, 351, 353, 354, 357, 358, 360, 362, 410, 411, 413, 414, 416, 417, 522, 542 to 549, 591 to 594, 541, 598, 609 to 612, 617 to 620, 631, 632, 636, 637, 640, 643 to 647, 649 to 652. -
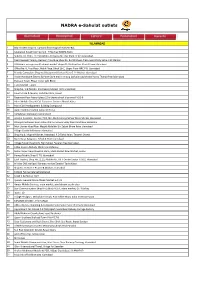
Active Franchise List ~ NADRA.Xlsx
NADRA e-Sahulat outlets ISLAMABAD 1 Bilal traders shop no 7 ground floor mughal market I‐8/1 2 Islamabad Karachi company G ‐ 9 Markaz NADRA Kisok 3 Subicca Inc. H.No. 112 Street No 70 Opposite Filter Plant G 9/3 Islamabad. 4 Pearl Iceream,Yammy Icecream franchise,Shop No. B‐2,Shaheen Plaza,near Utility Sotre,I‐10 Markaz 5 Al Rehmat enterprises Al rehmat market shops 01‐03 street no 4 koral town Islamabad 6 Office No. 6, First Floor, Malik Plaza, Block 16‐C, Upper Floor NRC F‐8, Islamabad 7 Friends Computers Shop no 9 basement Farhan Plaza G‐11 Markaz Islamabad 8 Arslan Hardware Electric & Paint Store machine stop Darkala road chowk Harno Thanda Pani Islamabad 9 Pakistan Town, Phase‐I near Lohi Bheer 10 Tariq Market F‐10/2. 11 Shop No. 1‐B Plot No. 2/A Pakeza Market I‐8/4 Islamabad 12 Hamza Card & Mobile, Saifullah Plaza, Rawat 13 Basement floor hajveri plaza 22‐b chaina chock blue area F‐6,G‐6 14 Adeel Mobile Shop & Call Customer Services Bharak Kahu 15 Main CDA Headquarters Building Compound 16 Aamir Communication Jabba UC Tarlai 17 Al‐Rehman Stationary Golra Sharif 18 Arsalan Customer Service, PCO, Nei Abadi Korang Sohan Warsi Market Islamabad. 19 Dhanyal Customer Near Police Station Service Simly Dam Road Near Barakahu. 20 Moh Usman Abad Near Masjid Abdullah Bin Zubair Bhara Kaho Islamabad 21 Village Chatta Bakhtawar Islamabad. 22 Shop No.8, Mughal Market, Irfanabad, P.O Tarlai Kalan, Taramri Chowk. 23 Main Bazar Sang Jani, Tehsil & Distt Islamabad 24 Village Farash Near Girls High School Federal Area Islamabad. -

Population Census of Pakistan 1961
( ·~ " POPULATION CENSUS OF PAKISTAN 1961 ~ DISTRICT CENSUS REPORT -RAWALPINDI PART-V rV lllAGE STATISJ.ics· 'COMPIL~D BY i<i-iA ·~ BASHIR AHMED KAAN 'ASSJSTANT DIRECTOR OF cENSUS Ri\WALPINoi ~ lt ~':"",.a;ll!;. mn=-rr:n INTRODUCTION The village is the ba sic unit of revenue The Village Statistics contained in this administration and the need for basic statis part have been compiled from Block-wise tics for villages is quite obvious as au plan fi gures contained in the Summaries prepared ning depends on such statistics. They are a lso by the Census Supervisors and Charge indispensable fo r carrying out sample surveys Superintendents. Except for data on houses over limited areas and form the basis of contin and houseJ10lds they are based on the results uous collection ofs tatistics on different aspects of the "Circle Sort"' which was carried out in of rural life and economy. The village was ta ken the Hand Sorting Centres after the physical as the basic unit of enumeration if its popula counting of the individual enumeration tion was 600 or it was a continuous collection schedules. The literacy figures, however, have of about 150 houses on an average. Where been lifted from the Summaries prepared by the village approximated to this size, it was the Supervisors and Charge Superintendents. constituted into a Block. A large nu mber of villages ha d to be split up into a number of The plan of presentati on is that for each Blocks, but the boundaries of Census Block village, the Hadbast number, its name in did not go beyond the limits of a revenue English and Urdu a nd a rea in acres, the estate. -
Audit Report
AUDIT REPORT ON THE ACCOUNTS OF CENTRAL ZAKAT FUND, ZAKAT COLLECTION CONTROLLING AGENCIES, ZAKAT COLLECTION OFFICES AND ISLAMABAD ZAKAT & USHR COMMITTEE AUDIT YEAR 2014-15 AUDITOR – GENERAL OF PAKISTAN TABLE OF CONTENTS ABBREVIATIONS & ACRONYMS ii PREFACE iii EXECUTIVE SUMMARY 1 SUMMARY OF TABLES & CHARTS 4 I Audit Work Statistics 5 II Audit Observations Regarding Financial Management 5 III Outcome Statistics 6 IV Irregularities Pointed Out 6 V Cost-Benefit 7 CHAPTER 1 CENTRAL ZAKAT FUND 8 1.1 Introduction 8 1.2 Comments on Budget & Accounts 9 1.3 Brief Comments on the Status of Compliance with PAC Directives 9 1.4 AUDIT PARAS 10 CHAPTER 2 ZAKAT COLLECTION CONTROLLING AGENCIES AND ZAKAT COLLECTION OFFICES 14 2.1 Introduction 14 2.2 Comments on Budget & Accounts 14 2.3 AUDIT PARAS 15 CHAPTER 3 ISLAMABAD ZAKAT & USHR COMMITTEE 25 3.1 Introduction 25 3.2 Comments on Budget & Accounts 26 3.3 Brief Comments on the Status of Compliance with PAC Directives 26 3.4 AUDIT PARAS 27 ANNEXURE 38 i ABBREVIATIONS & ACRONYMS AIR Audit & Inspection Report ACL Audit Command Language AG Accountant General AGPR Accountant General Pakistan Revenues CAZ Chief Administrator Zakat CZA Central Zakat Administration CZC Central Zakat Council CZF Central Zakat Fund CMA Controller Military Accounts CDRs Central Depository Receipts DAC Departmental Accounts Committee DAO District Accounts Office DHQ District Headquarter DSC Defense Saving Certificates DZA Directorate of Zakat Audit DZF District Zakat Fund FDRs Fixed Deposits Receipts GBZF Gilgit Baltistan Zakat Fund -

Public Sector Development Programme 2021-22
GOVERNMENT OF PAKISTAN PUBLIC SECTOR DEVELOPMENT PROGRAMME 2021-22 PLANNING COMMISSION MINISTRY OF PLANNING, DEVELOPMENT & SPECIAL INITIATIVES June, 2021 PREFACE Public Sector Development Programme (PSDP) is an important policy instrument aiming to achieve sustainable economic growth and socioeconomic objectives of the government. The outgoing fiscal year PSDP was made with a particular focus on strengthening the health sector and creating economic opportunities to combat widespread disruptions caused by COVID-19 pandemic. As a result of efficient and well-coordinated management of the pandemic, the economy showed signs of recovery and economic growth stood at 3.94% during FY 2020-21. In the upcoming year 2021-22, the priority of the Government is to further spur economic activities. Therefore, the PSDP in 2021-22 has been enhanced by 38% from Rs 650 billion in FY 2020-21 to Rs. 900 billion (including foreign aid of Rs 100 billion). The focus of PSDP 2021-22 is on improving transport and communication facilities with special emphasis on inter-provincial and regional connectivity, investment on building large dams and water conservation systems as per the National Water Policy, augmenting and strengthening health sector infrastructure and service delivery, improving access to higher education, social protection, increasing employment and livelihood opportunities, reducing regional disparities, mitigating effects of climate change, building knowledge economy, enhancing agricultural productivity & ensuring food security and supporting Public Private Partnership initiatives through providing Viability Gap funding. Special Development Packages have been initiated under the Regional Equalization Programme to ensure the development of the deprived areas to bring them at par with other developed regions of the country. -

UNESCO Final 003(Edited)
PAKISTAN BASELINE ASSESSMENT OF CURRENT SCENARIO OF PLASTIC WASTE MANAGEMENT ISLAMABAD CAPITAL TERRITORY (ICT) AND AYUBIA NATIONAL PARK (ANP) Copyright © 2019 UNESCO Islamabad Material in this report maybe reproduced for non-profit and academic purposes, provided due acknowledgement of the source is made. Disclaimer: The information contained herein is as per conditions during the time of survey and is shared in good faith. WWF-Pakistan or UNESCO will not be responsible for any legal action taken by anyone. Authors: Muhammad Hamza Abbas and Haider Ali - WWF-Pakistan Co-author: Misha Khan, WWF-Pakistan Editors: Dr Masood Arshad, -Nazifa Butt and Maryam Arshad - WWF-Pakistan Photo credits: © WWF-Pakistan Designed by Syeda Sadia Gilani, Sana Maqsood, Communications Department, WWF-Pakistan This report is available at: UNESCO Islamabad 7 th Floor, Serena Business Complex, Sector G-5/1, Islamabad, Pakistan Tel: +92-51-2600242 – 49 Fax: +92-51-2600250 Email: [email protected] Website: www.unesco.org.pk BASELINE ASSESSMENT OF CURRENT SCENARIO OF PLASTIC WASTE MANAGEMENT ISLAMABAD CAPITAL TERRITORY (ICT) AND AYUBIA NATIONAL PARK (ANP) Conducted by WWF-Pakistan November 2019 CONTENTS Foreword I Preface III List of Acronyms V Acknowledgements VII Executive Summary IX 1. Introduction 1 2. Methodology 3 2.1 Focus group discussions 3 2.2 Identification of scope areas 4 2.2.1 Islamabad Capital Territory 4 2.2.2 Ayubia National Park 6 2.3 Establishing a sample size for physical plastic waste assessment 6 2.3.1 Defining sample cycle for urban ICT